Surgical Evaluation and Management of Constipation Susanna S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

Utility of the Digital Rectal Examination in the Emergency Department: a Review
The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1196–1204, 2012 Published by Elsevier Inc. Printed in the USA 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2012.06.015 Clinical Reviews UTILITY OF THE DIGITAL RECTAL EXAMINATION IN THE EMERGENCY DEPARTMENT: A REVIEW Chad Kessler, MD, MHPE*† and Stephen J. Bauer, MD† *Department of Emergency Medicine, Jesse Brown VA Medical Center and †University of Illinois-Chicago College of Medicine, Chicago, Illinois Reprint Address: Chad Kessler, MD, MHPE, Department of Emergency Medicine, Jesse Brown Veterans Hospital, 820 S Damen Ave., M/C 111, Chicago, IL 60612 , Abstract—Background: The digital rectal examination abdominal pain and acute appendicitis. Stool obtained by (DRE) has been reflexively performed to evaluate common DRE doesn’t seem to increase the false-positive rate of chief complaints in the Emergency Department without FOBTs, and the DRE correlated moderately well with anal knowing its true utility in diagnosis. Objective: Medical lit- manometric measurements in determining anal sphincter erature databases were searched for the most relevant arti- tone. Published by Elsevier Inc. cles pertaining to: the utility of the DRE in evaluating abdominal pain and acute appendicitis, the false-positive , Keywords—digital rectal; utility; review; Emergency rate of fecal occult blood tests (FOBT) from stool obtained Department; evidence-based medicine by DRE or spontaneous passage, and the correlation be- tween DRE and anal manometry in determining anal tone. Discussion: Sixteen articles met our inclusion criteria; there INTRODUCTION were two for abdominal pain, five for appendicitis, six for anal tone, and three for fecal occult blood. -

The American Society of Colon and Rectal Surgeons' Clinical Practice
CLINICAL PRACTICE GUIDELINES The American Society of Colon and Rectal Surgeons’ Clinical Practice Guideline for the Evaluation and Management of Constipation Ian M. Paquette, M.D. • Madhulika Varma, M.D. • Charles Ternent, M.D. Genevieve Melton-Meaux, M.D. • Janice F. Rafferty, M.D. • Daniel Feingold, M.D. Scott R. Steele, M.D. he American Society of Colon and Rectal Surgeons for functional constipation include at least 2 of the fol- is dedicated to assuring high-quality patient care lowing symptoms during ≥25% of defecations: straining, Tby advancing the science, prevention, and manage- lumpy or hard stools, sensation of incomplete evacuation, ment of disorders and diseases of the colon, rectum, and sensation of anorectal obstruction or blockage, relying on anus. The Clinical Practice Guidelines Committee is com- manual maneuvers to promote defecation, and having less posed of Society members who are chosen because they than 3 unassisted bowel movements per week.7,8 These cri- XXX have demonstrated expertise in the specialty of colon and teria include constipation related to the 3 common sub- rectal surgery. This committee was created to lead inter- types: colonic inertia or slow transit constipation, normal national efforts in defining quality care for conditions re- transit constipation, and pelvic floor or defecation dys- lated to the colon, rectum, and anus. This is accompanied function. However, in reality, many patients demonstrate by developing Clinical Practice Guidelines based on the symptoms attributable to more than 1 constipation sub- best available evidence. These guidelines are inclusive and type and to constipation-predominant IBS, as well. The not prescriptive. -

OT Resource for K9 Overview of Surgical Procedures
OT Resource for K9 Overview of surgical procedures Prepared by: Hannah Woolley Stage Level 1 2 Gynecology/Oncology Surgeries Lymphadenectomy (lymph node dissection) Surgical removal of lymph nodes Radical: most/all of the lymph nodes in tumour area are removed Regional: some of the lymph nodes in the tumour area are removed Omentectomy Surgical procedure to remove the omentum (thin abdominal tissue that encases the stomach, large intestine and other abdominal organs) Indications for omenectomy: Ovarian cancer Sometimes performed in combination with TAH/BSO Posterior Pelvic Exenteration Surgical removal of rectum, anus, portion of the large intestine, ovaries, fallopian tubes and uterus (partial or total removal of the vagina may also be indicated) Indications for pelvic exenteration Gastrointestinal cancer (bowel, colon, rectal) Gynecological cancer (cervical, vaginal, ovarian, vulvar) Radical Cystectomy Surgical removal of the whole bladder and proximal lymph nodes In men, prostate gland is also removed In women, ovaries and uterus may also be removed Following surgery: Urostomy (directs urine through a stoma on the abdomen) Recto sigmoid pouch/Mainz II pouch (segment of the rectum and sigmoid colon used to provide anal urinary diversion) 3 Radical Vulvectomy Surgical removal of entire vulva (labia, clitoris, vestibule, introitus, urethral meatus, glands/ducts) and surrounding lymph nodes Indication for radical vulvectomy Treatment of vulvar cancer (most common) Sentinel Lymph Node Dissection (SLND) Exploratory procedure where the sentinel lymph node is removed and examined to determine if there is lymph node involvement in patients diagnosed with cancer (commonly breast cancer) Total abdominal hysterectomy/bilateral saplingo-oophorectomy (TAH/BSO) Surgical removal of the uterus (including cervix), both fallopian tubes and ovaries Indications for TAH/BSO: Uterine fibroids: benign growths in the muscle of the uterus Endometriosis: condition where uterine tissue grows on structures outside the uterus (i.e. -

Anorectal Disorders Satish S
Gastroenterology 2016;150:1430–1442 Anorectal Disorders Satish S. C. Rao,1 Adil E. Bharucha,2 Giuseppe Chiarioni,3,4 Richelle Felt-Bersma,5 Charles Knowles,6 Allison Malcolm,7 and Arnold Wald8 1Division of Gastroenterology and Hepatology, Augusta University, Augusta, Georgia; 2Department of Gastroenterology and Hepatology, Mayo College of Medicine, Rochester, Minnesota; 3Division of Gastroenterology of the University of Verona, Azienda Ospedaliera Universitaria Integrata di Verona, Verona, Italy; 4Division of Gastroenterology and Hepatology and UNC Center for Functional GI and Motility Disorders, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina; 5Department of Gastroenterology/Hepatology, VU Medical Center, Amsterdam, The Netherlands; 6National Centre for Bowel Research and Surgical Innovation, Blizard Institute, Queen Mary University of London, London, United Kingdom; 7Division of Gastroenterology, Royal North Shore Hospital, and University of Sydney, Sydney, Australia; 8Division of Gastroenterology, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin This report defines criteria and reviews the epidemiology, questionnaires and bowel diaries are correlated,5 some pathophysiology, and management of the following com- patients may not accurately recall bowel symptoms6; hence, mon anorectal disorders: fecal incontinence (FI), func- symptom diaries may be more reliable. tional anorectal pain, and functional defecation disorders. In this report, we examine the prevalence and patho- FI is defined as the recurrent uncontrolled passage of fecal physiology of anorectal disorders, listed in Table 1,and material for at least 3 months. The clinical features of FI provide recommendations for diagnostic evaluation and are useful for guiding diagnostic testing and therapy. management. These supplement practice guidelines rec- ANORECTAL Anorectal manometry and imaging are useful for evalu- ommended by the American Gastroenterological Associa- fl ating anal and pelvic oor structure and function. -

Intestine Transplant Manual
Intestine Transplant Manual Toronto Intestine Transplant Program TRANSPLANT MANUAL E INTESTIN This manual is dedicated to our donors, our patients and their families Acknowledgements Dr. Mark Cattral, MD, (FRCSC) Dr. Yaron Avitzur, MD Andrea Norgate, RN, BScN Sonali Pendharkar, BA (Hons), BSW, MSW, RSW Anna Richardson, RD We acknowledge the contribution of previous members of the team and to Cheryl Beriault (RN, BScN) for creating this manual. 2 TABLE OF CONTENTS Dedications and Acknowledgements 2 Welcome 5 Our Values and Philosophy of Care Our Expectations of You Your Transplant Team 6 The Function of the Liver and Intestines 9 Where are the abdominal organs located and what do they look like? What does your Stomach do? What does your Intestine do? What does your Liver do? What does your Pancreas do? When Does a Patient Need an Intestine Transplant? 12 Classification of Intestine Failure Am I Eligible for an Intestine Transplant? Advantages and Disadvantages of Intestine Transplant The Transplant Assessment 14 Investigations Consultations Active Listing for Intestine Transplantation (Placement on the List) 15 Preparing for the Intestine Transplant Trillium Drug Program Other Sources of Funding for Drug Coverage Financial Planning Insurance Issues Other Financial Considerations Related to the Hospital Stay Legal Considerations for Transplant Patients Advance Care Planning Waiting for the Intestine Transplant 25 Your Place on the Waiting List Maintaining Contact with the Transplant Team Coping with Stress Maintaining your Health While -

Information for Patients Having a Sigmoid Colectomy
Patient information – Pre-operative Assessment Clinic Information for patients having a sigmoid colectomy This leaflet will explain what will happen when you come to the hospital for your operation. It is important that you understand what to expect and feel able to take an active role in your treatment. Your surgeon will have already discussed your treatment with you and will give advice about what to do when you get home. What is a sigmoid colectomy? This operation involves removing the sigmoid colon, which lies on the left side of your abdominal cavity (tummy). We would then normally join the remaining left colon to the top of the rectum (the ‘storage’ organ of the bowel). The lines on the attached diagram show the piece of bowel being removed. This operation is done with you asleep (general anaesthetic). The operation not only removes the bowel containing the tumour but also removes the draining lymph glands from this part of the bowel. This is sent to the pathologists who will then analyse each bit of the bowel and the lymph glands in detail under the microscope. This operation can often be completed in a ‘keyhole’ manner, which means less trauma to the abdominal muscles, as the biggest wound is the one to remove the bowel from the abdomen. Sometimes, this is not possible, in which case the same operation is done through a bigger incision in the abdominal wall – this is called an ‘open’ operation. It does take longer to recover with an open operation but, if it is necessary, it is the safest thing to do. -

Constipation
Constipation Caris Diagnostics Health Improvement Series What is constipation? Constipation means that a person has three bowel movements or fewer in a week. The stool is hard and dry. Sometimes it is painful to pass. You may feel‘draggy’and full. Some people think they should have a bowel movement every day. That is not really true. There is no‘right’number of bowel movements. Each person's body finds its own normal number of bowel movements. It depends on the food you eat, how much you exercise, and other things. At one time or another, almost everyone gets constipated. In most cases, it lasts for a short time and is not serious. When you understand what causes constipation, you can take steps to prevent it. What can I do about constipation? Changing what you 4. Allow yourself enough time to have a bowel movement. eat and drink and how much you exercise will help re- Sometimes we feel so hurried that we don't pay atten- lieve and prevent constipation. Here are some steps you tion to our body's needs. Make sure you don't ignore the can take. urge to have a bowel movement. 1. Eat more fiber. Fiber helps form soft, bulky stool. It 5. Use laxatives only if a doctor says you should. is found in many vegetables, fruits, and grains. Be sure Laxatives are medicines that will make you pass a stool. to add fiber a little at a time, so your body gets used to Most people who are mildly constipated do not need it slowly. -

Enteroliths in a Kock Continent Ileostomy: Case Report and Review of the Literature
E200 Cases and Techniques Library (CTL) similar symptoms recurred 2 years later. A second ileoscopy showed a narrowed Enteroliths in a Kock continent ileostomy: efferent loop that was dilated by insertion case report and review of the literature of the colonoscope, with successful relief of her symptoms. Chemical analysis of one of the retrieved enteroliths revealed calcium oxalate crystals. Five cases have previously been noted in the literature Fig. 1 Schematic (●" Table 1). representation of a Kock continent The alkaline milieu of succus entericus in ileostomy. the ileum may induce the precipitation of a calcium oxalate concretion; in contrast, the acidic milieu found more proximally in the intestine enhances the solubility of calcium. The gradual precipitation of un- conjugated bile salts, calcium oxalate, and Valve calcium carbonate crystals around a nidus composed of fecal material or undigested Efferent loop fiber can lead to the formation of calcium oxalate calculi over time [5]. Endoscopy_UCTN_Code_CCL_1AD_2AJ Reservoir Competing interests: None Hadi Moattar1, Jakob Begun1,2, Timothy Florin1,2 1 Department of Gastroenterology, Mater Adult Hospital, South Brisbane, Australia The Kock continent ileostomy (KCI) was dure was done to treat ulcerative pan- 2 Mater Research, University of Queens- designed by Nik Kock, who used an intus- colitis complicated by colon cancer. She land, Translational Research Institute, suscepted ileostomy loop to create a nip- had a well-functioning KCI that she had Woolloongabba, Australia ple valve (●" Fig.1) that would not leak catheterized daily for 34 years before she and would allow ileal effluent to be evac- presented with intermittent abdominal uated with a catheter [1]. -
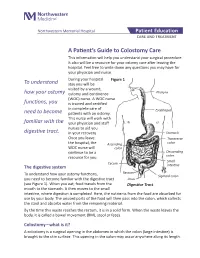
A Patient's Guide to Colostomy Care
Northwestern Memorial Hospital Patient Education CARE AND TREATMENT A Patient’s Guide to Colostomy Care This information will help you understand your surgical procedure. It also will be a resource for your ostomy care after leaving the hospital. Feel free to write down any questions you may have for your physician and nurse. During your hospital Figure 1 To understand stay you will be visited by a wound, how your ostomy ostomy and continence Pharynx (WOC) nurse. A WOC nurse functions, you is trained and certified in complete care of Esophagus need to become patients with an ostomy. This nurse will work with familiar with the your physician and staff nurses to aid you digestive tract. in your recovery. Stomach Once you leave Transverse the hospital, the Ascending colon WOC nurse will colon continue to be a Descending resource for you. colon Small Cecum The digestive system intestine Rectum To understand how your ostomy functions, Sigmoid colon you need to become familiar with the digestive tract Anus (see Figure 1). When you eat, food travels from the Digestive Tract mouth to the stomach. It then moves to the small intestine, where digestion is completed. Here, the nutrients from the food are absorbed for use by your body. The unused parts of the food will then pass into the colon, which collects the stool and absorbs water from the remaining material. By the time this waste reaches the rectum, it is in a solid form. When the waste leaves the body, it is called a bowel movement (BM), stool or feces. -

Reoperative Techniques and Management in Hirschsprung Disease: a Narrative Review
14 Review Article Reoperative techniques and management in Hirschsprung disease: a narrative review Farokh R. Demehri^, Belinda H. Dickie Department of Surgery, Boston Children’s Hospital, Boston, MA, USA Contributions: (I) Conception and design: All authors; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors Correspondence to: Farokh R. Demehri, MD. Department of Surgery, Boston Children’s Hospital, 300 Longwood Ave, Fegan 3, Boston, MA 02115, USA. Email: [email protected]. Abstract: The majority of children who undergo operative management for Hirschsprung disease have favorable results. A subset of patients, however, have long-term dysfunctional stooling, characterized by either frequent soiling or obstructive symptoms. The evaluation and management of a child with poor function after pull-through for Hirschsprung disease should be conducted by an experienced multidisciplinary team. A systematic workup is focused on detecting pathologic and anatomic causes of pull- through dysfunction. This includes an exam under anesthesia, pathologic confirmation including a repeat biopsy, and a contrast enema, with additional studies depending on the suspected etiology. Obstructive symptoms may be due to technique-specific types of mechanical obstruction, histopathologic obstruction, or dysmotility—each of which may benefit from reoperative surgery. The causes of soiling symptoms include loss of the dentate line and damage to the anal sphincter, which generally do not benefit from revision of the pull-through, and pseudo-incontinence, which may reveal underlying obstruction. A thorough understanding of the types of complications associated with various pull-through techniques aids in the evaluation of a child with postoperative dysfunction. -

High Quality Fecal Occult Blood Testing (FOBT) for CRC Screening: Evidence and Recommendations
High Quality Fecal Occult Blood Testing (FOBT) for CRC Screening: Evidence and Recommendations Rationale for use of FOBT High sensitivity fecal occult blood testing (FOBT) is one of the colorectal cancer screening methods recommended in guidelines from the American Cancer Society, the US Preventive Services Taskforce, and every other major medical organization. In spite of this widespread endorsement, primary care clinicians often express conviction that colonoscopy is the “gold standard” test for colorectal cancer screening and that the use of FOBT represents sub-standard care. These beliefs persist in spite of well-documented shortcomings of endoscopy (missed adenomas and cancers, higher complication rates and higher one-time costs than other screening methodologies), and the fact that access to endoscopy is limited or non- existent for a significant proportion of the U.S. population. Many clinicians are also unaware that randomized controlled trials of FOBT screening have demonstrated decreases in colorectal cancer incidence and mortality, and modeling studies suggest that the years of life saved through a high quality FOBT screening program are essentially the same as with a high quality colonoscopy based screening programs. Recent advances in stool blood screening include the emergence of new tests and improved understanding of the impact of quality factors on testing outcomes. This document provides state-of-the-science information about high quality stool testing. Types of Fecal Occult Blood Tests Two main types of FOBT are available – guaiac and immunochemical. Both types of FOBT have been shown to have reasonably high detection rates for colon and rectal cancers; adenoma detection rates are appreciably lower.