Photodocumentation in the Investigation of Child Abuse
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Photography and Video Policy: to Govern Clinical and Non-Clinical Recordings
PAT/PA 14 v.4 Photography and Video Policy: to Govern Clinical and Non-clinical Recordings This procedural document supersedes: PAT/PA 14 v.3 – Photography and Video Policy: to Govern Clinical and Non-clinical Recordings Did you print this document yourself? The Trust discourages the retention of hard copies of policies and can only guarantee that the policy on the Trust website is the most up-to-date version. If, for exceptional reasons, you need to print a policy off, it is only valid for 24 hours. Author/reviewer: (this Tim Vernon - Head of Medical Photography and version) Graphic Design Roy Underwood - Head of Information Governance & Registration Authority Manager Date written/revised: 20.08.2013 Approved by: Information Governance Group Date of approval: 09 September 2013 Date issued: 12 November 2013 Next review date: 09 September 2016 Target audience: Trust-wide Page 1 of 32 PAT/PA 14 v.4 Amendment Form Please record brief details of the changes made alongside the next version number. If the procedural document has been reviewed without change, this information will still need to be recorded although the version number will remain the same. Version Date Brief Summary of Changes Author Issued Version 4 12 Nov • Amendment to section 5.3 - about the Tim Vernon 2013 copyright of images found on the Internet • Amendment to section 5.5 - about the registration of photography & video equipment with MPGD and its safe storage. Version 3 November • Reformatted to meet new style format Tim Vernon 2012 as per Trust policy CORP/COMM 1 • References updated • Appendices updated and re-designed • Appendix 4 and 5 added Version 2 January ‘Dolphin Imaging System in Orthodontics’ Tim Vernon (minor 2012 added to section 10. -
ASSESSING MEDICAL PHOTOGRAPHY EQUIPMENT a Guide to Available Technology and Its Potential Benefits
COVER FOCUS ASSESSING MEDICAL PHOTOGRAPHY EQUIPMENT A guide to available technology and its potential benefits. BY EMILY ALTEN Emily Alten is a writing enthusiast and biology nerd who specializes in educational healthcare and medicine content for RxPhoto. She is a Magna Cum Laude graduate from Columbia University with a degree in biological sciences/pre-medical studies. RxPhoto’s medical app converts an iPhone or an iPad into a clinical photography system securely capturing, managing, and sharing patient photos and videos. RxPhoto.com ithout a doubt, you need to take photos of your anatomical region. Most physicians set up a photography patients on a daily basis. Whether you’re building room specifically for using these types of cameras. a before and after portfolio for marketing or using photography for procedure tracking, you want MOBILE DEVICES Wyour pictures to look clean and consistent. Very few offices have Because of the upfront cost of the other options, it’s no a skilled photographer on staff, so it can be difficult to decide on surprise that many doctors are using mobile devices, such as the best camera to use. Ahead, we profile the pros and cons of tablets and smartphones, especially since the quality of mobile the three most common options for aesthetic photography. device cameras has been improving at a staggering pace. DSLR MOBILE DEVICES VERSUS DSLR Many physicians choose a DSLR camera for their clinical Smartphone and tablet cameras are often just as good, if photography, and most set up a dedicated photography not better, than standard point-and-shoot digital cameras. -

Hysteria in the Lens of Nineteenth Century Medical Photography
11 EXPOSURE, NEGATIVE, PROOF: HYSTERIA IN THE LENS OF NINETEENTHCENTURY MEDICAL PHOTOGRAPHY M ICHAEL P. V ICARO P ENNS YLVANIA STATE U NIVERS ITY—G REATER A LLEGHENY This article explores the role of photography in the and forcing things in the world to present themselves in cultural production of “hysteria” in the nineteenth-cen- a manner that could be seen, analyzed, and thereby con- tury, arguing that image-making technologies deeply trolled (Heidegger 1938). Photography, introduced into shaped public perceptions of deviance and normality. a flourishing culture of scientific empiricism, helped to Late nineteenth-century hysteria can be described as a satisfy and to amplify the desire for vantage points from uniquely “photogenic” ailment— literally produced and which one might witness and dutifully record without bias developed by the light of the camera flash. Art historians the magnitude and minutia of life (Peters 2005). In early have studied the photographic history of hysteria (Didi- texts, the processes of daguerreotypy and photography Huberman 2003; Koehler 2001; Schade 1995; Gilman were routinely called “discoveries” rather than “inventions,” 1982). But media scholars have largely ignored the way suggesting that they were natural phenomenon harnessed images of hysteria functioned as a series of visual argu- by human hands (Marien 2002). In Daguerre’s words, “the ments about the “normal” bourgeois, white, feminine body. daguerreotype is not an instrument which serves to draw Conversely, those whose work has situated hysteria in the nature; but a chemical and physical process which gives larger context of the formation of the modern body have her the power to reproduce herself ” (qtd. -

Photographing Fluorescent Minerals with Mineralight and Blak-Ray
Application Bulletin UVP-AB-120 Corporate Headquarters: UVP, Inc. European Operations: Ultra-Violet Products Limited 2066 W. 11th Street, Upland, CA 91786 USA Unit 1, Trinity Hall Farm Estate, Nuffield Road Telephone: (800)452-6788 or (909)946-3197 Cambridge CB4 1TG UK Telephone: 44(0)1223-420022 E-Mail: [email protected] E-Mail: [email protected] PHOTOGRAPHING FLUORESCENT MINERALS WITH MINERALIGHT AND BLAK-R AY LAMPS Taking pictures in ultraviolet light of fluorescent minerals is a relatively simple operation if one follows certain basic requirements and understands the several variables that control what is obtained on the picture. There are several factors that control obtaining the best picture and among these are the size of power of the ultraviolet light source, the distance of the light source to the subject, the type of film used, the fluorescent color of the mineral specimen, the type of filter on the camera, and the final exposure of the picture. These subjects are taken up below in orde r. The size of the light source will make a difference as far as the picture is concerned because the more powerful the light source, the shorter the exposure. The distance of the ultraviolet light to the subject is also of great importance for the closer the light source is to the subject being photographed, the brighter the fluorescence will be and the shorter exposure required. While tubular light sources do not vary according to the so-called square la w, never- theless, moving the light source into one-half of its original distance will more than double the light intensity with corresponding increase in fluorescent brightness. -
Reflected Ultraviolet (Modified Camera)
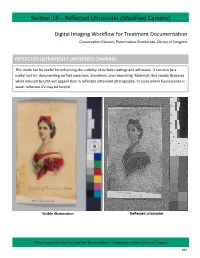
Section 18—Reflected Ultraviolet (Modified Camera) Digital Imaging Workflow for Treatment Documentation Conservation Division, Preservation Directorate, Library of Congress REFLECTED ULTRAVIOLET (MODIFIED CAMERA) This mode can be useful for enhancing the visibility of surface coatings and adhesives. It can also be a useful tool for documenting surface abrasions, accretions, and retouching. Materials that visably fluoresce when induced by UVA will appear dark in reflected ultraviolet photography. In cases where fluorescence is weak, reflected UV may be helpful. Visible illumination Reflected ultraviolet Digital Imaging Workflow for Treatment Documentation—Conservation Division, Library of Congress 18.1 Section 18—Reflected Ultraviolet (Modified Camera) Figure 18.01 Figure 18.02 Figure 18.03 Digital Imaging Workflow for Treatment Documentation—Conservation Division, Library of Congress 18.2 Section 18—Reflected Ultraviolet (Modified Camera) Capture Preliminary If not done already, capture a visible illumination image with the modified camera following instructions in Section 14. Wear UV goggles when the UV lights are on. Set Up 1. Use the Nikon D700 modified camera and the CoastalOpt lens. 2. The CoastalOpt lens MUST be set at the minimum aperture setting of f/45 to utilize the electronic aperture function (otherwise the camera will display FEE). 3. The PECA 900 and X-Nite BP1 filters are used for reflected ultraviolet photography with the modified camera (fig 18.01). The filters are stored in the studio cabinet. Very carefully, screw on both filters to the end of the camera lens. The order the filters are screwed on does not matter. 4. Plug in the UV lamps. It is important to plug in both cords (two for each lamp) for at least 20 seconds before switching on lamps. -
Introduction to Photography
Edited with the trial version of Foxit Advanced PDF Editor To remove this notice, visit: www.foxitsoftware.com/shopping Introduction to Photography Study Material for Students : Introduction to Photography CAREER OPPORTUNITIES IN MEDIA WORLD Mass communication and Journalism is institutionalized and source specific. It functions through well-organized professionals and has an ever increasing interlace. Mass media has a global availability and it has converted the whole world in to a global village. A qualified journalism professional can take up a job of educating, entertaining, informing, persuading, interpreting, and guiding. Working in print media offers the opportunities to be a news reporter, news presenter, an editor, a feature writer, a photojournalist, etc. Electronic media offers great opportunities of being a news reporter, news Edited with the trial version of editor, newsreader, programme host, interviewer, cameraman,Foxit Advanced producer, PDF Editor To remove this notice, visit: director, etc. www.foxitsoftware.com/shopping Other titles of Mass Communication and Journalism professionals are script writer, production assistant, technical director, floor manager, lighting director, scenic director, coordinator, creative director, advertiser, media planner, media consultant, public relation officer, counselor, front office executive, event manager and others. 2 : Introduction to Photography INTRODUCTION The book will introduce the student to the techniques of photography. The book deals with the basic steps in photography. Students will also learn the different types of photography. The book also focuses of the various parts of a photographic camera and the various tools of photography. Students will learn the art of taking a good picture. The book also has introduction to photojournalism and the basic steps of film Edited with the trial version of development in photography. -

10 Tips for Better Patient Care and Better Business
The Dermatologist’s Guide to Effective Clinical Photography 10 Tips for Better Patient Care and Better Business Photography has become essential to the practice of dermatology and aesthetic surgery. It provides a mechanism to improve patient care, enrich your documentation, aid in patient education/consultation, and allow you to set realistic expectations for your patients through the use of “before and after” images for cosmetic procedures. Despite the power of great photography, most medical practitioners find it difficult to capture high quality images. Consis- tent lighting, as well as camera and subject placement is critical to taking the quality photos that can showcase your skills and expand your practice. We have compiled ten invaluable tips to help you and your office achieve the best photographic results possible. Put a mark on the floor where the photog- of the distal cheek. This will help your pre- and Stand your ground. ▪ 1 rapher should stand. Try to keep the camera post-treatment images maintain consistency for successful comparisons. Many photographers stand too close to their over this line to maintain the distance. subjects, which may create distortion in the Photographing extreme close-ups Perspective is also important in non-clinical image. Additionally, at a short distance, the For extreme close-ups, special equipment is situations. The effects of laser and cosmetic bright flash from most cameras will overex- often required. The macro mode on a point- treatments can be effectively documented pose or “wash out” the center of the picture. It’s and-shoot camera, or a macro lens on a digital with consistent patient positioning. -

Medical Photography Guidelines 2006
Medical Photography Guidelines 2006 Harborview Center for Sexual Assault and Traumatic Stress If visible injuries are present, photography with digital, 35mm, specialized Polaroid, or video camera assists in documentation GENERAL Each camera type has advantages and limitations. − Polaroid photos generally have poor color and preservation − Video should have no sound recording unless all parties are aware of and consent 1 Careful documentation with drawing is mandatory even when photographs are obtained Each institution should take appropriate steps to maintain the privacy and dignity of the patient in photos Always document name of photographer and date of photos This may be done by documentation in the chart, in a photo log, or by writing the photographer name and date on the patient identification label which is then photographed TECHNIQUE Staff must be trained in specific camera and photography techniques If date function is used, verify that date is correct Check flash function: photos may be better either with or without flash First photo is of patient identification label One photo should include patient face Photograph each injury site 3 times First, from at least 3 feet away, to demonstrate the injury in context Second, close up Third, close up with a measuring device (ruler, coin, or ABFO rule) BODY PHOTOS Photos of body injury are as significant as genital injury in sexual assault cases Drape patient appropriately, photos may be shown in open court Hospital personnel may either take the photos or assist law enforcement -

Redalyc.Technical Photography for Mural Paintings: the Newly
Conservar Património E-ISSN: 2182-9942 [email protected] Associação Profissional de Conservadores Restauradores de Portugal Portugal Cosentino, A.; Gil, M.; Ribeiro, M.; Di Mauro, R. Technical photography for mural paintings: the newly discovered frescoes in Aci Sant’Antonio (Sicily, Italy) Conservar Património, núm. 20, diciembre, 2014, pp. 23-33 Associação Profissional de Conservadores Restauradores de Portugal Lisboa, Portugal Available in: http://www.redalyc.org/articulo.oa?id=513651365003 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Article / Artigo Technical photography for mural paintings: the newly discovered frescoes in Aci Sant’Antonio (Sicily, Italy) A. Cosentino1,* M. Gil2 M. Ribeiro3 R. Di Mauro4 1 Cultural Heritage Science Open Source, Piazza Cantarella, 11 Aci Sant’Antonio, 95025, Italy 2 Hercules Laboratory, Évora University, Palácio do Vimioso 8, 7000-809 Évora, Portugal 3 Professional photographer ( freelancer) 4 Professional architect (freelancer) * [email protected] Abstract Keywords A cycle of 18th century frescoes, depicting the last days of Christ on earth, were recently discovered Panoramic photography in Aci Sant’Antonio (Sicily, Italy). The paintings survive along the corners of an originally square Infrared photography chapel that was altered in the early 20th century, acquiring the current octagonal plan. This Ultraviolet photography paper presents the results of the technical photography documentation of these wall paintings Raking light photography and illustrates the methodological challenges that were posed during their examination. Raking Infrared false color light photography was used to reveal the paintings’ state of conservation, details of the plaster Mural paintings work and painting techniques. -

Effects of Light on Materials in Collections
Effects of Light Effects on Materials in Collections Data on Photoflash and Related Sources Schaeffer T. Terry The Getty Conservation Institute research in conservation GCI Effects of Light on Materials in Collections Schaeffer research in conservation The Getty Conservation Institute Effects of Light on Materials in Collections Data on Photoflash and Related Sources Terry T. Schaeffer 2001 Dinah Berland: Editorial Project Manager Elizabeth Maggio: Manuscript Editor Anita Keys: Production Coordinator Hespenheide Design: Designer Printed in the United States of America 10 9 8 7 6 5 4 3 2 © 2001 The J. Paul Getty Trust Second printing 2002 Getty Publications 1200 Getty Center Drive, Suite 500 Los Angeles, California 90049–1682 www.getty.edu The Getty Conservation Institute The Getty Conservation Institute works internationally to advance conservation in the visual arts. The Institute serves the conservation community through scientific research, education and training, model field projects, and the dissemination of information. The Institute is a program of the J. Paul Getty Trust, an international cultural and philanthropic institution devoted to the visual arts and the humanities. Research in Conservation The Research in Conservation reference series presents the findings of research conducted by the Getty Conservation Institute and its individual and institutional research partners, as well as state-of-the-art reviews of conservation literature. Each volume covers a topic of current interest to conservators and conservation scientists. Other volumes in the Research in Conservation series include Biodeterioration of Stone in Tropical Environments: An Overview (Kumar and Kumar 1999); Inert Gases in the Control of Museum Insect Pests (Selwitz and Maekawa 1998); Oxygen-Free Museum Cases (Maekawa 1998); Accelerated Aging: Photochemical and Thermal Aspects (Feller 1994); Airborne Particles in Museums (Nazaroff, Ligoki, et al. -

UV and IR Photography
UV & IR PHOTOGRAPHY IN FORENSIC SCIENCE INTRODUCTION • Ultraviolet and infrared have valuable application in law enforcement photography. • Photography utilizing these radiations may provide information about an object or material which cannot be obtained by other photographic methods. Either or both could be considered as part of a physical examination in cases where visual examination or photography by normal processes fail. • The visible spectrum ranges from blue at 400nm to red at 700nm.Ultraviolet wavelengths are shorter than 400nm and infrared wavelengths are longer than 700nm. • They provide us with no visual response and therefore are not considered to be light. Certain narrow bands of this invisible radiation, however, have practical photographic applications. • All standard photographic papers and photographic films are sensitive to UV. They are not, however, sensitive to infrared. Special film, sensitized to infrared radiations, is required for infrared photography. This infrared film is also sensitive to blue-violet and to ultraviolet. • Developing and printing techniques are similar to the normal processes for both ultraviolet and infrared photography. • The good thing is that both processes are non- destructive to inanimate objects. For life forms, the usual precautions regarding exposure to the eyes should be heeded. In cases of uncertainty as to which technique might produce the best results, you may have to try all. ULTRAVIOLET PHOTOGRAPHY • Ultraviolet Radiation • For practical photographic purposes we use only the long wave ultraviolet band. • Long wave ultraviolet :- 320 to 400 nanometres. • This band is transmitted by regular optical glass, of which most photographic lenses are made and, therefore, is of most practical value in ultraviolet photography. -

On Photography, Trans Visibility, and Legacies of the Clinic
arts Article Condition Verified: On Photography, Trans Visibility, and Legacies of the Clinic Chase Joynt 1,* and Emmett Harsin Drager 2 1 The Department of Gender Studies, University of Victoria, Victoria, BC V8P 5C2, Canada 2 Department of American Studies & Ethnicity, University of Southern California, Los Angeles, CA 90089, USA; [email protected] * Correspondence: [email protected] Received: 1 September 2019; Accepted: 31 October 2019; Published: 13 November 2019 Abstract: We approach this paper with a shared investment in historical and contemporary representations of trans and gender non-conforming people, and our individual research in the archives of early US Gender Clinics. Together, we consider what is at stake—or what might be possible—when we connect legacies of photography used as diagnostic tools in gender clinics with snapshots of early, community-based gatherings, and the presence of trans people in contemporary art. From the archives of Robert J. Stoller and photos of Casa Susanna, to the collaborative photography of Zackary Drucker and Amos Mac, and the biometric data art-theory experiments of Zach Blas, we engage a series of image-based projects, which animate underlying questions and socio-political debates about the politics of visuality, and visibility’s impact on trans and gender non-conforming people. Moreover, we argue that rhetorical strategies of proof—from conditions verified in clinics to shared existence through photography—are tethered to, and thus trapped by, the logics and discipline of legibility and re-institutionalization. Keywords: gender clinics; photography; transgender; Robert J. Stoller; visibility; opacity; Casa Susanna; Zackary Drucker; Amos Mac 1. Preface A photograph is a secret about a secret.