Pharmacogenomics and Improving Patient Care Rob Leffler, R.Ph
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinical Pharmacology 1: Phase 1 Studies and Early Drug Development
Clinical Pharmacology 1: Phase 1 Studies and Early Drug Development Gerlie Gieser, Ph.D. Office of Clinical Pharmacology, Div. IV Objectives • Outline the Phase 1 studies conducted to characterize the Clinical Pharmacology of a drug; describe important design elements of and the information gained from these studies. • List the Clinical Pharmacology characteristics of an Ideal Drug • Describe how the Clinical Pharmacology information from Phase 1 can help design Phase 2/3 trials • Discuss the timing of Clinical Pharmacology studies during drug development, and provide examples of how the information generated could impact the overall clinical development plan and product labeling. Phase 1 of Drug Development CLINICAL DEVELOPMENT RESEARCH PRE POST AND CLINICAL APPROVAL 1 DISCOVERY DEVELOPMENT 2 3 PHASE e e e s s s a a a h h h P P P Clinical Pharmacology Studies Initial IND (first in human) NDA/BLA SUBMISSION Phase 1 – studies designed mainly to investigate the safety/tolerability (if possible, identify MTD), pharmacokinetics and pharmacodynamics of an investigational drug in humans Clinical Pharmacology • Study of the Pharmacokinetics (PK) and Pharmacodynamics (PD) of the drug in humans – PK: what the body does to the drug (Absorption, Distribution, Metabolism, Excretion) – PD: what the drug does to the body • PK and PD profiles of the drug are influenced by physicochemical properties of the drug, product/formulation, administration route, patient’s intrinsic and extrinsic factors (e.g., organ dysfunction, diseases, concomitant medications, -
An Update on ABCB1 Pharmacogenetics
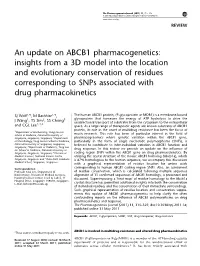
The Pharmacogenomics Journal (2011) 11, 315–325 & 2011 Macmillan Publishers Limited. All rights reserved 1470-269X/11 www.nature.com/tpj REVIEW An update on ABCB1 pharmacogenetics: insights from a 3D model into the location and evolutionary conservation of residues corresponding to SNPs associated with drug pharmacokinetics SJ Wolf1,6, M Bachtiar1,6, The human ABCB1 protein, (P-glycoprotein or MDR1) is a membrane-bound 1 2 3 glycoprotein that harnesses the energy of ATP hydrolysis to drive the J Wang , TS Sim , SS Chong unidirectional transport of substrates from the cytoplasm to the extracellular 1,4,5 and CGL Lee space. As a large range of therapeutic agents are known substrates of ABCB1 protein, its role in the onset of multidrug resistance has been the focus of 1Department of Biochemistry, Yong Loo Lin School of Medicine, National University of much research. This role has been of particular interest in the field of Singapore, Singapore, Singapore; 2Department pharmacogenomics where genetic variation within the ABCB1 gene, of Microbiology, Yong Loo Lin School of Medicine, particularly in the form of single nucleotide polymorphisms (SNPs), is National University of Singapore, Singapore, believed to contribute to inter-individual variation in ABCB1 function and Singapore; 3Department of Pediatrics, Yong Loo Lin School of Medicine, National University of drug response. In this review we provide an update on the influence of Singapore, Singapore, Singapore; 4Division of coding region SNPs within the ABCB1 gene on drug pharmacokinetics. By Medical Sciences, National Cancer Centre, utilizing the crystal structure of the mouse ABCB1 homolog (Abcb1a), which Singapore, Singapore and 5Duke-NUS Graduate is 87% homologous to the human sequence, we accompany this discussion Medical School, Singapore, Singapore with a graphical representation of residue location for amino acids Correspondence: corresponding to human ABCB1 coding region SNPs. -

Absolute Bioavailability and Dose-Dependent Pharmacokinetic Behaviour Of
Downloaded from https://www.cambridge.org/core British Journal of Nutrition (2008), 99, 559–564 doi: 10.1017/S0007114507824093 q The Authors 2007 Absolute bioavailability and dose-dependent pharmacokinetic behaviour of . IP address: dietary doses of the chemopreventive isothiocyanate sulforaphane in rat 170.106.202.8 Natalya Hanlon1, Nick Coldham2, Adriana Gielbert2, Nikolai Kuhnert1, Maurice J. Sauer2, Laurie J. King1 and Costas Ioannides1* 1Molecular Toxicology Group, School of Biomedical and Molecular Sciences, University of Surrey, Guildford, , on Surrey GU2 7XH, UK 30 Sep 2021 at 18:04:41 2TSE Molecular Biology Department, Veterinary Laboratories Agency Weybridge, Woodham Lane, New Haw, Addlestone, Surrey KT15 3NB, UK (Received 29 March 2007 – Revised 12 July 2007 – Accepted 25 July 2007) , subject to the Cambridge Core terms of use, available at Sulforaphane is a naturally occurring isothiocyanate with promising chemopreventive activity. An analytical method, utilising liquid chromatog- raphy-MS/MS, which allows the determination of sulforaphane in small volumes of rat plasma following exposure to low dietary doses, was devel- oped and validated, and employed to determine its absolute bioavailability and pharmacokinetic characteristics. Rats were treated with either a single intravenous dose of sulforaphane (2·8 mmol/kg) or single oral doses of 2·8, 5·6 and 28 mmol/kg. Sulforaphane plasma concentrations were determined in blood samples withdrawn from the rat tail at regular time intervals. Following intravenous administration, the plasma profile of sulforaphane was best described by a two-compartment pharmacokinetic model, with a prolonged terminal phase. Sulforaphane was very well and rapidly absorbed and displayed an absolute bioavailability of 82 %, which, however, decreased at the higher doses, indicating a dose-dependent pharmacokinetic behaviour; similarly, Cmax values did not rise proportionately to the dose. -

Importance of ADME and Bioanalysis in the Drug Discovery
alenc uiv e & eq B io io B a f v o a i l l a Journal of a b Vuppala et al., J Bioequiv Availab 2013, 5:4 n r i l i u t y o DOI: 10.4172/jbb.10000e31 J ISSN: 0975-0851 Bioequivalence & Bioavailability EditorialResearch Article OpenOpen Access Access Importance of ADME and Bioanalysis in the Drug Discovery Pradeep K Vuppala1*, Dileep R Janagam2 and Pavan Balabathula2 1Preclinical Pharmacokinetics Shared Resource, St. Jude Children’s Research Hospital, Memphis, TN, USA 2University of Tennessee Health Sciences Center, Memphis, TN, USA Editorial Bioanalytical support plays a vital role during the lead optimization stages. The major goal of the bioanalysis is to assess the over-all The hunt for new drugs can be divided into two stages: discovery ADME characteristics of the new chemical entities (NCE’s). Arrays and development. Drug discovery includes generating a hypothesis of of bioanalytical methods are required to completely describe the the target receptor for a particular disorder and screening the in vitro pharmacokinetic behavior in laboratory animals as well as in humans and/or in vivo biological activities of the new drug candidates. Drug [7]. Bioanalytical tools can play a significant role for the progress development involves the assessment of efficacy and toxicity of the new in drug discovery and development. Physiologic fluids such as blood, drug candidates. serum, plasma, urine and tissues are analyzed to determine the absorption and disposition of a drug candidate administered to a test To aid in a discovery program, accurate data on pharmacokinetics animal [8]. -

Intestinal Permeability and Drug Absorption: Predictive Experimental, Computational and in Vivo Approaches
pharmaceutics Review Intestinal Permeability and Drug Absorption: Predictive Experimental, Computational and In Vivo Approaches David Dahlgren and Hans Lennernäs * Department of Pharmacy, Uppsala University, Box 580 SE-751 23 Uppsala, Sweden * Correspondence: [email protected]; Tel.: +46-18-471-4317; Fax: +46-18-471-4223 Received: 2 July 2019; Accepted: 7 August 2019; Published: 13 August 2019 Abstract: The main objective of this review is to discuss recent advancements in the overall investigation and in vivo prediction of drug absorption. The intestinal permeability of an orally administered drug (given the value Peff) has been widely used to determine the rate and extent of the drug’s intestinal absorption (Fabs) in humans. Preclinical gastrointestinal (GI) absorption models are currently in demand for the pharmaceutical development of novel dosage forms and new drug products. However, there is a strong need to improve our understanding of the interplay between pharmaceutical, biopharmaceutical, biochemical, and physiological factors when predicting Fabs and bioavailability. Currently, our knowledge of GI secretion, GI motility, and regional intestinal permeability, in both healthy subjects and patients with GI diseases, is limited by the relative inaccessibility of some intestinal segments of the human GI tract. In particular, our understanding of the complex and highly dynamic physiology of the region from the mid-jejunum to the sigmoid colon could be significantly improved. One approach to the assessment of intestinal permeability is to use animal models that allow these intestinal regions to be investigated in detail and then to compare the results with those from simple human permeability models such as cell cultures. -

The Ethical, Legal and Social Implications of Pharmacogenomics in Developing Countries
The Ethical, Legal and Social Implications of Pharmacogenomics in Developing Countries Report of an International Group of Experts Human Genetics Chronic Diseases and Health Promotion WHO Library CataloguinginPublication Data The ethical, legal and social implications of pharmacogenomics in developing countries : report of an international group of experts. "Preparation of this report was undertaken by Human Genetics, headed by Victor Boulyjenkov. Cathy Schapper (Monash University) had principal responsibility for researching, writing and editing the report ..."Acknowledgements. 1.Pharmacogenetics ethics. 2.Pharmacogenetics legislation. 3.Ethics, Pharmacy. 4.Patient rights. 5.Socioeconomic factors. 6.Legislation, Drug. 7.Developing countries. I.Boulyjenkov, Victor. II.Schapper, Cathy. III.World Health Organization. ISBN 978 92 4 159546 9 (NLM classification: QV 38) © World Health Organization 2007 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; email: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. -

Pharmacogenomics to Predict Tumor Therapy Response: a Focus on ATP-Binding Cassette Transporters and Cytochromes P450
Journal of Personalized Medicine Review Pharmacogenomics to Predict Tumor Therapy Response: A Focus on ATP-Binding Cassette Transporters and Cytochromes P450 Viktor Hlaváˇc 1,2,* , Petr Holý 1,2,3 and Pavel Souˇcek 1,2 1 Toxicogenomics Unit, National Institute of Public Health, 100 00 Prague, Czech Republic; [email protected] (P.H.); [email protected] (P.S.) 2 Laboratory of Pharmacogenomics, Biomedical Center, Faculty of Medicine in Pilsen, Charles University, 306 05 Pilsen, Czech Republic 3 Third Faculty of Medicine, Charles University, 100 00 Prague, Czech Republic * Correspondence: [email protected]; Tel.: +420-267082681; Fax: +420-267311236 Received: 31 July 2020; Accepted: 26 August 2020; Published: 28 August 2020 Abstract: Pharmacogenomics is an evolving tool of precision medicine. Recently,due to the introduction of next-generation sequencing and projects generating “Big Data”, a plethora of new genetic variants in pharmacogenes have been discovered. Cancer resistance is a major complication often preventing successful anticancer treatments. Pharmacogenomics of both somatic mutations in tumor cells and germline variants may help optimize targeted treatments and improve the response to conventional oncological therapy. In addition, integrative approaches combining copy number variations and long noncoding RNA profiling with germline and somatic variations seem to be a promising approach as well. In pharmacology, expression and enzyme activity are traditionally the more studied aspects of ATP-binding cassette transporters and cytochromes P450. In this review, we briefly introduce the field of pharmacogenomics and the advancements driven by next-generation sequencing and outline the possible roles of genetic variation in the two large pharmacogene superfamilies. -
Bioavailability and Bioequivalence Studies Submitted in Ndas Or Inds — General Considerations
Guidance for Industry Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs — General Considerations DRAFT GUIDANCE This guidance document is being distributed for comment purposes only. Comments and suggestions regarding this draft document should be submitted within 60 days of publication in the Federal Register of the notice announcing the availability of the draft guidance. Submit electronic comments to http://www.regulations.gov. Submit written comments to the Division of Dockets Management (HFA-305), Food and Drug Administration, 5630 Fishers Lane, rm. 1061, Rockville, MD 20852. All comments should be identified with the docket number listed in the notice of availability that publishes in the Federal Register. For questions regarding this draft document contact the CDER Office of Clinical Pharmacology at 301-796-5008 or [email protected]. U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) March 2014 Biopharmaceutics Guidance for Industry Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs— General Considerations Additional copies are available from: Office of Communications Division of Drug Information, WO51, Room 2201 Center for Drug Evaluation and Research Food and Drug Administration 10903 New Hampshire Avenue, Silver Spring, MD 20993 http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/default.htm Phone: 301-796-3400; Fax: 301-847-8714 [email protected] U.S. Department of Health and Human Services Food -

Molecular Targets of Pepper As Bioavailability Enhancer
OPEM www.opem.org Oriental Pharmacy and Experimental Medicine 2009 9(4), 269-276 DOI 10.3742/OPEM.2009.9.4.269 Molecular targets of pepper as bioavailability enhancer Priyanshee Gohil and Anita Mehta* Department of Pharmacology, LM College of Pharmacy, Navrangpura, Ahmedabad–380009, Gujarat, India Received for publication January 21, 2008; accepted March 20, 2009 SUMMARY Black pepper (family Piperaceae), is called king of spices because it is one of the oldest spice and alone accounts for about 35% of the world’s total spice trade. The pepper is used in Ayurvedic medicine for the treatment of various ailments particularly neurological, broncho-pulmonary and gastrointestinal disorders. Pepper has also been reported to have various pharmacological actions but recently, it is highlighted as a bioavailability enhancer. This results in higher plasma concentration of drugs, nutrients, ions and other xenobiotics, rendering them more bioavailable for physiological as well as pharmacological actions in the body. Numerous scientific studies reported that piperine; a main bioactive compound of pepper, is responsible for its bioavailability enhancing property. It’s a well known fact that pepper enhances bioavailability by inhibition of microsomal enzyme system but other mechanisms are also responsible to acts as a bioavailability enhancer. The brief overview of the mechanism of action of pepper as well as its applications as bioavailability enhancer is given in the present article. Key words: Piperine; Bioavailability enhancer INTRODUCTION and 3 - 5% (on dry weight basis) in P. nigrum Linn (black pepper) and P. longum Linn (long pepper) Pepper species present as one of the key component respectively. It is isolated from fruits and it is in many preparations and formulations in traditional absent in the leaves and stem of plants. -

Pharmacogenomics: the Promise of Personalized Medicine for CNS Disorders
Neuropsychopharmacology REVIEWS (2009) 34, 159–172 & 2009 Nature Publishing Group All rights reserved 0893-133X/09 $30.00 REVIEW ............................................................................................................................................................... www.neuropsychopharmacology.org 159 Pharmacogenomics: The Promise of Personalized Medicine for CNS Disorders Jose de Leon*,1,2,3,4 1 2 Mental Health Research Center, Eastern State Hospital, University of Kentucky, Lexington, KY, USA; College of Medicine, 3 4 University of Kentucky, Lexington, KY, USA; College of Pharmacy, University of Kentucky, Lexington, KY, USA; Psychiatry and Neurosciences Research Group (CTS-549), Institute of Neurosciences, Medical School, University of Granada, Granada, Spain This review focuses first on the concept of pharmacogenomics and its related concepts (biomarkers and personalized prescription). Next, the first generation of five DNA pharmacogenomic tests used in the clinical practice of psychiatry is briefly reviewed. Then the possible involvement of these pharmacogenomic tests in the exploration of early clinical proof of mechanism is described by using two of the tests and one example from the pharmaceutical industry (iloperidone clinical trials). The initial attempts to use other microarray tests (measuring RNA expression) as peripheral biomarkers for CNS disorders are briefly described. Then the challenge of taking pharmacogenomic tests (compared to drugs) into clinical practice is explained by focusing on regulatory -

Bioavailability of Metals
BIOAVAILABILITY OF METALS by David A. John and Joel S. Leventhal INTRODUCTION The fate of various metals, including chromium, nickel, copper, manganese, mercury, cadmium, and lead, and metalloids, including arsenic, antimony, and selenium, in the natural environment is of great concern (Adriano, 1986; 1992), particularly near former mine sites, dumps, tailing piles, and impoundments, but also in urban areas and industrial centers. Soil, sediment, water, and organic materials in these areas may contain higher than average abundances of these elements, in some cases due to past mining and (or) industrial activity, which may cause the formation of the more bioavailable forms of these elements. In order to put elemental abundances in perspective, data from lands and watersheds adjacent to these sites must be obtained and background values, often controlled by the bedrock geology and (or) water-rock interaction, must be defined. In order to estimate effects and potential risks associated with elevated elemental concentrations that result from natural weathering of mineral deposits or from mining activities, the fraction of total elemental abundances in water, sediment, and soil that are bioavailable must be identified. Bioavailability is the proportion of total metals that are available for incorporation into biota (bioaccumulation). Total metal concentrations do not necessarily correspond with metal bioavailability. For example, sulfide minerals may be encapsulated in quartz or other chemically inert minerals, and despite high total concentrations of metals in sediment and soil containing these minerals, metals are not readily available for incorporation in the biota; associated environmental effects may be low (Davis and others, 1994). Consequently, overall environmental impact caused by mining these rocks may be much less than mining another type of mineral deposit that contains more reactive minerals in lower abundance. -

Pharmacogenomics—Is There a Role in Antibiotic Therapy?
Pharmacogenomics—a role in antibiotic therapy? DB Davison et al 14 sist over long periods of time, and they there are inborn cohesive forces 1 Pinker S. How the Mind Works. WW Nor- cannot grow except by recruitment. which cause the different individ- ton & Company: New York, London, 1997, pp 1–528. In short, populations differ from uals within a population to coop- 2 Wynne Edwards WC. Evolution through each other because many of their erate sufficiently for the popu- group selection. Blackwell: Oxford, 1986. members tend to carry different lation to function as one 3 Wilson DS. Proc Nat Acad Sci USA 1975; 72: mutants; furthermore, it is the non- evolutionary unit. 143–146. 4 Wilson DS. Science 1997; 276: 1816–1817. uniformity of the individual members (2) As a second requirement, there 5 Wilson DS, Sober E. J Theor Biol 1989; 136: of a population which helps a popu- must be effective evolutionary dif- 337–356. lation to function as an effective ferences between individuals 6 Rice SH. J Theor Biol 1995; 177: 237–245. entity, and thereby to allow evolution- which at the same time make 7 Crognier E. Ann Hum Biol 2000; 27: 221– 237. ary competition. The situation is anal- every population different from 8 Michod RE, Roze D. Heredity 2001; 86:1–7. ogous to that of a complex organism other populations. The existence 9 Hamilton WD. J Theor Biol 1964; 7:1–52. which has different cells, but they col- of mutations assures the occur- 10 Maynard Smith J. Evolutionary Genetics (2nd laborate and form a living unit.