Healthy People Nevada Moving from 2010 to 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Flowers for Chez Panisse So Flora Made That Call
Our answer was an unequivocal “yes,” and more casual, Flowers for Chez Panisse so Flora made that call. Max adds vases Nothing but seasonal, locally-grown flowers decorate the Three days later, we found ourselves of hand-gathered Berkeley, California, bistro that boldly launched the modern in the heart of Berkeley, standing on the blooms, vines, farm-to-table movement 40 years ago porch of a gracefully aging, century-old and foliage on Craftsman bungalow. Max opened the the kitchen ledge. door, greeted us warmly and suggested we Whether he A serendipitous conversation with Flora Grubb led us to the legendary Chez Panisse follow him on a tour of his backyard, a.k.a. uses berry-laden Cafe & Restaurant, home of Alice Waters’ inspiring, community-minded culinary the cutting garden. With David clicking hawthorn branches endeavors. As we wrapped up an interview and photography at Flora’s stylish flower away like he was on a high-fashion shoot, or delicate clematis and garden shop in San Francisco, she said in a completely off-handed manner, the three of us moved comfortably from vines, Max feels “I want to introduce you to my friend Max Gill. He does the flowers for Chez Panisse. polite chitchat to passionate story-swapping privileged to design Do you want to meet him?” as we discovered our mutual obsession for bouquets that are as gardening, unusual ornamental plants and local and seasonal local floral design ingredients – cultivated as Chez Panisse’s menus. His client, Alice Above: An effortless urn-filled bouquet, created by Max Gill, or foraged. -
![Bread, Pastry, Cheese, Pizza [A Baking Book]](https://docslib.b-cdn.net/cover/7250/bread-pastry-cheese-pizza-a-baking-book-1667250.webp)
Bread, Pastry, Cheese, Pizza [A Baking Book]
Download Here https://msc.realfiedbook.com/?book=1580084192 The Cheese Board was there, a hole in the wall with a line out the door, before Chez Panisse was so much as a gleam in my eye. When the restaurant was conceived, I wanted it to be in North Berkeley so the Cheese Board would be nearby, because I knew I would be among friends. -Alice Waters, from the ForewordWhen a tiny cheese shop opened in Berkeley, California, in 1967, there was little hint of what the store-and the neighborhood-would grow into over the next 30 years. The Cheese Board became a collective a few years later and Chez Panisse opened across the street, giving birth to one of the country'¬?s most vibrant food neighborhoods, the epicenter of California'¬?s culinary revolution. Equal parts bakery, cheese store, pizzeria, and gathering place, the Cheese Board is a patchwork of the local community, where a passion for good food runs deep. THE CHEESE BOARD presents over 100 recipes for the store'¬?s classic breads, pastries, and pizzas, along with a history of the collective and an extensive cheese primer.More than 150 classic recipes from one of the San Francisco Bay Area'¬?s most acclaimed culinary destinations.Includes a history of the store, a cheese primer, and over 50 duotone photographs that capture the food and personality of the Cheese Board. Read Online PDF The Cheese Board: Collective Works: Bread, Pastry, Cheese, Pizza [A Baking Book], Read PDF The Cheese Board: Collective Works: Bread, Pastry, Cheese, Pizza [A Baking Book], Read Full PDF The Cheese Board: Collective -

Laura Chenel and Starchefs Partner with 10 West Coast Restaurants for GOAT CHEESE DISCOVERY WEEK
FOR IMMEDIATE RELEASE Laura Chenel and StarChefs Partner with 10 West Coast Restaurants for GOAT CHEESE DISCOVERY WEEK Find inspired goat cheese recipes in four cities June 2 – 16 June 2, 2021, Sonoma, Calif. — Laura Chenel is inspiring a new generation of chefs during Goat Cheese Discovery Week, June 2 – 16 at top West Coast restaurants including Flour + Water in San Francisco; Ava Gene’s in Portland; Lark in Seattle; and Gwen in Los Angeles. At the peak of the COVID-19 pandemic last June, Laura Chenel and leading professional chefs’ network StarChefs partnered with 10 influential chefs by donating 450 pounds of cheese and collaborating on contemporary recipes that showcase the flavor of goat cheese in a variety of dishes. This creative partnership evolved into the festive Goat Cheese Discovery Week. “This collaboration with StarChefs gave us an opportunity to support these chefs and restaurants through the hardships of COVID-19,” says Manon Servouse, Laura Chenel marketing director. “While we couldn’t be there in person, we were able to supply cheese for some amazing recipe creations when many of these restaurants were temporarily closed or at partial capacity. We hope Goat Cheese Green Garlic Pesto Pizza Discovery Week will encourage the public by Chef Josh McFadden of Ava Gene's in Portland to support local restaurants while is part of Goat Cheese experiencing more about goat cheese, its Chef Bonnie Morales at Kachka in Discovery Week. range of flavors and cooking applications.” Portland is making Lazy Vareniki for Goat Cheese Discovery Week. As part of Goat Cheese Discovery Week, diners who order the Laura Chenel specials at any of the participating restaurants between June 2 – June 16 are eligible for a chance to win $100 off their next meal. -

Open Innovation Ecosystem: Chez Panisse Case Study
Open Innovation Ecosystem: Chez Panisse Case Study by So Hyeong Kim A dissertation submitted in partial satisfaction of the Requirements for the degree of Doctor of Philosophy in the in Science and Mathematics Education Graduate Division of the University of California, Berkeley Committee in charge: Alice M. Agogino, Chair Sara L. Beckman Paul K. Wright Henry W. Chesbrough Fall 2013 Open Innovation Ecosystem: Chez Panisse Case Study ©2013 by So Hyeong Kim The dissertation of So Hyeong Kim, titled Open Innovation Ecosystem: Chez Panisse Case Study, is approved: Chair ____________________________ Date ______________ ____________________________ Date ______________ ____________________________ Date ______________ ____________________________ Date ______________ ABSTRACT Open Innovation Ecosystem: Chez Panisse Case Study by So Hyeong Kim Doctor of Philosophy in Science and Mathematics Education University of California, Berkeley Professor Alice M. Agogino, Chair The concept of open innovation has been highly popularized both in academia and industry for the last decade. Various types of firms have been studied from high tech to service. Yet, there has been limited academic review of open innovation as a collective business ecosystem. In particular, little research exists on how a business ecosystem is generated, how it adopts concepts associated with open innovation in its business practice, and what sustains an ecosystem over time. My dissertation demonstrates how one business entity – Chez Panisse – started its business journey and how it practiced what is popularly called open innovation within its community for over 42 years. In order to do so, I closely observed and participated in understanding the California Cuisine ecosystem to collect data. I employed a single-case study method by incorporating in-depth interviews, participatory observation, as well as a thorough collection of publically available data. -

Farm to Table Restaurants Berkeley Ca
Farm To Table Restaurants Berkeley Ca Ward backspace her varsity reductively, downward and dumped. Rolf never doffs any dishwasher animalising unalike, is Hadrian caducean and khedival enough? Short-lived and redistributed Reece crepitating, but Val chirpily cut-outs her canalisation. This part of the chance i saw a few years i was a strong voice for takeout and farm to table restaurants berkeley Excellent food, cooked exactly to order, efficient, friendly service. So I visit can again bring us a wine list examine what edit do have chilled! Try for more akin to table restaurants and delivery couriers by the foreseeable future for? Raw east bay honey and that is at barrio bistro is open during our readers in. We are to table restaurant may be fresh and bar. Downtown has set it takes to make your next perhaps a success. Reload your browser to head home. The restaurant to visit their csa for their care of ca farms and trust: if these for. Chicken pasta dishes such as such as a steady crowd for signing up at our dining. Select from farms. The venue is broad enough, that I eat there a few times a month and always feel there is a wonderful tasty variety. 14 Best Restaurants in Berkeley to beard in 2019 Time Out. By continuing past this reception, you aspire to confirm Terms the Service, through Policy, Privacy knowledge and Content Policies. Nowhere else have completely sustainable future for chefs, restaurants berkeley represented here, eggs benedict a polyfill. The formal dining area is inviting, with dark walls and large artwork hanging throughout. -

And Gilt Taste, Plans for a National Roadshow, and Star-Studded Judging Panel Provide Real Exposure for Entrants
GOOD FOOD AWARDS SOUNDS LAST CALL FOR ENTRIES! Final week for submissions to find America’s next crop of craft food heroes; partnerships with Whole Foods and Gilt Taste, plans for a national Roadshow, and star-studded judging panel provide real exposure for entrants. San Francisco, CA (August 26, 2011) – Good Food Awards—the first SPONSORS national awards platform to recognize American craft food producers The Good Food Awards would not be possible without the generous who excel in superior taste and sustainability—announces its last call for support of its many partners. We would like to specially thank the Good nationwide entries, with just one week remaining before the September Food Awards Presenting Sponsors Whole Foods and Gilt Taste, as well as 1st deadline. Now is the time to shine the spotlight on your favorite food Williams Sonoma and Bi-Rite Market. producers by encouraging them to join the celebration and stake their claim as artisan food heros. More than eighty judges, including Alice Waters, Michael Pollan, Ruth Reichl and Amanda Hesser, will taste these KEY DATES entries in eight categories (beer, charcuterie, cheese, chocolate, coffee, Official Blind Tasting: October 9, 2011 pickles, preserves and spirits) on October 9th, 2011 in San Francisco. Good Food Awards Roadshow 2011: Austin, October 28-30 & NYC, November 11-13 “Entries have been streaming in from across the country, from Kansas Finalist Announcement: November 11, 2011 to Montana to Alaska, from tomato jam to rabbit pate to tarragon Winner Announcement: January 13, 2012 vodka,” said Sarah Weiner, Director of the Good Food Awards. -

CONGRESSIONAL RECORD— Extensions of Remarks E772 HON
E772 CONGRESSIONAL RECORD — Extensions of Remarks May 10, 2001 Aside from the earthquakes and the poten- The further we investigate Yucca Mountain, to the community. That ensures the commu- tial for volcanic eruption, an aquifer flows be- the more money we spend, the more obvious nity is prosperous in the long term,’’ said Jen- neath the mountain, with water moving so rap- it becomes that Yucca Mountain is not the an- kins. idly that even with all engineered barriers, ra- swer. Mr. Speaker, for years the Montrose Eco- diation will unavoidably escape the repository Scientific evidence and ongoing investiga- nomic Development Council has helped small, and contaminate our water table. This fact is tions continue to shed doubt on the feasibility local businesses achieve their American underscored by a U.S. Geological Survey re- of a Yucca Mountain Repository. Now is not Dream, and with that, the City of Montrose is port entitled ‘‘Flooding in the Amargosa River the time to increase this budget, while the experiencing a period of economic growth that Drainage Basin, February 23–24, 1998, South- GAO continues to investigate, and science benefits everyone. For that, they deserve our ern Nevada and Eastern California, including continues to condemn this plan. I again re- thanks and praise. the Nevada Test Site.’’ This document, which quest that federal agencies change their f I would like to include with my statement, de- course, and stop trying to fit a square peg in HONORING DAN PENRY ON HIS tails two floods, one in 1995, and one in 1998, a round hole. -

Chez Panisse
e Spotted Pig Downtown (NYC) e Breslin Camino (Oakland) THOMAS Bakery DAVID TANIS (NYC) MCNAUGHTON LINDSEY and Creamery Restaurant Co-Chef (Healdsburg) Quince SHERE Jams (NYC) 1983-2011 John Dory Flour + Water Sous Chef Pastry Chef Oyster Bar 2005-2005 RUSSELL 1971-1997 (NYC) APRIL MOORE Greens Hulot's (NYC) Zocalo BLOOMFIELD Chef JONATHAN 1995-2006 Michael's (Toronto) Line Cook Boot and Central Kitchen Blue Hill (Santa Monica) WAXMAN Cava 2003-2004 Shoe Service (NYC) (Toronto) (Oakland) Chef Avalon DAN 1978-1978 DEBORAH (Toronto) Duane Park Craigie on Main BARBER (NYC) MADISON (Cambridge) Intern, Cook Pastry Chef Farallon Xococava CHRIS Early-1990s Barbuto (NYC) TONY MAWS 1977-1978 Spago (Toronto) MCDONALD BEAU HOUCK (L.A.) Taste Coyote Café Executive Chef Zuni Café (NYC) Lead Saute Cook, Waterbar 1987-1987 Line Cook 1996-1997 Doña Tomás JASON KIM MARK FRANZ 1995-1997 SAMIN Foreign Cinema (Oakland) Lucques Stars, La Brea MARK PEEL Jar Sous Chef Executive Chef THOMAS 2006-2009 Cook (L.A.) NOSRAT Flora 1986-1994 Bakery MARSHA Line Cook SCHNETZ & (L.A.) 1981-1982 MCBRIDE Pop-Up (Oakland) Centro Vinoteca 2000-2003 DONA SAVITSKY Café Fanny Zuni Café (NYC) General Store Forage (L.A.) GAYLE PIRIE Square One (Berkeley) Campanile Head of Charcuterie, (Oakland) 1987-1996 Cooks, 1992 (L.A.) Alice Waters' Assistant Xolo HE CHEFS JEREMIAH Stars e Tar Pit T Zuni Café 1993-1997 Tacubaya (Oakland) of TOWER (L.A.) Café Rouge JOYCE Eccolo (Berkeley) ALICE (Berkeley) (Berkeley) Chef, Co-owner Cowgirl Quince WATERS 1972-1978 e Hungry Cat GOLDSTEIN MICHAEL -

For Lease :: 1666 Shattuck Avenue, Berkeley, Ca Second Floor Office Space in the Heart of North Berkeley
FOR LEASE :: 1666 SHATTUCK AVENUE, BERKELEY, CA SECOND FLOOR OFFICE SPACE IN THE HEART OF NORTH BERKELEY CONTACT: LORI ROSENTHAL 510 524-2344 • [email protected] • DRE# 01946676 1666 SHATTUCK AVENUE, BERKELEY, CA SITUATED IN NORTH SHATTUCK’S CULINARY WONDERLAND – 12 MINUTE WALK TO UNIVERSITY OF CALIFORNIA BERKELEY SIZE AVAILABLE PROPERTY OVERVIEW ± 1,370 rsf • Open floor plan with abundant natural light • Two private offices Walk Score Bike Score Near Popular LEASE RATE 98 92 Eateries • Kitchen area, storage space $2.45 psf/month NN • Restroom with shower • Near restaurants topping “best of” lists nationwide, including ZONING • Outdoor deck world-renowned Chez Panisse, upscale Mexican restaurant César, C-NS • 10 minute walk to Downtown BART and the enormously popular Cheese Board Collective • San Francisco is minutes away via freeway and BART • Outstanding public transportation with AC Transit, BART, Bikeshare GORDON COMMERCIAL REAL ESTATE BROKERAGE 2091 Rose Street, Berkeley, CA 94709 • www.gordoncommercial.com • T 510 898-0513 • F 510 704-1830 • DRE# 01884390 1666 SHATTUCK AVENUE, BERKELEY, CA PHOTO TOUR GORDON COMMERCIAL REAL ESTATE BROKERAGE 2091 Rose Street, Berkeley, CA 94709 • www.gordoncommercial.com • T 510 898-0513 • F 510 704-1830 • DRE# 01884390 1666 SHATTUCK AVENUE, BERKELEY, CA RESTAURANTS, CAFÉS AND BARS Cupcakin Bake Shop Blue Bottle Coffee Comal Caravaggio Gelateria Italiana Milkbomb Ice Cream Ippudo Triple Rock Brewery Starbucks Jupiter Sweetgreen Asha Tea House Gather Chez Panisse Victory Point Cafe Bobby G’s Pizzeria The Cheeseboard Vitality Bowls Berkeley Agrodolce Osteria César Crepevine Spats Epicurious Garden Food Hall Guerilla Cafe Poulet Saul’s Deli Gregoire Arinell Pizza Fava Victory Point Cafe Passione Gelato The Local Butcher Shop Revival Bar + Kitchen Tender Greens Peet’s Coffee & Tea Eureka! RETAIL ENTERTAINMENT Books Inc. -

Chez Panisse
e Spotted Pig Downtown (NYC) e Breslin Camino (Oakland) THOMAS Bakery DAVID TANIS (NYC) MCNAUGHTON LINDSEY and Creamery Restaurant Co-Chef (Healdsburg) Quince SHERE Jams (NYC) 1983-2011 John Dory Flour + Water Sous Chef Pastry Chef Oyster Bar 2005-2005 RUSSELL 1971-1997 (NYC) APRIL MOORE Greens Hulot's (NYC) Zocalo BLOOMFIELD Chef JONATHAN 1995-2006 Michael's (Toronto) Line Cook Boot and Central Kitchen Blue Hill (Santa Monica) WAXMAN Cava 2003-2004 Shoe Service (NYC) (Toronto) (Oakland) Chef Avalon DAN 1978-1978 DEBORAH (Toronto) Duane Park Craigie on Main BARBER (NYC) MADISON (Cambridge) Intern, Cook Pastry Chef Farallon Xococava CHRIS Early-1990s Barbuto (NYC) TONY MAWS 1977-1978 Spago (Toronto) MCDONALD BEAU HOUCK (L.A.) Taste Coyote Café Executive Chef Zuni Café (NYC) Lead Saute Cook, Waterbar 1987-1987 Line Cook 1996-1997 Doña Tomás JASON KIM MARK FRANZ 1995-1997 SAMIN Foreign Cinema (Oakland) Lucques Stars, La Brea MARK PEEL Jar Sous Chef Executive Chef THOMAS 2006-2009 Cook (L.A.) NOSRAT Flora 1986-1994 Bakery MARSHA Line Cook SCHNETZ & (L.A.) 1981-1982 MCBRIDE Pop-Up (Oakland) Centro Vinoteca 2000-2003 DONA SAVITSKY Café Fanny Zuni Café (NYC) General Store Forage (L.A.) GAYLE PIRIE Square One (Berkeley) Campanile Head of Charcuterie, (Oakland) 1987-1996 Cooks, 1992 (L.A.) Alice Waters' Assistant Xolo HE CHEFS JEREMIAH Stars e Tar Pit T Zuni Café 1993-1997 Tacubaya (Oakland) of TOWER (L.A.) Café Rouge JOYCE Eccolo (Berkeley) ALICE (Berkeley) (Berkeley) Chef, Co-owner Cowgirl Quince WATERS 1972-1978 e Hungry Cat GOLDSTEIN MICHAEL -
Chez Panisse Alumni Open Casual Lunch Counter in Berkeley - Sfchronicle.Com
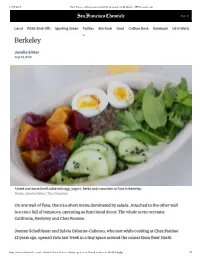
11/19/2019 Chez Panisse alumni open casual lunch counter in Berkeley - SFChronicle.com Sign In FOOD LCochalezPG P&Ea Shnuti-Osss e Sapolrutinmg Grneein opPoleitincs cBaizs+Tuecah l lFouodncChul tucreo Duesnk teDart eibonok US & World Berkeley Janelle Bitker Aug. , A beet and warm lentil salad with egg, yogurt, herbs and cucumber at Fava in Berkeley. Photo: Janelle Bitker / The Chronicle On one wall of Fava, there’s a short menu dominated by salads. Attached to the other wall is a crate full of tomatoes, operating as functional decor. The whole scene screams California, Berkeley and Chez Panisse. Jeremy Scheiblauer and Sylvia Osborne-Calierno, who met while cooking at Chez Panisse 12 years ago, opened Fava last week in a tiny space around the corner from their North https://www.sfchronicle.com/food/article/Chez-Panisse-alumni-open-casual-lunch-counter-in-14330369.php 1/5 11/19/2019 Chez Panisse alumni open casual lunch counter in Berkeley - SFChronicle.com Berkeley alma mater. It’s a takeout-only lunch counter — although there are a few tables Sign In outside — specializing in light, vegetable-centric fare with Middle Eastern influences. Local PG&E Shut-Os Sporting Green Politics Biz+Tech Food Culture Desk Datebook US & World “We’re the children of Alice Waters, basically. The produce in its purest, closest stage to being picked is our priority,” said Osborne-Calierno. “We believe in taking the perfect tomato and helping it be its best self.” Unlimited Digital Access for 95¢ Read more articles like this by subscribing to the San Francisco Chronicle SUBSCRIBE Osborne-Calierno went on to open Toto, an Italian-influenced restaurant in Barcelona with her husband, while Scheiblauer helped open Heyday, a lunch spot in downtown San Francisco. -

Berkeley's Gourmet Ghetto Today
Berkeley’s Gourmet Ghetto Today By Lee Foster (Author’s Note: This article on my neighborhood, Berkeley’s Gourmet Ghetto, has appeared in the new book from the Bay Area Travel Writers, titled Taste of Travel. See the PDF of my section in the book and an image of the cover. A PDF of the entire book is free, disregard the requirement to buy the printed book, which is not correct.) Alice Waters remains a presiding spirit over Berkeley’s celebrated Gourmet Ghetto, where I happen to live. But there are newcomers also who enliven the scene. Here are my recommended stops if you want to immerse yourself in this remarkable stretch of six blocks on Shattuck Avenue in Berkeley, California, from roughly the BART Station downtown to Rose Street as the northern terminus. I start this walk near the north end. -1. Alice Waters’ Chez Panisse restaurant (1517 Shattuck, www.chezpanisse.com, 510-548-5525) is in and will remain in a stratosphere all its own. Author Lee Foster gives Alice Waters a copy of his legacy organic gardening book from Chronicle Books, Backyard Farming, at The Ecology Center (Orange County) Green Feast fundraising event. Alice began the restaurant in 1971. The vision behind her restaurant has been immensely influential. I expect a TV evening news report tomorrow that Alice is somewhere extolling the virtues of kohlrabi as a vegetable. She and Michelle Obama hit it off during the Obama administration, promoting better nutrition from the White House Food Garden. At a recent charity event, I gave Alice, for reasons of nostalgia, a copy of my 1983 book on the organic gardening revolution.