Women's Prior Knowledge of the Abortion Law and Decision-Making
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Globalisation and Transitions in Abortion Care in Ghana Patience Aniteye1 and Susannah H
Aniteye and Mayhew BMC Health Services Research (2019) 19:185 https://doi.org/10.1186/s12913-019-4010-8 RESEARCHARTICLE Open Access Globalisation and transitions in abortion care in Ghana Patience Aniteye1 and Susannah H. Mayhew2* Abstract Background: Access to safe abortion is a globally contested policy and social justice issue – contested because of its religious and moral dimensions regarding the right to life and personhood of a foetus vs. the rights of women to make decisions about their own bodies. Many nations have agreed to address the health consequences of unsafe abortion, though stopped short of committing to providing comprehensive services. Ghana has a relatively liberal abortion law dating from 1985 and has ratified most international agreements on provision of care. Policy implementation has been very slow, but modest effortsarenowbeingmadetoreducematernalmortality caused by unsafe abortions. Understanding whether globalisation has played a role in this transition to practice is important to institutionalise the transition in Ghana and to learn lessons for other countries seeking to implement policies, but analysis is lacking. Methods: Drawing on 58 in-depth key informant interviews and policy document analysis we describe the development of de jure law and policies on comprehensive abortion care in Ghana, de facto interpretation and implementation of those policies, and assess what role globalization played in the transition in abortion care in Ghana. Results: We found that an accumulation of global influences has converged to start a transition in the culture of abortion care and service provision in Ghana, from a restrictive interpretation of the law to facilitating more widespread access to legal, safe abortion services through development of policies and guidelines and a slow change in attitudes and practices of health providers. -

Availability, Accessibility and Utilization of Post-Abortion Care in Sub-Saharan Africa: a Systematic Review
HEALTH CARE FOR WOMEN INTERNATIONAL https://doi.org/10.1080/07399332.2019.1703991 REVIEW ARTICLE Availability, accessibility and utilization of post-abortion care in Sub-Saharan Africa: A systematic review Chimaraoke Izugbaraa, Frederick Murunga Wekesahb , Meroji Sebanya, Elizabeth Echokac, Joshua Amo-Adjeid, and Winstoun Mugab aInternational Center for Research on Women, Washington, D.C, USA; bAfrican Population & Health Research Center, Nairobi, Kenya; cCentre for Public Health Research, Kenya Medical Research Institute - KEMRI, Nairobi, Kenya; dDepartment of Population and Health, University of Cape Coast, Cape Coast, Ghana ABSTRACT ARTICLE HISTORY At the 1994 ICPD, sub-Saharan African (SSA) states pledged, Received 28 June 2019 inter alia, to guarantee quality post-abortion care (PAC) serv- Accepted 9 December 2019 ices. We synthesized existing research on PAC services provi- sion, utilization and access in SSA since the 1994 ICPD. Generally, evidence on PAC is only available in a few countries in the sub-region. The available evidence however suggests that PAC constitutes a significant financial burden on public health systems in SSA; that accessibility, utilization and avail- ability of PAC services have expanded during the period; and that worrying inequities characterize PAC services. Manual and electrical vacuum aspiration and medication abortion drugs are increasingly common PAC methods in SSA, but poor-qual- ity treatment methods persist in many contexts. Complex socio-economic, infrastructural, cultural and political factors mediate the availability, accessibility and utilization of PAC services in SSA. Interventions that have been implemented to improve different aspects of PAC in the sub-region have had variable levels of success. Underexplored themes in the exist- ing literature include the individual and household level costs of PAC; the quality of PAC services; the provision of non-abor- tion reproductive health services in the context of PAC; and health care provider-community partnerships. -

Introduction of Medical Abortion in Ghana
Population Council Knowledge Commons Reproductive Health Social and Behavioral Science Research (SBSR) 2011 Introduction of medical abortion in Ghana Emmanuel Kuffour Population Council Selina F. Esantsi Population Council Placide Tapsoba Population Council Gloria Quansah Asare Ian Askew Population Council Follow this and additional works at: https://knowledgecommons.popcouncil.org/departments_sbsr-rh Part of the Demography, Population, and Ecology Commons, Family, Life Course, and Society Commons, Health Policy Commons, International Public Health Commons, Obstetrics and Gynecology Commons, Public Health Education and Promotion Commons, and the Women's Health Commons How does access to this work benefit ou?y Let us know! Recommended Citation Kuffour, Emmanuel, Selina F. Esantsi, Placide Tapsoba, Gloria Quansah Asare, and Ian Askew. 2011. "Introduction of medical abortion in Ghana." Accra: Population Council. This Report is brought to you for free and open access by the Population Council. INTRODUCTION OF MEDICAL ABORTION IN GHANA Emmanuel Osei Kuffour1 , Selina F. Esantsi1, Placide Tapsoba1, Gloria Quansah- Asare2, Ian Askew3 Emmanuel Osei Kuffour PhD (abd); M&E Advisor, Population Council, Ghana, Selina F. Esantsi, MA; Program Officer, Population Council, Ghana Placide Tapsoba, MD, MPH; Director, Population Council, Ghana Gloria Quansah-Asare, MD, PhD; Director of Family Health Division, Ghana Health Service Ian Askew Ph.D; Director, Reproductive Health Services and Research, Population Council i INTRODUCTION OF MEDICAL ABORTION IN GHANA Emmanuel Osei Kuffour1, Selina F. Esantsi1, Placide Tapsoba1, Gloria Quansah-Asare2, Saumya RamaRao3 The Population Council is an international, nonprofit, nongovernmental organization that seeks to improve the well-being and reproductive health of current and future generations around the world and to help achieve a humane, equitable, and sustainable balance between people and resources. -

Unusual Presentation of Phaechromocytoma in a Child- A
September 2006 Volume 40, Number 3 GHANA MEDICAL JOURNAL OVERVIEW OF THE LAW AND AVAILABILITY OF ABORTION SERVICES IN GHANA R.A.S MORHEE AND *E.S.K. MORHEE1 Faculty of Law, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana and 1De- partment of Obstetrics and Gynaecology, Komfo Anokye Teaching Hospital, Kumasi, Ghana. SUMMARY this form of behaviour with the aim of preventing Introduction: In Ghana unsafe abortion remains a its occurrence and to deter people with like minds major public health problem despite apparent lib- from indulging in such a practice. History how- eralization of the law on abortion over two dec- ever, shows that abortion is a fundamental human ades. The contention is that the current law on behaviour that has been practiced in all cultural abortion makes enforceability difficult and leaves settings and that no level of restrictive laws has 1,2 room for untrained personnel to engage in danger- succeeded in controlling it. Thus when a woman ous abortion procedures and that there is need for decides to end an unwanted pregnancy she will law reform. often go to extreme length to do so, regardless of Objectives: To bring into focus how the current whether the procedure is safe or legal and as long law affects the availability of safe abortion service as there is unwanted pregnancy abortion will be a in Ghana and to bring out suggestions that may be fact of life. Unsafe abortion accounts for at least useful in future amendment of the law. 13% of global maternal mortality that is dispropor- 3,4 Methods: Using the information gathered from tionately high in Africa Most of these deaths as literature review the current law on abortion in well as the long-term complications of unsafe Ghana and relevant sections of the criminal code abortion are preventable through improved access were critically analyzed from medico-legal per- to effective family planning methods and contra- spective. -

Abortion Care in Ghana: a Critical Review of the Literature
Rominski & Lori Abortion care in Ghana Abortion care in Ghana REVIEW ARTICLE Abortion Care in Ghana: A Critical Review of the Literature Sarah D Rominski1* and Jody R Lori2 1Global REACH, University of Michigan Medical School; 2School of Nursing, University of Michigan. * For Correspondence: E-mail: [email protected], Phone: 001-734-717-5930. Abstract The Government of Ghana has taken important steps to mitigate the impact of unsafe abortion. However, the expected decline in maternal deaths is yet to be realized. This literature review aims to present findings from empirical research directly related to abortion provision in Ghana and identify gaps for future research. A total of four (4) databases were searched with the keywords “Ghana and abortion” and hand review of reference lists was conducted. All abstracts were reviewed. The final include sample was 39 articles. Abortion-related complications represent a large component of admissions to gynecological wards in hospitals in Ghana as well as a large contributor to maternal mortality. Almost half of the included studies were hospital-based, mainly chart reviews. This review has identified gaps in the literature including: interviewing women who have sought unsafe abortions and with healthcare providers who may act as gatekeepers to women wishing to access safe abortion services. (Afr J Reprod Health 2014; 18[3]: 17-35) Keywords: Abortion, Ghana, Review Résumé Le gouvernement du Ghana a pris des mesures importantes pour atténuer l'impact de l'avortement à risque. Cependant, la baisse attendue de la mortalité maternelle est encore à réaliser. Cette revue de la documentation a pour but de présenter les résultats de recherches empiriques directement liés à la prestation de l'avortement au Ghana et d'identifier les lacunes de la recherche future. -
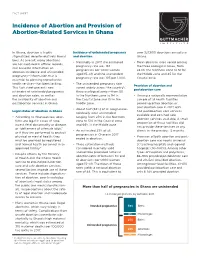
Incidence of Abortion and Provision of Abortion-Related Services in Ghana
FACT SHEET Incidence of Abortion and Provision of Abortion-Related Services in Ghana In Ghana, abortion is highly Incidence of unintended pregnancy over 327,600 abortions annually in stigmatized, despite relatively liberal and abortion Ghana. laws. As a result, many abortions • Nationally in 2017, the estimated • Mean abortion rates varied among are not captured in official records, pregnancy rate was 194 the three ecological zones, from and accurate information on pregnancies per 1,000 women 24 for the Northern zone to 51 for abortion incidence and unintended aged 15–49, and the unintended the Middle zone and 45 for the pregnancy—information that is pregnancy rate was 103 per 1,000. Coastal zone. essential to planning reproductive health services—has been lacking. • The unintended pregnancy rate Provision of abortion and This fact sheet presents new varied widely across the country’s postabortion care estimates of unintended pregnancy three ecological zones—from 50 and abortion rates, as well as in the Northern zone to 94 in • Among a nationally representative the availability of abortion and the Coastal zone and 131 in the sample of all health facilities postabortion services in Ghana. Middle zone. providing either abortion or postabortion care in 2017, 63% • About half (53%) of all pregnancies Legal status of abortion in Ghana had postabortion care services nationally were unintended, available and 22% had safe • According to Ghanaian law, abor- ranging from 23% in the Northern abortion services available. A small tions are legal in cases of rape, zone to 51% in the Coastal zone proportion of these facilities did incest, fetal abnormality or disease, and 66% in the Middle zone. -

Abortions in Ghana: Experiences of University Students
VOLUME 8 (2014),ISSUE 4 HEALTH SCIENCE JOURNAL RESEARCH ARTICLE (26.1%) of students. Conclusions: Abortions, mostly unsafe, are Abortions in Ghana: common experiences among students. Immediate sensitization and education on the experiences of university alternatives to abortions; unsafe abortions; students contraception; and counselling and family planning services is necessary among students. Nana Nimo Appiah-Agyekum Male partners play a significant role in the decision to abort, choice of method and also Department of Public Administration and provide support during the abortion procedures; Health Services Management, University of and must be actively involved in all abortion Ghana Business School, Accra-Ghana interventions among students. Particular attention and the necessary research by both Abstract state and non-state stakeholders on abortion Background: Students in Ghana and other must focus on the activities of quack abortion developing countries remain the major providers, self-induced abortions among vulnerable group most likely to have abortions students as well as reasons for the low utilization and suffer abortion stigma. However there is a of safe abortion services among students in spite dearth of empirical information on the of their knowledge of and access to these experiences of Higher Education students on services . abortion needed for evidence based policies and interventions. Keywords: Abortion, unsafe, experiences, self- Aim: The aim of the present study was to explore induced, students, Ghana some of the key experiences of University students on abortion in Ghana so as to provide Corresponding author: Nana Nimo Appiah-Agyekum, Department of Public Administration and Health Services information for evidence based interventions. Management, University of Ghana Business School, P O Box Methods: Data was collected from 142 students LG 78, Legon, Accra, Ghana, Email: nappiah- of the University of Ghana through 18 focus [email protected] group discussions [FGDs]. -
Interpreting and Implementing Existing Abortion Laws in Africa 2013
Interpreting and Implementing Existing Abortion Laws in Africa 2013 Content INTRODUCTION 8 SUMMARY OF LAWS REGULATING ABORTION IN AFRICA 11 WORLD HEALTH ORGANIZATION GUIDANCE ON SAFE ABORTION 13 CARE . TRANSLATING HEALTH AND HUMAN RIGHTS STANDARDS INTO ACTION: BRIEF CASE STUDIES FROM THREE COUNTRIES (GHANA, ETHIOPIA, 17 Zambia) CONCLUSION 21 ANNEX I: SOURCES TO CONSIDER WHEN INTERPRETING AND IMPLEMENTING 23 ABORTION LAWS ANNEX II: FURTHER INFORMATION ON HUMAN RIGHTS STANDARDS 33 3 Foreword The promotion of maternal, newborn and child health (MNCH) across the African continent is a priority of the African Union Commission. The continent has, no doubt, recorded significant improvement with regard to MNCH status. The economic growth being experienced across the continent provides a further window of opportunity to consolidate on those gains and cover more ground. Maternal, Newborn and Child Health status is a very critical indicator that provides an insight into the quality of life of any nation’s citizens. Women account for about fifty percent of the continent’s population. Therefore sustainable economic growth cannot be engendered unless they are empowered and their overall quality of life is improved. Unsafe abortion unfortunately continues to contribute to morbidity and mortality in Africa. Each AU member state has laws in place to regulate the practice within its sovereign responsibility to promote community wellbeing. Evidence has shown that if these laws, irrespective of their apparently liberal or restrictive nature, are implemented with a view to saving women’s lives and improving their health, the contribution of unsafe abortion to maternal mortality will be significantly contained. Evidence further shows that restrictive laws result in higher levels of unsafe abortion. -

Post-Abortion Contraception in Ghana Background
Post-Abortion Contraception in Ghana Background: In developing countries, including Ghana, approximately 26% of maternal deaths occur among young women aged 15-19 (Patton et al 2013). Many pregnancies in this age group are unplanned and unwanted; resulting in high rates of induced abortion, many of which are unsafe (Evens et al 2014). There are an estimated 5.5 million unsafe abortions in sub-Saharan Africa every year (WHO 2011) and although the overall number of abortions is declining, the proportion of all abortions that are unsafe is rising (Haddad & Nour 2009). The abortion law in Ghana is one of the most liberal on the continent allowing for abortion by a qualified health worker in a registered facility if the pregnancy is the result of rape or incest, if there is fetal malformation or if the continuation of the pregnancy will risk the mental or physical health of the mother (Morhe & Morhe 2006). The total fertility rate in Ghana has fallen from between 4.5 and 5 births per woman in 1985 to around 3 per woman in 2006 (Finlay & Fox 2013), a higher decline than can be explained by the contraception prevalence rate in the country (Blanc 2002). However, it is less clear what impact the liberalization of the law has had on Ghanaian women’s ability and willingness to access a safe abortion (Finlay & Fox 2013). Further, regardless of the law governing abortion, it remains a highly stigmatized procedure and relaxing a law may not, without additional steps, reduce this stigmatization (Shellenberg et al, 2011). Not all unsafe abortions result in death. -

Predictors of Pregnancy Termination Among Young Women in Ghana: Empirical Evidence from the 2014 Demographic and Health Survey Data
healthcare Article Predictors of Pregnancy Termination among Young Women in Ghana: Empirical Evidence from the 2014 Demographic and Health Survey Data Bright Opoku Ahinkorah 1 , Abdul-Aziz Seidu 2,3 , John Elvis Hagan Jr. 4,5,* , Anita Gracious Archer 6, Eugene Budu 2, Faustina Adoboi 7 and Thomas Schack 5 1 School of Public Health, Faculty of Health, University of Technology Sydney, Sydney 2007, Australia; [email protected] 2 Department of Population and Health, University of Cape Coast, Cape Coast 0494, Ghana; [email protected] (A.-A.S.); [email protected] (E.B.) 3 College of Public Health, Medical and Veterinary Sciences, James Cook University, Townsville 4811, Australia 4 Department of Health, Physical Education, and Recreation, University of Cape Coast, Cape Coast 0494, Ghana 5 Neurocognition and Action-Biomechanics-Research Group, Faculty of Psychology and Sports Science, Bielefeld University, Postfach 1001 31, 33501 Bielefeld, Germany; [email protected] 6 School of Nursing and Midwifery, University of Health and Allied Sciences, Sokode-Lokoe PMB 31, Ho 342-0041, Ghana; [email protected] 7 Cape Coast Nursing and Midwifery Training College, Cape Coast 729, Ghana; [email protected] * Correspondence: [email protected] Citation: Ahinkorah, B.O.; Seidu, Abstract: Pregnancy termination remains a delicate and contentious reproductive health issue A.-A.; Hagan, J.E., Jr.; Archer, A.G.; because of a variety of political, economic, religious, and social reasons. The present study examined Budu, E.; Adoboi, F.; Schack, T. the associations between demographic and socio-economic factors and pregnancy termination among Predictors of Pregnancy Termination young Ghanaian women. -

Abortion in Ghana
In Brief 2010 Series, No.2 Abortion in Ghana Maternal mortality is the second most common cause of incidence. Nevertheless, we must rely on such surveys where other sources of death among women in Ghana, and more than one in 10 information on abortion are sparse. maternal deaths (11%) are the result of unsafe induced According to the GMHS, 7% of all 1 abortions. In addition, a substantial proportion of women pregnancies end in abortion (Figure 1, who survive an unsafe abortion experience complications page 2), and 15% of women aged 15 –49 have ever had an abortion.1 About 15 from the procedure. This suffering is all the more tragic abortions are performed for every 1,000 women of reproductive age (15–44) each because it is unnecessary: Many women likely turn to un- year. According to a study conducted in safe providers or do not obtain adequate postabortion care the late 1990s in southern Ghana, 17 abortions were observed for every 1,000 when it is needed because they are unaware that abortion women of reproductive age.5 The level of is legal on fairly broad grounds in Ghana. abortion in Ghana appears to be lower than in Western Africa as a whole, where the rate stands at 28 procedures per The abortion law in Ghana, enacted in a program to reduce maternal morbid- 1,000 women.6 1985, states that an abortion performed ity and mortality—particularly that due by a qualified medical practitioner is le- to unsafe abortion—in Ghana.4 The While underreporting might compro- gal if the pregnancy is the result of rape, program’s goals include ensuring that mise the accuracy of induced abortion incest or “defilement of a female idiot;” contraceptives and comprehensive abor- estimates, there is fairly clear evidence if continuation of the pregnancy would tion care are routinely available at all that 37% of births in the country are un- risk the life of the woman or threaten levels of the public and private health planned—23% are mistimed and 14% are her physical or mental health; or if there service delivery system. -

Seeking in Ghana, West Africa
International Journal of Gynecology and Obstetrics 126 (2014) 217–222 Contents lists available at ScienceDirect International Journal of Gynecology and Obstetrics journal homepage: www.elsevier.com/locate/ijgo CLINICAL ARTICLE Female autonomy and reported abortion-seeking in Ghana, West Africa Sarah D. Rominski a,⁎, Mira Gupta a,RaymondAborigob,c, Phillip Adongo d, Cyril Engman e, Abraham Hodgson b,f,CherylMoyera,g a Global REACH, University of Michigan Medical School, Ann Arbor, USA b Navrongo Health Research Centre, Ghana Health Service, Navrongo, Ghana c Jeffrey Cheah School of Medicine and Health Sciences, MONASH University, Sunway Campus, Subang Jaya, Malaysia d Department of Social and Behavioural Sciences, School of Public Health, University of Ghana, Accra, Ghana e Department of Pediatrics and Maternal Child Health, Schools of Medicine and Public Health, University of North Carolina, Chapel Hill, USA f Ghana Health Service, Accra, Ghana g Department of Medical Education, University of Michigan Medical School, Ann Arbor, USA article info abstract Article history: Objective: To investigate factors associated with self-reported pregnancy termination in Ghana and thereby ap- Received 4 October 2013 preciate the correlates of abortion-seeking in order to understand safe abortion care provision. Received in revised form 6 March 2014 Methods: In a retrospective study, data from the Ghana 2008 Demographic and Health Survey were used to inves- Accepted 7 May 2014 tigate factors associated with self-reported pregnancy termination. Variables on an individual and household level were examined by both bivariate analyses and multivariate logistic regression. A five-point autonomy Keywords: scale was created to explore the role of female autonomy in reported abortion-seeking behavior.