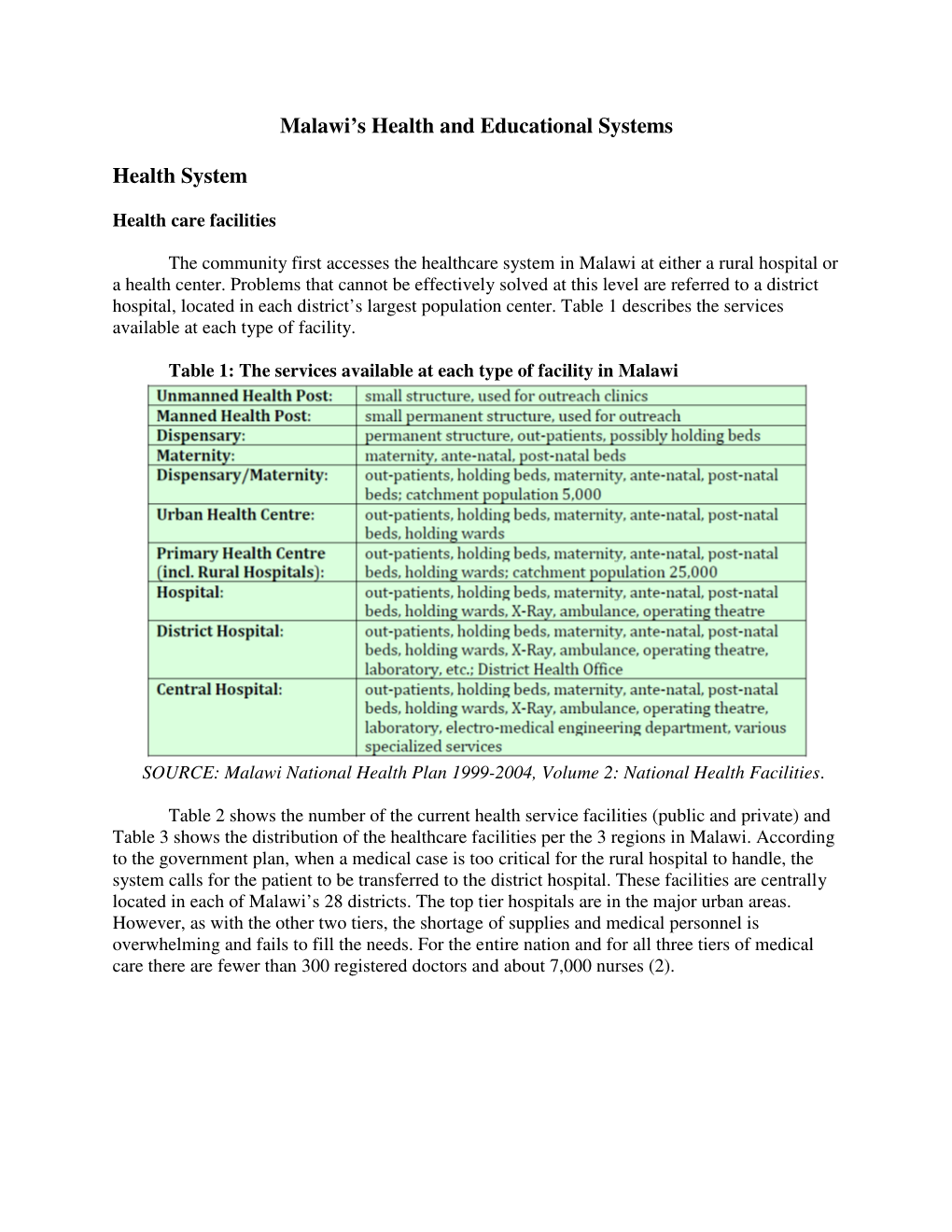
Malawi's Health and Educational Systems Health System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Partners in Health in Neno District, Malawi
C ASES IN G LOBAL H EALTH D ELIVERY GHD-029 JULY 2013 Partners In Health in Neno District, Malawi In May 2012, Ophelia Dahl, cofounder and executive director of Partners In Health (PIH), an international health nongovernmental organization (NGO), was preparing for the Board of Directors’ meeting. On the agenda was an in-depth review of Abwenzi Pa Za Umoyo (the translation of “Partners In Health” in Chichewa; APZU), PIH’s sister site in Neno District, Malawi. Dahl reflected on her two trips to Neno, the first in 2008 and the second in 2011. She recalled how, in 2008, she had traveled for hours along a worn-out dirt road and visited public health clinics that seemed neglected. In fact, the district as a whole seemed abandoned. In 2011, she visited Neno’s lively primary school, ate at a local restaurant, and got cash out of an ATM machine. With limited primary data from the field, Dahl wondered how to demonstrate the changes that had occurred during this time period to the Board of Directors. What was APZU’s impact? Overview of Malawi The Republic of Malawi is a landlocked, democratic country in southeastern Africa and one of the most densely populated on the continent (see Exhibit 1 for map of Malawi). Zambia, Tanzania, Mozambique, and Lake Malawi border Malawi’s 118,484 square kilometers. Major religions are Christianity (82.7%) and Islam (13%).1 Official languages are English and Chichewa. History The arrival of Scottish missionary and explorer David Livingstone in 1859 marked present-day Malawi’s first significant Western contact. -
Effective Health Financing Models in SADC: Three Case Studies
Effective health financing models in SADC: Three case studies Prepared for FinMark Trust by Insight Actuaries and Consultants Date: April 2016 Authors: Shivani Ranchod (FASSA) Daniël Erasmus (FIFoA) Matan Abraham Julian Bloch Kudzai Chigiji Kathryn Dreyer (FASSA) 1 | P a g e Table of Contents 1. Executive Summary ............................................................................................................................ 4 2. Introduction ......................................................................................................................................... 7 2.1. Background to the study ......................................................................................................... 7 2.2. Selection process and criteria .................................................................................................. 8 3. Sema Doc - Kenya .............................................................................................................................. 8 3.1. Overview of country context ................................................................................................... 9 3.1.1. The Kenyan population ................................................................................................... 9 3.1.2. Healthcare and health insurance in Kenya .................................................................... 10 3.1.3. Mobile technology ........................................................................................................ 12 3.2. Benefit structure -

Informal Payments in Public Hospitals of Malawi - a Case of Kamuzu Central Hospital
Informal Payments in Public Hospitals of Malawi - A Case of Kamuzu Central Hospital Annette Mphande Namangale ( [email protected] ) University of Malawi College of Medicine https://orcid.org/0000-0003-0639-5501 Isabel Kazanga Chiumia University of Malawi College of Medicine Research Keywords: Malawi, Informal Payment, Public Health System, Access to Healthcare Posted Date: January 11th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-141193/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Informal Payments in Public Hospitals of Malawi – A Case of Kamuzu Central Hospital Annette Mphande Namangale1, Isabel Kazanga Chiumia2 Affiliation: School of Public Health, College of Medicine, University of Malawi, Malawi Co-author's email: [email protected] Corresponding author’s email: [email protected] Address: P.O Box 30356, Lilongwe 3, Malawi Abstract Background: Informal payments in public health facilities act as a barrier to accessing quality healthcare services especially for the poor people. There is growing evidence that in most low- income countries, most poor people are unable to access quality health care services due to demands for payments for services that should be accessed for free. This research was aimed at investigating informal payments for health care services at Kamuzu Central Hospital, one of the referral public hospitals in Malawi. Results of this study provide evidence on the magnitude and factors influencing informal payments in Malawi so that relevant policies and strategies may be made to address this problem. Methods: The study employed a mixed methods research design. The quantitative study component had a sample size of 295 patients and guardians at Kamuzu Central Hospital (KCH). -

Community-Based Distribution of Injectable Contraceptives in Malawi
COMMUNITY-BASED DISTRIBUTION OF INJECTABLE CONTRACEPTIVES IN MALAWI APRIL 2009 This publication was produced for review by the U.S. Agency for International Development (USAID). It was prepared by Faye Richardson, Maureen Chirwa, Margot Fahnestock, Meghan Bishop, Priya Emmart, and Bridget McHenry of the Health Policy Initiative, Task Order 1. Suggested citation: Richardson, F., M. Chirwa, M. Fahnestock, M. Bishop, P. Emmart, and B. McHenry. 2009. Community-based Distribution of Injectable Contraceptives in Malawi. Washington, DC: Futures Group International, Health Policy Initiative, Task Order 1. The USAID | Health Policy Initiative, Task Order 1, is funded by the U.S. Agency for International Development under Contract No. GPO-I-01-05-00040-00, beginning September 30, 2005. Task Order 1 is implemented by Futures Group International, in collaboration with the Centre for Development and Population Activities (CEDPA), White Ribbon Alliance for Safe Motherhood (WRA), Futures Institute, and Religions for Peace. COMMUNITY-BASED DISTRIBUTION OF INJECTABLE CONTRACEPTIVES IN MALAWI APRIL 2009 The views expressed in this publication do not necessarily reflect the views of the U.S. Agency for International Development or the U.S. Government. CONTENTS Acknowledgments ......................................................................................................................................iv Executive Summary ....................................................................................................................................v -
The Local Governance Performance Index (LGPI) in Malawi: Selected Findings on Health
The Program on Governance and Local Development The Local Governance Performance Index (LGPI) in Malawi: Selected Findings on Health Report November 2016 SERIES 2016:7 Acknowledgements This project reflects fruitful collaboration of researchers at the Christian Michelson Institute, including Ragnhild Muriaas, Lise Rakner and Vibeke Wang; the Institute for Public Opinion and Research, including Asiyati Chiweza, Boniface Dulani, Happy Kayuni, Hannah Swila and Atusaye Zgambo; and the Program on Governance and Local Development, including Adam Harris, Kristen Kao, Ellen Lust, Maria Thorson, Jens Ewald, Petter Holmgren, Pierre Landry and Lindsay Benstead during implementation, and in addition Ruth Carlitz, Sebastian Nickel, Benjamin Akinyemi, Laura Lungu and Tove Wikehult in the process of data cleaning and analysis. We gratefully recognize the hard work of colleagues at the Institute for Public Opinion and Research who lead the survey research teams. These include, Ellasy Chimimba, Grace Gundula, Steve Liwera, Shonduri Manda, Alfred Mangani, Razak Mussa, Bernard Nyirenda, Charles Sisya and Elizabeth Tizola. We also thank Jane Steinberg, who provided excellent and timely editing of this report. Finally, we reserve special recognition for Laura Lungu and Kristen Kao, who led this report. This project has been made possible with the financial support of the Moulay Hicham Foundation, the Carnegie Corporation of New York, The World Bank and Yale University, which funded development of the Local Governance Performance Index, and the Swedish Research Council and the Research Council of Norway, which funded implementation in Norway. We are grateful for their support. Executive Summary Malawi is one of the poorest countries in the world. Gross national income per capita is just $747 U.S.,1 and nearly 51 percent of the population resides below the national poverty line.2 As such, much of the population suffers from health ailments. -

Accountability and Redress for Discrimination in Healthcare in Botswana, Malawi and Zambia
Accountability and redress for discrimination in healthcare in Botswana, Malawi and Zambia SOUTHERN AFRICA LITIGATION CENTRE Accountability and redress for discrimination in healthcare in Botswana, Malawi and Zambia August 2016 SALC REPORT Accountability and redress for discrimination in healthcare in Botswana, Malawi and Zambia © 2016 Southern Africa Litigation Centre ISBN Print: 978-0-620-72928-4 ISBN Digital: 978-0-60-72930-7 About the Southern Africa Litigation Centre The Southern Africa Litigation Centre (SALC), established in 2005, aims to provide support – both technical and financial – to human rights and public interest initiatives undertaken by domestic lawyers in southern Africa. SALC works in Angola, Botswana, Democratic Republic of Congo, Lesotho, Malawi, Mozambique, Namibia, Swaziland, Zambia and Zimbabwe. Its model is to work in conjunction with domestic lawyers in each jurisdiction who are litigating public interest cases involving human rights or the rule of law. SALC supports these lawyers in a variety of ways, as appropriate, including providing legal research and drafting, training and mentoring, and monetary support. SALC’s objectives include the provision of training and the facilitation of legal networks within the region. Authorship and acknowledgement This report was researched and written by Annabel Raw, Health Rights Lawyer at SALC, with data sourced from consultants Chipo Nkhata, Monica Tabengwa and Ketsile Molokomme, and from the Botswana Council for the Disabled (Dorcas Taukobong), the Centre for Human Rights Education, Advice and Assistance (Victor Mhango and Chikondi Chijozi Ngwira), the Coalition of Women Living with HIV and AIDS, Malawi (Annie Banda), the Centre for the Development of People, Malawi (Victor Gama and Gift Trapence), Disability Rights Watch (Wamundila Waliuya and Bruce Chooma), Friends of Rainka (Henry Muzawandile), the International Coalition of Women, Zambia (Clementine Mumba), Lesbian Gays and Bisexuals of Botswana (Bradley Fortuin), Sisonke Botswana (Tosh Legoreng), and Transbantu Zambia (Sean Reggee). -

Examining Equity in Out-Of-Pocket Expenditures and Utilization of Healthcare Services in Malawi
AN ABSTRACT OF THE DISSERTATION OF Ruth Hope Mwandira for the degree of Doctor of Philosophy in Public Health presented on May 31, 2011. Title: Examining Equity in Out-of-Pocket Expenditures and Utilization of Healthcare Services in Malawi Abstract approved: _______________________________________________________________ Chunhuei Chi Best international health practice requires that all people benefit equally from health care services regardless of their socio-economic status and that healthcare payments be based on ability to pay. Although recent household surveys in Malawi show progress in a number of health indicators population averages, many inequalities in health outcomes still exist or are widening among households stratified by socioeconomic and geographical location variables. Inequalities in out-of-pocket expenditures (OOPEs) for healthcare and how they influence utilization of healthcare services are of particular interest to policy makers as they ultimately affect overall health of households. The rationale for this study is that analysis of inequities in healthcare between socioeconomic groups can help to unmask intra-group and between groups’ inequities hidden in national population averages. The study’s three main papers examined equity in households’ out-of-pocket healthcare payments and utilization of medical care. The study adopted the widely used economic frameworks and techniques developed by O’Donnell et al (2008) for analyzing health equity using household data. These economic frameworks focus on the notion of equal treatment for equal need and that payment for healthcare should be according to ability to pay. The Malawi Integrated Household Survey 2(2005) (MIHS2) was the main dataset used in the analysis. The MIHS2 is currently the only dataset that presents inequalities in healthcare expenditures at the household level in Malawi. -
![Global Trends in Care Seeking and Access to Diagnosis and Treatment of Childhood Illnesses [WP116]](https://docslib.b-cdn.net/cover/7884/global-trends-in-care-seeking-and-access-to-diagnosis-and-treatment-of-childhood-illnesses-wp116-1567884.webp)
Global Trends in Care Seeking and Access to Diagnosis and Treatment of Childhood Illnesses [WP116]
DHS WORKING PAPERS Global Trends in Care Seeking and Access to Diagnosis and Treatment of Childhood Illnesses Adam Bennett Thom Eisele Joseph Keating Josh Yukich 2015 No. 116 DEMOGRAPHIC AND March 2015 HEALTH This document was produced for review by the United States Agency for International Development. SURVEYS Global Trends in Care Seeking and Access to Diagnosis and Treatment of Childhood Illnesses Adam Bennett1 Thom Eisele2 Joseph Keating2 Josh Yukich2 ICF International Rockville, Maryland, USA March 2015 1Malaria Elimination Initiative, Global Health Group, University of California, San Francisco 2Center for Applied Malaria Research and Evaluation, Tulane University School of Public Health and Tropical Medicine Corresponding author: Thom Eisele, Center for Applied Malaria Research and Evaluation, Department of Global Health Systems and Development, Tulane University School of Public Health and Tropical Medicine, 1440 Canal Street, Suite 2200, New Orleans, LA 70112 USA; Phone: +1-504-988-3542; Fax: +1-504-988-1568; Email: [email protected] Acknowledgments: Lia Florey (ICF International), Erin Eckert (USAID), and Rene Salgado (USAID) are thanked for their review and comment on the draft report. Zhe Xu (Tulane University) is sincerely thanked for his help with data management and data processing. Editor: Sidney Moore Document Production: Natalie La Roche This study was carried out with support provided by the United States Agency for International Development (USAID) through The DHS Program (#GPO–C–00–08–00008–00). The views expressed are those of the authors and do not necessarily reflect the views of USAID or the United States Government. The DHS Program assists countries worldwide in the collection and use of data to monitor and evaluate population, health, and nutrition programs. -

Analyzing Tuberculosis Diagnosis and Treatment in Kasungu, Malawi
Colby College Digital Commons @ Colby Honors Theses Student Research 2016 Analyzing Tuberculosis Diagnosis and Treatment in Kasungu, Malawi Andrew Currier Colby College Follow this and additional works at: https://digitalcommons.colby.edu/honorstheses Part of the International Public Health Commons Colby College theses are protected by copyright. They may be viewed or downloaded from this site for the purposes of research and scholarship. Reproduction or distribution for commercial purposes is prohibited without written permission of the author. Recommended Citation Currier, Andrew, "Analyzing Tuberculosis Diagnosis and Treatment in Kasungu, Malawi" (2016). Honors Theses. Paper 836. https://digitalcommons.colby.edu/honorstheses/836 This Honors Thesis (Open Access) is brought to you for free and open access by the Student Research at Digital Commons @ Colby. It has been accepted for inclusion in Honors Theses by an authorized administrator of Digital Commons @ Colby. Analyzing Tuberculosis Diagnosis and Treatment in Kasungu, Malawi Andy Currier Environmental Studies Program Colby College Waterville, Maine May 6, 2016 A thesis submitted to the faculty of the Environmental Studies Program in partial fulfillment of the graduation requirements for the Degree of Bachelor of Arts with honors in Environmental Studies ____________________ __________________ _______________________ Gail Carlson, Advisor Philip Nyhus, Reader William McDowell, Reader Copyright © (2016) by the Environmental Studies Program, Colby College. All rights reserved. ii ABSTRACT Despite Tuberculosis (TB) being a highly curable disease, it continues to result in over 5% of deaths in the Sub-Saharan African country of Malawi. Coupled with HIV, the disease remains one of the leading causes of death in Malawi. In the summer of 2015, I joined a research team from Partners in Hope to conduct a survey evaluating the health centers that provide TB care in the Kasungu region of Malawi. -

The Implications of Contracting out Health Care Provision to Private Not-For
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Queen Margaret University eResearch THE IMPLICATIO1S OF CO1TRACTI1G OUT HEALTH CARE PROVISIO1 TO PRIVATE 1OT-FOR- PROFIT HEALTH CARE PROVIDERS: THE CASE OF SERVICE LEVEL AGREEME1TS I1 MALAWI ELVIS SITITHA1A MPAKATI GAMA Thesis submitted in fulfilment of the requirements for the degree of Doctor of Philosophy in Health economics QUEE1 MARGARET U1IVERSITY 2013 1 Declaration I have read and understood the school’s definition of plagiarism and cheating given in the research degrees handbook. I hereby declare that this thesis is my own work and that, to the best of my knowledge, it contains no previously published or written by another person nor material which to a substantial extent has been accepted for the award of any other degree of the university or other institute of higher learning, except where due acknowledgment has been made in the text. Signed.........Elvis Mpakati Gama.......................Date......18 December 2013.......................... Elvis Sitithana Mpakati Gama 2 “The primary determinants of disease are mainly economic and social, and therefore its remedies must also be economic and social. Medicine and politics cannot and should not be kept apart” (Geoffrey Rose- The strategy of preventive medicine, Oxford, Oxford University Press, 1992, page 129) 3 ABSTRACT Background: The Malawi government in 2002 embarked on an innovative health care financing mechanism called Service Level Agreement (SLA) with Christian Health Association of Malawi (CHAM) institutions that are located in areas where people with low incomes reside. The rationale of SLA was to increase access, equity and quality of health care services as well as to reduce the financial burden of health expenditure faced by poor and rural communities. -

Lives of Malawian Nurses: Stories Behind the Statistics
Lives of Malawian nurses: Stories behind the statistics Astrida Ieva Grigulis Thesis submitted for the degree of Doctor of Philosophy University College London Centre for International Health and Development UCL Institute of Child Health Declaration I, Astrida Grigulis, confirm that the work presented in this thesis is my own. Where information has been derived from other sources, I confirm that this has been indicated in the thesis. Signed: 2010 2 Abstract Malawi lost a significant proportion of its most experienced and qualified nurses to international migration between 2000 and 2005. The lure of overseas life and poor conditions of service at home caused an unprecedented wave of migration. This thesis is about the experiences and motivations of nurses who left Malawi, and of those who stayed behind. Using a qualitative biographical method to examine their experiences along a timeline of key life events, I develop a comprehensive picture of nurse migration. The findings show that nurses’ decisions and experiences have been shaped by demographic and political shifts and by a strong culture of family. Population growth has increased competition for higher education and caused a palpable shift in motives for becoming a nurse. Prospective students now see nurse training as a means to a guaranteed career, or to a marketable qualification which can lead to alternative employment. Working conditions have not improved despite numerous government initiatives, and nurses are still leaving for greener pastures. Many now move to Malawian Non-Governmental Organisations, but before 2005 nurses were able to take advantage of the United Kingdom’s (UK) active recruitment strategy. -

Strengthening Primary Health Care at District-Level in Malawi-Determining
Makaula et al. BMC Health Services Research (2019) 19:509 https://doi.org/10.1186/s12913-019-4341-5 RESEARCHARTICLE Open Access Strengthening primary health care at district-level in Malawi - determining the coverage, costs and benefits of community- directed interventions Peter Makaula1* , Mathias Funsanani1, Kondwani Chidzammbuyo Mamba2,3, Janelisa Musaya3 and Paul Bloch4 Abstract Background: Community-Directed Interventions (CDI) is a participatory approach for delivery of essential healthcare services at community level. It is based on the values and principles of Primary Health Care (PHC). The CDI approach has been used to improve the delivery of services in areas that have previously applied Community-Directed Treatment with ivermectin (CDTi). Limited knowledge is available about its added value for strengthening PHC services in areas without experience in CDTi. This study aimed to assess how best to use the CDI approach to strengthen locally identified PHC services at district level. Methods: This was a comparative intervention study carried out over a period of 12 months and involving four health centres and 16 villages assigned to 1) a conventional Essential Health Package (EHP)/PHC approach at health centre level or 2) an EHP/PHC/CDI approach at community level in addition to EHP/PHC at health centre level. Communities decided which intervention components to be included in the intervention. These were home management of malaria (HMM), long lasting insecticide treated nets (LLIN), vitamin A and treatment against schistosomiasis. The outcomes of the two strategies were compared quantitatively after the intervention was completed with regard to intervention component coverage and costs. Qualitative in-depth interviews with involved health professionals, implementers and beneficiaries were carried out to determine the benefits and challenges of applied intervention components.