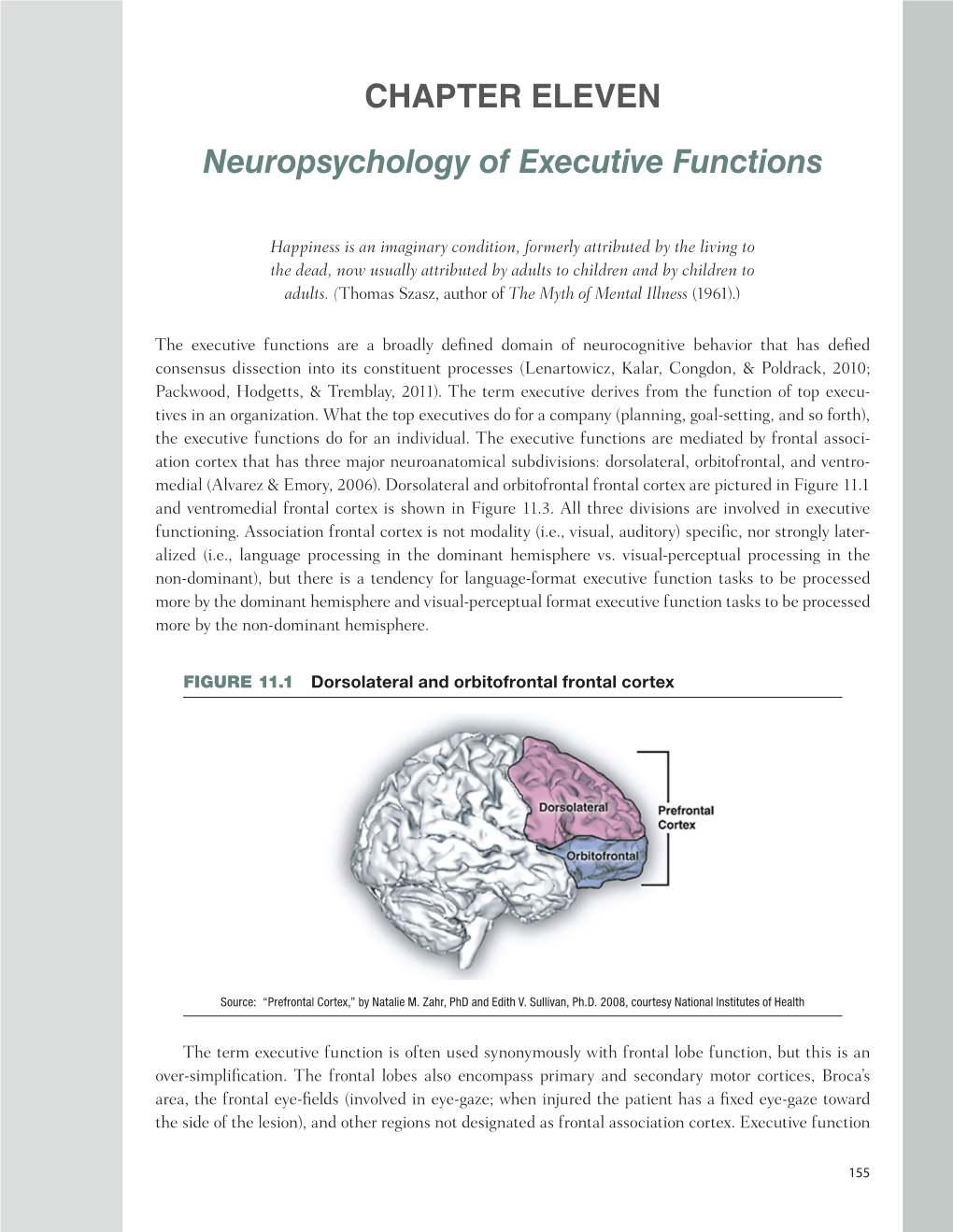
CHAPTER ELEVEN Neuropsychology of Executive Functions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

NEGLECT and ANOSOGNOSIA a CHALLENGE for PSYCHOANALYSIS Psychoanalytic Treatment of Neurological Patients with Hemi-Neglect
Psychoanalytische Perspectieven, 2002, 20, 4: 611-631 NEGLECT AND ANOSOGNOSIA A CHALLENGE FOR PSYCHOANALYSIS Psychoanalytic treatment of neurological patients with hemi-neglect Klaus Röckerath1 Introduction This paper deals with two phenomena often observed in patients with a lesion to the right hemisphere of the brain: neglect and anosognosia. Fol- lowing an overview of the neglect syndrome from a neuroscientific per- spective I will present preliminary results and hypotheses formulated by our group based on the psychoanalytic treatment of seven such patients. It may be somewhat unusual for neurologically impaired patients to undergo psychoanalytic treatment. But in recent years, a combined effort to under- stand the underlying mechanisms of psychic phenomena has evolved in psychoanalysis and the neurosciences. Hence, the field of neuro-psycho- analysis established itself, studying the psychic implications of neurologi- cal damage in order to understand and gain insight into the "psychic appa- ratus", as constructed by Freud, from a different point of view. It is well known that Freud, a trained neurologist, hoped that one day the mecha- nism of psychic functions would be understood from a neurologist's point of view. He was convinced that the answer to the psychic problems he encountered with his patients must be rooted in the matter of the mind: the brain. That is why groups of psychoanalysts and neuroscientists all over the world have begun to exchange news and views about their common interest: the human mind. Both sciences basically deal with the same object. One way psychoanalysts can contribute is by looking at neurologically impaired patients in a psychoanalytic framework to establish what is dif- 1.The Neurops ychoanalytic Study Group Frankfurt/Cologne, Germany. -
Amsterdam Executive Functions
Executive function and behaviour Masud Husain Professor of Neurology & Cognitive Neuroscience, University of Oxford Lead for Neurological Conditions, Oxford NIHR Biomedical Research Centre Supported by The Wellcome Trust What are executive functions? They’re functions that are thought to be deployed when control needs to be exerted § Typically described as ‘supervisory’ or ‘controlling’ § Deployed when a situation is novel or difficult § When you need to pay attention because there isn’t an automatic / habitual response to the problem or the automatic response would be inappropriate Example: When the phone rings in someone else’s house, you don’t pick it up, even though the automatic tendency in your own home is to do so § When several cognitive processes need to be co-ordinated § Or when you need to shift from one type of process to another Orchestration of behaviour They’re functions that are thought to be deployed when control needs to be exerted § Initiate § Maintain / Sustain / Invigorate / Energise § Stop ongoing action § Inhibit inappropriate behaviour or prepotent response § Switch to a different behavioural set / set shifting / mental flexibility § Working memory: manipulation of items in short term memory § Monitor consequences of behaviour / error monitoring § Planning and prioritization § Multi-tasking § Social / emotional engagement When executive function breaks down There might be profound consequences Executive function Associated executive dysfunction Clinical presentation Task initiation Reduced self-generated behaviours -

Parietal Lobes: Evolution, Neuroanatomy, and Function
Parietal Lobes: Evolution, Neuroanatomy, and Function Charles J. Vella, PhD May 3, 2017 Intent of this lecture Parietal lobe syndromes are mostly domain of neurology, not NP But these syndromes will affect NP performance on multiple tests There are lots of anatomical references: you can always use the pdf online as reference text There are lots of unusual, sometimes rare, syndromes My objective is to have you be aware of when parietal lobe functioning is involved in something you are seeing clinically in a patient The discovery of the Parietal Lobe Franciscus Sylvius (1614-1672) Physician, physiologist, anatomist, and chemist Professor at the University of Leidon (1641) Was in the chemistry lab at the University when he discovered the deep cleft (Sylvian Fissure). History of Parietal Lobe Discovery In 1874 Bartholow recorded odd sensation from legs on stimulating post central gyrus through skull wounds Djerine – alexia , agraphia -- angular gyrus lesion Hugo Liepmann--- ideomotor & ideational apraxia in (L) sided lesion Cushing in 1909 --- Electrical stimulation in conscious human beings –– mainly tactile hallucinations; first homunculus Critchley (1953) – 1st monograph on “ The Parietal Lobes” Siegel et al. (2003) – “The Parietal Lobes” Macdonald Critchley: Parietal Lobes Parietal Lobes No independent existence as anatomical / physiological unit Operates in conjunction with brain as a whole Strategically situated between other lobes Greater variety of clinical manifestations than rest of the hemisphere Ignored in -
The Right Hemisphere and Disorders of Cognition and Communication
The Right Hemisphere and Disorders of Cognition and Communication Theory and Clinical Practice The Right Hemisphere and Disorders of Cognition and Communication Theory and Clinical Practice Margaret Lehman Blake, PhD 5521 Ruffin Road San Diego, CA 92123 e-mail: [email protected] Website: http://www.pluralpublishing.com Copyright © 2018 by Plural Publishing, Inc. Typeset in 10.5/14 Palatino by Flanagan’s Publishing Services, Inc. Printed in the United States of America by McNaughton & Gunn All rights, including that of translation, reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, recording, or otherwise, including photocopying, recording, taping, Web distribution, or information storage and retrieval systems without the prior written consent of the publisher. For permission to use material from this text, contact us by Telephone: (866) 758-7251 Fax: (888) 758-7255 e-mail: [email protected] Every attempt has been made to contact the copyright holders for material originally printed in another source. If any have been inadvertently overlooked, the publishers will gladly make the necessary arrangements at the first opportunity. Library of Congress Cataloging-in-Publication Data: Names: Blake, Margaret Lehman, author. Title: The right hemisphere and disorders of cognition and communication : theory and clinical practice / Margaret Lehman Blake. Description: San Diego, CA : Plural, [2018] | Includes bibliographical -

Cerebral Localization
CEREBRAL LOCALIZATION PARIETAL LOBE SIGNS December 18,2013 PARIETAL LOBE DR UTKARSH BHAGAT DR UTKARSH File:Gray726,727.svg 2 December 18,2013 BROADMANN AREAS DR UTKARSH BHAGAT DR UTKARSH wikimedia.org/wikipedia/commons/0/09 3 December 18,2013 PARIETAL LOBE ¢ Special high order sensory organ ¢ Locus of transmodal ( intersensory) integration BHAGAT DR UTKARSH ¢ Awareness of one’s body & its relation to extra personal space and of objects in the environment to each other. 4 December 18,2013 LESIONS OF PARIETAL LOBE Post central gyrus DR UTKARSH BHAGAT DR UTKARSH ¢ Simple somatosensory disturbances ¢ Contra lateral sensory loss (object recognition > position sense > touch > pain and temperature, vibration); tactile extinction ¢ Contra lateral pain, paresthesias Mesial aspect (cuneus) ¢ Transcortical sensory aphasia? (dominant hemisphere) ¢ Attentional disorder 5 December 18,2013 LESIONS OF PARIETAL LOBE ¢ In general, left hemisphere is dominant for thought and DR UTKARSH BHAGAT DR UTKARSH reasoning, analytic and mathematical skills the right hemisphere is dominant for tasks requiring spatial and constructional skills, as well as for directed attention and body image 6 December 18,2013 LESIONS OF PARIETAL LOBE Lateral aspect (superior and inferior parietal lobules) ¢ Dominant hemisphere DR UTKARSH BHAGAT DR UTKARSH ¢ Parietal apraxia (higher lesion) ¢ Finger agnosia ¢ Acalculia ¢ Right-left disorientation ¢ Literal alexia (supramarginal gyrus) ¢ Conduction aphasia 7 December 18,2013 LESIONS OF PARIETAL LOBE ¢ Nondominant hemisphere ¢ Anosognosia DR UTKARSH BHAGAT DR UTKARSH ¢ Hemispatial neglect (sensory inattention) ¢ Constructional apraxia ¢ Dressing apraxia ¢ Loss of topographical memory ¢ Allesthesia ¢ Hemisomatognosia ¢ Asymbolia for pain 8 December 18,2013 ANOSOGNOSIA ¢ Patients fail to recognize the hemiplegic limbs as belonging to them (anosognosia) DR UTKARSH BHAGAT DR UTKARSH ¢ and confabulate when asked whom they belong to (they often ascribe them to the examiner: somatoparaphrenia). -
The Neurologic Diagnosis
The Neurologic Diagnosis A Practical Bedside Approach Jack N. Alpert Second Edition 123 The Neurologic Diagnosis Jack N. Alpert The Neurologic Diagnosis A Practical Bedside Approach Second Edition Jack N. Alpert Department of Neurology University of Texas Medical School at Houston Houston, TX USA ISBN 978-3-319-95950-4 ISBN 978-3-319-95951-1 (eBook) https://doi.org/10.1007/978-3-319-95951-1 Library of Congress Control Number: 2018956294 © Springer Nature Switzerland AG 2019 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. -

Study of Anosognosia
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.41.6.548 on 1 June 1978. Downloaded from Journal ofNeurology, Neurosurgery, andPsychiatry, 1978, 41, 548-555 Study of anosognosia JOHN CUTTING From the Institute of Psychiatry and King's College Hospital, London SUMMARY Anosognosia (denial of weakness) and "anosognosic phenomena" (other abnormal attitudes to a weak limb) were studied in 100 acute hemiplegics. Both conditions were associated with lesions of either hemisphere. Apathy, visual field defect, and impaired picture identifica- tion were particularly prominent in anosognosia. A failure to integrate information from one side of the body was regarded as fundamental to the condition; explanations in terms of "unilateral neglect" and "agnosia" are discussed. Babinski introduced the word "anosognosia" in have attributed to right hemisphere damage a pre- 1914 as a description of patients who ignored their eminent role in its development (Bogen, 1969; hemiplegia. In current usage the term embraces Galin, 1974). It is true that anosognosia for a right Protected by copyright. a variety of abnormal attitudes. Chief among these hemiplegia has only rarely been recorded. Exclud- is an explicit verbal denial that the limb is weak. ing left handed patients and those with bilateral Some patients, although admitting to their dis- lesions, only four case reports remain (Von Hagen ability on direct questioning, minimise its extent, and Ives, 1937; Nathanson et al., 1952; Weinstein often in a jocular fashion (anosodiaphoria, and Kahn, 1955; Welman, 1969). However, the Babinski, 1914). Yet others experience the limb presence of aphasia in patients with left hemis- as strange or not belonging to them, or even phere lesions complicates the issue. -

Treating Unawareness After Stroke 1 Running Head: MANAGING
Treating unawareness after stroke 1 Running Head: MANAGING UNAWARENESS AFTER STROKE Unawareness after stroke: A review and practical guide to understanding, assessing, and managing anosognosia for hemiplegia. Paul M. Jenkinson1, Catherine Preston2, & Simon J. Ellis3 1School of Psychology, University of Hertfordshire, UK. 2School of Social Sciences, Nottingham Trent University, UK. 3Department of Neurology, University Hospital of North Staffordshire, UK. Correspondence concerning this article should be addressed to: P. M. Jenkinson, School of Psychology, University of Hertfordshire, College Lane, Hatfield, AL10 9AB. Tel: 01707 284618. Email: [email protected]. Keywords: unawareness; anosognosia for hemiplegia; assessment; treatment; rehabilitation. Treating unawareness after stroke 2 Abstract How should stroke patients with poor motor awareness be managed? This question is important because unawareness (or anosognosia) is related to poor rehabilitation and prognosis. This narrative review provides a guide for clinicians and (applied) academics to understanding, assessing and managing anosognosia. Questions addressed are: What is anosognosia? What causes anosognosia? How can anosognosia be assessed? And how can anosognosia be managed? We suggest that anosognosia is a multifaceted disorder, with diverse neuroanatomical and psychopathological origins. Assessment should measure various aspects of awareness, and management should be multidimensional to address problems with motor function, awareness, and emotional / motivational disturbance. Treating unawareness after stroke 3 Unawareness after stroke: A review and practical guide to understanding, assessing, and managing anosognosia for hemiplegia. 1. Introduction Providing care for patients who are unaware of their motor deficit is a difficulty frequently encountered by health professionals working with stroke patients. Unawareness is a considerable problem for rehabilitation, leading to sub-optimal benefits and significantly poorer prognosis (Appelros, Karlsson, Seiger, & Nydevik, 2002). -

Unilateral Neglect: Assessment and Rehabilitation
International Journal of Neuroscience and Behavioral Science 4(1): 1-10, 2016 http://www.hrpub.org DOI: 10.13189/ijnbs.2016.040101 Unilateral Neglect: Assessment and Rehabilitation Richard P. Conti1,*, Jacqueline M. Arnone2 1School of Psychology, Kean University, United States 2School of Nursing, Kean University, United States Copyright©2016 by authors, all rights reserved. Authors agree that this article remains permanently open access under the terms of the Creative Commons Attribution License 4.0 International License Abstract Over 795,000 individuals in the U.S. suffer Moreover, stroke expenditures in the United States are an from strokes annually, with 610,000 accounting for first estimated $34 billion annually [4].This sum includes the attacks. Stroke represents the fifth leading cause of death and charges for health care services, prescriptions to treat stroke, resulting long-term disability in the United States. Unilateral and lost productivity due to morbidity and mortality [3,5]. neglect (UN) is a disabling characteristic of stroke, occurring Unilateral Neglect (UN) is a disabling characteristic of from lesion damage to one hemisphere of the brain. stroke, as a result of lesion damage to one hemisphere of the Individuals with UN do not respond normally to objects, brain [6,7]. This disorder is a multifaceted and complex stimuli, and people located to their contralesional side. Right neurological condition in which an individual fails to hemispheric lesions exhibit the greatest impairment. respond to stimuli in the contralesional hemispace, which Incidence rates of UN vary from 13%-81%. Impairment of cannot be explained by primary sensory or motor defects this condition impedes an individual’s capacity to execute [8,9]. -

Anosognosia for Hemiplegia: a Clinical-Anatomical Prospective Study
doi:10.1093/brain/awq297 Brain 2010: 133; 3578–3597 | 3578 BRAIN A JOURNAL OF NEUROLOGY Anosognosia for hemiplegia: a clinical-anatomical prospective study Roland Vocat,1 Fabienne Staub,2 Tiziano Stroppini2 and Patrik Vuilleumier1,3 1 Laboratory for Behavioural Neurology and Imaging of Cognition, Department of Neuroscience and Clinic of Neurology, University of Geneva School of Medicine, 1211 Geneva, Switzerland 2 Department of Neurology, Centre Hospitalier Universitaire Vaudois (CHUV), 1011 Lausanne, Switzerland 3 Centre for Neuroscience, University of Geneva, 1211 Geneva, Switzerland Correspondence to: Roland Vocat, Neurology and Imaging of Cognition, Department of Neurology, Downloaded from University Hospital (HUG), 24 rue Micheli-du-Crest, CH-1211 Geneva, Switzerland E-mail: [email protected] brain.oxfordjournals.org Anosognosia for hemiplegia is a common and striking disorder following stroke. Because it is typically transient and variable, it remains poorly understood and has rarely been investigated at different times in a systematic manner. Our study evaluated a at University of Geneva on July 4, 2011 prospective cohort of 58 patients with right-hemisphere stroke and significant motor deficit of the left hemibody, who were examined using a comprehensive neuropsychological battery at 3 days (hyperacute), 1 week (subacute) and 6 months (chronic) after stroke onset. Anosognosia for hemiplegia was frequent in the hyperacute phase (32%), but reduced by almost half 1 week later (18%) and only rarely seen at 6 months (5%). Anosognosia -

ANOSOGNOSIA for HEMIPLEGIA Theoretical, Clinical, and Neural Aspects
AHP: THEORETICAL, CLINICAL, AND NEURAL ASPECTS 1 ANOSOGNOSIA FOR HEMIPLEGIA Theoretical, Clinical, and Neural Aspects Bachelor Degree Project in Cognitive Neuroscience 15 ECTS Spring term 2011 Joel Gerafi Supervisor: Judith Annett Examiner: Pilleriin Sikka AHP: THEORETICAL, CLINICAL, AND NEURAL ASPECTS 2 Anosognosia for Hemiplegia: Theoretical, Clinical, and Neural Aspects Submitted by Joel Gerafi to the University of Skövde as a final year project towards the degree of B.Sc. in the School of Humanities and Informatics. The project has been supervised by Judith Annett. 10/6/2011 I hereby certify that all material in this final year project which is not my own work has been identified and that no work is included for which a degree has already been conferred on me. Signature: ___________________________________________ AHP: THEORETICAL, CLINICAL, AND NEURAL ASPECTS 3 Abstract Anosognosia for hemiplegia (AHP) is relatively common among patients who suffer from a stroke. It is characterized as a denial of bodily paralysis and the complexity of studying it is evident. Anosognosia is a neuropsychological deficit of self-awareness and most frequently associated with both cortical and subcortical lesions distributed within the right hemisphere, resulting in a left hemiplegia. The purpose of this review is to provide a comprehensive overview of AHP by presenting theoretical, clinical, and neural aspects. Different diagnostic procedures have attempted to clinically evaluate patients with AHP. The timing of assessment and the characteristic differences between these procedures are crucial factors to consider. Various theories regarding the underlying mechanisms of AHP are also discussed in this review, suggesting the cause of AHP from different perspectives. -

Depression, Apathy and Impaired Self-Awareness Following Severe Traumatic Brain Injury: a Preliminary Investigation
Brain Injury ISSN: 0269-9052 (Print) 1362-301X (Online) Journal homepage: https://www.tandfonline.com/loi/ibij20 Depression, apathy and impaired self-awareness following severe traumatic brain injury: a preliminary investigation U. Bivona, A. Costa, M. Contrada, D. Silvestro, E. Azicnuda, M. Aloisi, G. Catania, P. Ciurli, C. Guariglia, C. Caltagirone, R. Formisanohttps:// orcid.org/0000-0002-2516-0540 & G.P. Prigatano To cite this article: U. Bivona, A. Costa, M. Contrada, D. Silvestro, E. Azicnuda, M. Aloisi, G. Catania, P. Ciurli, C. Guariglia, C. Caltagirone, R. Formisanohttps://orcid.org/0000-0002-2516-0540 & G.P. Prigatano (2019) Depression, apathy and impaired self-awareness following severe traumatic brain injury: a preliminary investigation, Brain Injury, 33:9, 1245-1256, DOI: 10.1080/02699052.2019.1641225 To link to this article: https://doi.org/10.1080/02699052.2019.1641225 Published online: 14 Jul 2019. Submit your article to this journal Article views: 319 View related articles View Crossmark data Citing articles: 5 View citing articles Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=ibij20 BRAIN INJURY 2019, VOL. 33, NO. 9, 1245–1256 https://doi.org/10.1080/02699052.2019.1641225 Depression, apathy and impaired self-awareness following severe traumatic brain injury: a preliminary investigation U. Bivona a, A. Costa b, M. Contrada a, D. Silvestroa, E. Azicnudaa, M. Aloisia, G. Cataniaa, P. Ciurli a, C. Guariglia a,c, C. Caltagirone a,d, R. Formisanoa, and G.P. Prigatanoe aIRCCS, Santa Lucia Foundation, Rome, Italy; bUnicusano University, Rome, Italy; cSapienza University, Rome, Italy; dTor Vergata University, Rome, Italy; eDepartment of Clinical Neuropsychology, Barrow Neurological Institute, St.