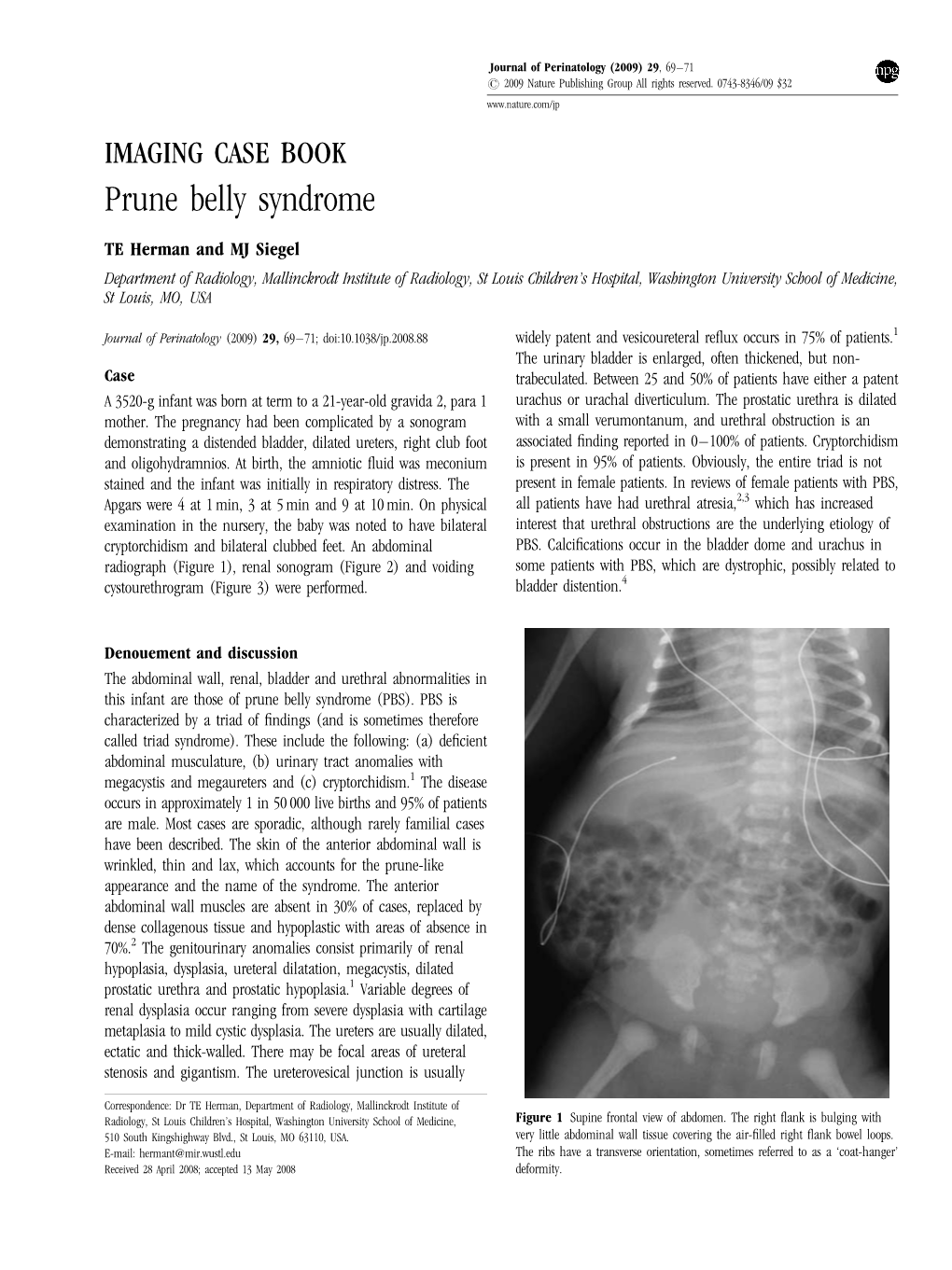
Prune Belly Syndrome
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Eagle-Barrett Syndrome Katherine Munier, MS, NNP-BC
Eagle-Barrett Syndrome Katherine Munier, MS, NNP-BC Children’s Hospital Colorado, Anschutz Medical Campus, CO An Overview Fluid & Electrolyte Balance A Case Study Pathogenicity Eagle-Barret Syndrome (Prune-Belly Syndrome) is Kidney Function The kidneys maintain fluid A 2.925kg male born at 35 weeks completed a rare congenital anomaly, thought to be caused by balance in the body. The renal medulla is integral gestational age (GA) via induced vaginal delivery. urethral outlet obstruction in early development. It to the urine concentration process. In response to This pregnancy was complicated by fetal bladder consists of a characteristic clinical triad: abdominal dehydration, the kidneys concentrate urine. In the outlet obstruction, and oligohydramnios. History is wall musculature deficiency, urinary tract presence of fluid overload, urine is diluted.1 significant for methamphetamine use, production, abnormalities, and cryptorchidism. Not all cases and distribution. Mother states she has been sober present with all three findings; additionally, the Sodium (Na+) Reference Range 134-144 mmol/L for over 8 months. Maternal urine toxicology and severity may vary.3 Serum [Na+] reflects total body water and Na+ meconium toxicology negative. balance In addition, congenital cardiac, pulmonary, At birth: the infant presented with Apgar scores of gastrointestinal, and orthopedic malformations can 8/9. At 6 minutes of life his heart rate was greater Potassium (K+) 4.1-5.3 mmol/L be appreciated in many Eagle-Barrett syndrome than 100; however, central cyanosis, gasps, and Serum [K+] is a function of internal (distribution of cases—some of which may have precipitated from retractions were present. He received continuous 3 K+ across cell membranes) and external (body) K+ an oligohydramnios sequence. -

Prune Belly Syndrome with Pouch Colon with Scaphoid Megalourethra: a Newer Embryological and Prognostic Perspective
42 Case report Prune belly syndrome with pouch colon with scaphoid megalourethra: a newer embryological and prognostic perspective Saurabh Garge, Monika Bawa and Katragadda Lakshmi Narasimha Rao We here report a rare association of megalourethra with Department of Pediatric Surgery, Advanced Pediatric Center, PGIMER, Chandigarh, India pouch colon with prune belly syndrome. We also provide a newer embryological and prognostic perspective to this Correspondence to Saurabh Garge, MCh, Department of Pediatric Surgery, Advanced Pediatric Center, PGIMER, Chandigarh 160012, India association. Ann Pediatr Surg 11:42–45 c 2015 Annals of Tel: + 91 172 274 7585 x5320; fax: + 91 172 274 4401/274 5078; Pediatric Surgery. e-mail: [email protected] Annals of Pediatric Surgery 2015, 11:42–45 Received 15 November 2012 accepted 26 May 2014 Keywords: megalourethra, prune belly syndrome pouch colon, scaphoid Introduction pressing the urethra, patient voided turbid purulent Prune belly syndrome (PBS), also known as Eagle–Barrett urine. The scrotum lacked rugosities and bilateral testis syndrome, comprises a triad of anomalies that include were undescended. They were not palpable even in the abdominal wall flaccidity, urologic abnormalities, and inguinal region (Fig. 1). The anal opening was absent, bilateral cryptorchidism. The incidence of PBS is with poorly developed buttocks and median raphe. A between 1 in 29 000 and 1 in 40 000 live male births, cross-table prone lateral radiograph and erect anteropos- with incidence four times higher in twins [1–6]. Male terior abdominal radiograph were suggestive of a high individuals are affected 20 times more often than female rectal anomaly with a pouch colon (Fig. -

Redalyc.Prune-Belly Syndrome: an Autopsy Case Report
Autopsy and Case Reports E-ISSN: 2236-1960 [email protected] Hospital Universitário da Universidade de São Paulo Brasil Pereira Silva Vasconcelos, Marcela Arruda; Picciarelli de Lima, Patricia Prune-belly syndrome: an autopsy case report Autopsy and Case Reports, vol. 4, núm. 4, octubre-diciembre, 2014, pp. 35-41 Hospital Universitário da Universidade de São Paulo São Paulo, Brasil Available in: http://www.redalyc.org/articulo.oa?id=576060827006 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Article / Autopsy Case Report Artigo / Relato de Caso de Autópsia Prune-belly syndrome: an autopsy case report Marcela Arruda Pereira Silva Vasconcelosa, Patricia Picciarelli de Limaa Vasconcelos MAPS, Lima PP. Prune-belly syndrome: an autopsy case report. Autopsy Case Rep [Internet]. 2014;4(4):35-41. http://dx.doi.org/10.4322/acr.2014.037 ABSTRACT Prune-belly syndrome (PBS) is a rare congenital anomaly characterized by a spectrum of mild-to-severe presentations of urinary tract malformations, deficient abdominal wall musculature, and cryptorchidism in male newborns or genital abnormalities in the female newborns. Currently, antenatal diagnosis is feasible with ultrasound examination, and treatment is based on case report experience. More recently, intrauterine management has been undertaken with encouraging results. The authors report a case of PBS diagnosed at the seventeenth gestation week, when ultrasonographic examination revealed the presence of ascites, distended bladder, thickened bladder wall and posterior urethral valve. -

Prune Belly Syndrome in Surviving Males Can Be Caused by Hemizygous Missense Mutations in the X-Linked Filamin a Gene Nida S
Iqbal et al. BMC Medical Genetics (2020) 21:38 https://doi.org/10.1186/s12881-020-0973-x RESEARCH ARTICLE Open Access Prune belly syndrome in surviving males can be caused by Hemizygous missense mutations in the X-linked Filamin A gene Nida S. Iqbal1* , Thomas A. Jascur1, Steven M. Harrison1,2, Angelena B. Edwards1, Luke T. Smith1, Erin S. Choi1, Michelle K. Arevalo1, Catherine Chen1, Shaohua Zhang1, Adam J. Kern1, Angela E. Scheuerle3,4, Emma J. Sanchez1,5, Chao Xing4 and Linda A. Baker1,5* Abstract Background: Prune belly syndrome (PBS) is a rare, multi-system congenital myopathy primarily affecting males that is poorly described genetically. Phenotypically, its morbidity spans from mild to lethal, however, all isolated PBS cases manifest three cardinal pathological features: 1) wrinkled flaccid ventral abdominal wall with skeletal muscle deficiency, 2) urinary tract dilation with poorly contractile smooth muscle, and 3) intra-abdominal undescended testes. Despite evidence for a genetic basis, previously reported PBS autosomal candidate genes only account for one consanguineous family and single cases. Methods: We performed whole exome sequencing (WES) of two maternal adult half-brothers with syndromic PBS (PBS + Otopalatodigital spectrum disorder [OPDSD]) and two unrelated sporadic individuals with isolated PBS and further functionally validated the identified mutations. Results: We identified three unreported hemizygous missense point mutations in the X-chromosome gene Filamin A (FLNA) (c.4952 C > T (p.A1448V), c.6727C > T (p.C2160R), c.5966 G > A (p.G2236E)) in two related cases and two unrelated sporadic individuals. Two of the three PBS mutations map to the highly regulatory, stretch-sensing Ig19– 21 region of FLNA and enhance binding to intracellular tails of the transmembrane receptor β-integrin 1 (ITGβ1). -

A Case Study of Prune Belly Syndrome with Congenital Vesico-Subumbilical Skin Fistula Allam Fayez Abuhamda1* and Mazen El-Sakka 2
Case Report iMedPub Journals Annals of Clinical and Laboratory Research 2018 www.imedpub.com Vol.6 No.3:254 ISSN 2386-5180 DOI: 10.21767/2386-5180.100254 A Case Study of Prune Belly Syndrome with Congenital Vesico-Subumbilical Skin Fistula Allam Fayez Abuhamda1* and Mazen El-Sakka 2 1Shifa Women`S Hospital, Shifa Nicu, Ministry of Health, Gaza, Palestine. 2Faculty of Pharmacy, Al Azhar University, Gaza, Palestine. *Corresponding author: Allam Fayez Abuhamda, Consultant Neonatologist, Shifa Women`S Hospital, Shifa Nicu, Ministry of Health, Gaza, Palestine, Tel: +00972597502720; E-mail: [email protected] Received Date: July 29, 2018; Accepted Date: September 11, 2018; Published Date: September 13, 2018 Citation: Abuhamda AF, EL-Sakka M (2018) A Case Study of Prune Belly Syndrome with Congenital Vesico-Subumbilical Skin Fistula. Ann Clin Lab Res Vol.6 No.3: 254. The PBS characterized by the deficient development of abdominal muscles that causes the skin of the abdomen to Abstract wrinkle like a prune, bilateral cryptorchidism, abnormalities of the urinary tract such as bilateral gross hydronephrosis, Prune Belly Syndromes (PBS) usually fatal unless there is a megaureter, and megacystis. communication between the fetal bladder and the amniotic sac. We report a case of PBS with congenital This article presents a case of neonate seen in our vesico-subumbilical skin fistula in a Palestinian male institution Al Shifa Hospital-Gaza, State of Palestine, neonate. The patient had defect abdominal muscles, presenting of PBS with congenital vesico-subumbilical fistula. wrinkled abdominal skin, cryptorchidism, urethral atresia, vesico-subumbilical skin fistula and normal kidney Case Report function. Baby was discharged home in general condition with once daily prophylactic dose of oral amoxicillin. -

The Prune Belly Syndrome: Urological Aspects and Long-Term Outcomes of a Rare Disease
Pediatric Reports 2012; volume 4:e20 The Prune Belly syndrome: affecting almost exclusively males (>95%), and characterized by a triad of clinical features Correspondence: Apostolos P. Labanaris, Prostate urological aspects and including urinary tract anomalies, abdominal Center Northwest, Department of Urology and long-term outcomes wall deficiency and bilateral cryptorchidism. Pediatric Urology, St. Antonius Medical Center, of a rare disease Nowadays, not as many children with PBS are Moellenweg 22, 48599 Gronau, Germany. seen in clinical practice as in the past, mainly Tel. +49.2562.915.7114 - Fax: +49.2562.915.2105. E-mail: [email protected] Vahudin Zugor,1 Günter E. Schott,2 due to prenatal ultrasound and subsequent pregnancy termination of affected cases. Apostolos P. Labanaris1 Key words: Prune-Belly syndrome, diagnosis, The protruding hypoplastic abdominal wall therapeutic options, surgical treatment. 1Department of Urology and Pediatric looks like a dried prune, hence the name Urology-Prostate Center Northwest, 1-5 Prune-Belly. However, abortive forms are Received for publication: 30 May 2011. St. Antonius Medical Center, Gronau; often also presented in which hypoplasia of the Revision received: 17 November 2011. 2Deparment of Urology, University of abdominal wall is not particularly severe. Accepted for publication: 18 November 2011. Erlangen Medical Center, Erlangen, Malformations of the urinary tract are due to This work is licensed under a Creative Commons Germany dysplasia of the smooth muscles of the renal Attribution NonCommercial 3.0 License (CC BY- pelvis and of the ureters, as well as of the pro- NC 3.0). static part of the urethra. Depending on type and severity, the syndrome presents with three ©Copyright V. -

Prune Belly Syndrome: a Case of Early Prenatal Diagnosis
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Kamra S et al. Int J Reprod Contracept Obstet Gynecol. 2017 Apr;6(4):1652-1655 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20171447 Case Report Prune belly syndrome: a case of early prenatal diagnosis Suvidhi Kamra1, Unmesh Santpur1*, Nidhi Puri2, Neetu Pippet2 1Department of Obstetrics and Gynecology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India 2 Department of Anatomy, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India Received: 18 January 2017 Accepted: 27 February 2017 *Correspondence: Dr. Unmesh Santpur, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Prune belly syndrome is a rare congenital disorder typically characterized by a triad of malformation of the urogenital tract, defect of abdominal wall musculature, and cryptorchidism. The condition is generally incompatible with life as infants born with this syndrome are either stillborn or die within the first few weeks of life. The present case is of a fetus presenting with prune bell syndrome, detected in first trimester of pregnancy. Keywords: Abdominal wall musculature, Abortus, Cryptoorchidism, Megalourethra, Prune belly syndrome, Ultrasound INTRODUCTION the diagnostic feature. However, renal function is the most important factor that determines the survival. The Frequent use of antenatal ultrasound has enabled us to other associated anomalies are pulmonary hypoplasia, detect various fetal anomalies at earlier gestations, thus club foot, potter’s facies and hip dislocation. -

Congenital Megalourethra in Prune Belly Syndrome
Open Access Archives of Case Reports Case Report A rare case: Congenital Megalourethra in prune belly ISSN 2637-3793 syndrome Ismail Selvi1, Numan Baydilli2* and Emre Can Akınsal2 1Department of Urology, Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital, Ankara, Turkey 2Department of Urology, Erciyes University, Kayseri, Turkey *Address for Correspondence: Numan Baydilli, Abstract MD, Erciyes University, Faculty of Medicine, Department of Urology, Köşk Mahallesi, Prof. Dr. Introduction: Prune Belly syndrome is a disease characterized by abdominal muscle defect, bilateral Turhan Feyzioğlu Cad. No:42, 38039 Melikgazi, cryptorchidsim and urinary system anomalies (refl ux megaureter, hydronephrosis, etc.). Pulmonary, cardiac, and Kayseri, Turkey, Tel: +903522076666-21134; gastrointestinal anomalies may also be present. Management of these rare cases is very important. In this case, Email: [email protected] the clinical course of a patient with Prune Belly syndrome with megaurethra is presented. Submitted: 16 January 2018 Case: The patient from the fi rst gestation and parturition with birth weight of 2500 g and 38 weeks was Approved: 29 January 2018 hospitalized because of the bilateral hydronephrosis. His physical examination revealed undescended testicles Published: 30 January 2018 and a large penis. The abdominal muscles were not very atrophic. The size of the kidney was small, bilateral Copyright: 2018 Selvi I, et al. This is an open hydroureteronephrosis and wide posterior urethra on the ultrasound. Renal function tests were progressively access article distributed under the Creative disturbed and the patient underwent cystourethroscopy for diagnostic purposes in terms of posterior urethral Commons Attribution License, which permits valve. A large diverticulum was found in anterior urethra. -

Article 6.Pmd
DSJUOG 10.5005/jp-journals-10009-1175 REVIEW ARTICLE Screening of Fetal Thorax and Abdomen Screening of Fetal Thorax and Abdomen Kazuo Maeda Professor (Emeritus), Department of Obstetrics and Gynecology, Tottori University Medical School, Yonago, Japan Correspondence: Kazuo Maeda, 3-125, Nadamachi, Yonago, Tottoriken 683-0835, Japan, Phone and Fax: 81-859-22-6856 e-mail: [email protected] ABSTRACT Ultrasonic screening was studied in the congenital and acquired disorders of fetal thorax cavity, diaphragm, lung and heart; those of fetal peritoneal cavity, liver, alimentary tract, abdominal wall; those of fetal kidneys, ureter and urinary bladder; and those of fetal genital organs. Keywords: Ultrasound, Screening, Fetus, Thorax, Abdomen, Hydrothorax, Lung, Diaphragm, CHD, Arrhythmia, Intestine, Liver, Kidney, Ureter, Bladder, Genitalia. FETAL THORAX Fetal thorax abnormalities are diagnosed by 2D, 3D, 4D ultrasound imaging, color Doppler flow mapping and pulsed Doppler flow velocity waveform. Abnormal number of fetal ribs with associated anomalies were reported.1,2 Deformity of Fetal Thorax Chondroectodermal dysplasia, thanatophoric dwarfism, various chondrodystrophy or dwarfism develop fetal thorax deformity, including bell-shape thorax with hypoplastic lung. Hypoplastic Fetal Lung Fetal lung volume is determined by using volume measuring 3,4 function of 3D ultrasound. Fig. 1: Pleural effusion and ascites at 19 weeks of gestation. Tomographic ultrasound imaging of fetal thorax and abdomen. Lung Immature Fetal Lung and liver float due to pleural effusion and ascites in the thoracic and abdominal spaces respectively. This was 45X/46XY mosaicism case Fetal lung immaturity diagnosis is significant in preterm labor and both pleural effusion and ascites repeatedly appeared and resolved to predict neonatal respiratory distress syndrome. -

Challenging Diagnosis of Prune Belly Syndrome Antenatally: a Case Report Waleed H
Alkhamis et al. Journal of Medical Case Reports (2019) 13:198 https://doi.org/10.1186/s13256-019-2120-x CASE REPORT Open Access Challenging diagnosis of prune belly syndrome antenatally: a case report Waleed H. Alkhamis , Sahar Hassan Abdulghani* and Amer Altaki Abstract Background: Prune belly syndrome is a rare congenital condition of uncertain etiology. It is characterized with a triad of abdominal distension due to deficient abdominal wall, genitourinary tract anomalies, and musculoskeletal anomalies. This condition varies in its severity which makes diagnosis challenging during early antenatal scanning. Case presentation: We reported a severe phenotype of prune belly syndrome which was not fully suspected in a 29- year-old Saudi woman was G4T2P0A1L2 at 21 weeks of gestation at the time of early antenatal presentation; however, it became apparent during diagnosis at a subsequent follow-up scan during advanced gestational age. Conclusion: Weconcludethatsuspicionofsuchanomaliesthroughanearlyantenatalscanrequireanurgentfurther follow-up scan in a tertiary center. The referral to the tertiary center must be to an experienced ultrasonographer and maternal–fetal medicine specialist for a decision to be made antenatally regarding the course of pregnancy and post- delivery management based on the severity of the condition. Keywords: Abdominal distention, Clubfeet, Urinary bladder enlargement, Prune belly syndrome Background Case presentation Prune belly syndrome (PBS) is known as Eagle–Barrett The authors report a case of a 29-year-old Saudi woman Syndrome or Obrinsky syndrome and is characterized by who was G4T2P0A1L2 at 21 weeks of gestation. She was a lack of development of abdominal wall muscles giving free from medical illness and she had had no previous the appearance of thin wrinkled skin which appears surgical procedures. -

Prune Belly Syndrome: Early Management Outcome of Nine Consecutive Cases
Original Article Prune belly syndrome: Early management outcome of nine consecutive cases OH Ekwunife, JO Ugwu, V Modekwe Department of Surgery, Paediatric Surgery Unit, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria Abstract Background: Prune belly syndrome (PBS) is a rare congenital malformation of unclear etiology. The disease progress and outcome in developing countries are not clear as most reports are isolated case reports. Materials and Methods: A review of 9 patients managed for PBS in 5 years. Results: There were 7 males and 2 females, aged 30 min‑11 days (median = 5 days) at the time of presentation (a child presented as neonate, defaulted from follow‑up and represented at 10 years of life). Their weights on admission were 2.5‑4.2 kg (median = 3 kg). Maternal age range was 26‑37 years (median = 32 years), with five mothers being above 30 years. Seven mothers had febrile illness in the first trimester and took antimalarial drugs or antibiotics. Intestinal malrotation was the most common associated anomaly. The degree of the anterior abdominal wall and the urinary tract morphology varies from patient to patient. Urinary tract anomalies were initially managed conservatively. Two infants however later had cutaneous ureterostomy due to worsening renal function and recalcitrant urinary tract infection (UTI). Four infants had abdominoplasty at the 2nd week, 6th week, 3rd year and 10th year of life. Seven orchiopexies were done. Four were done by Fowler‑Stephen’s method while the rest were via the inguinal route. Of the former, 3 testicles have normal volume 6 months after, whereas one atrophied. -

Prune Belly Syndrome with Bilateral Hydronephrosis - a Case Report
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Prune Belly Syndrome with Bilateral Hydronephrosis - A Case Report Kumar G V1, Shivaleela C2, Viswanathakumar H M3, Suresh B S4 1Assistant Professor in Pediatrics, 2Assistant Professor in Anatomy, 3Professor & HOD of Pediatrics, 4Associate Professor of Anatomy; Sri Siddhartha Medical College, Tumkur, Karnataka, India. Corresponding Author: Kumar G V Received: 02/03//2014 Revised: 29/03/2014 Accepted: 02/04/2014 ABSTRACT Prune belly syndrome is a rare congenital anomaly of uncertain etiology almost exclusive to males. It is characterized by the triad of absent or incomplete abdominal musculature, undescended testes, and urinary tract abnormalities. A male baby with above characteristic triad was brought to our hospital. A diagnosis of prune-belly syndrome was made. Here we report a case of prune-belly syndrome, in order to highlight the occurrence of this rare syndrome in our environment and to review its pathogenesis, presentation and management. Key words: Prune-belly syndrome, hydronephrosis. INTRODUCTION The case is reported for its rare congenital Prune belly syndrome was described abnormality. for the first time in the 1800s.[1] It is a rare condition defined by the triad of abdominal CASE REPORT muscle deficiency, severe urinary tract A 3.0kg male baby was brought to abnormality and cryptorchidism.[2-4] Other our hospital by an un-booked 23-year old names for Prune Belly Syndrome are Eagle- Gravida 1, Para 1, mother with history of Barret syndrome, Triad syndrome, Osler- abdominal distension since birth, fever and Parker Syndrome. It is caused by urethral lethargy since 2days and not taking feeds obstruction early in development resulting in since one day.