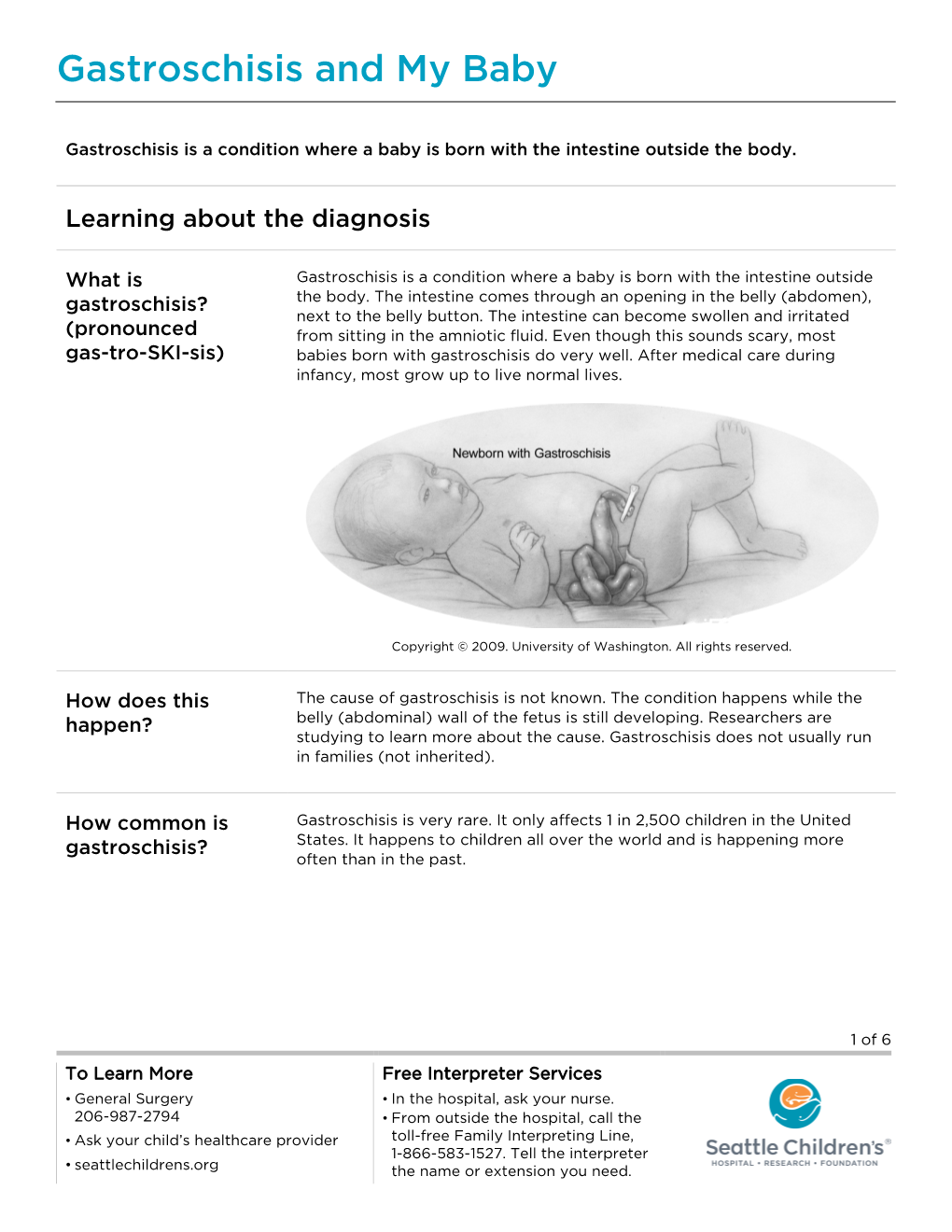
PE731 Gastroschisis and My Baby
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Abdominal Wall Defect
Abdominal wall defect Description An abdominal wall defect is an opening in the abdomen through which various abdominal organs can protrude. This opening varies in size and can usually be diagnosed early in fetal development, typically between the tenth and fourteenth weeks of pregnancy. There are two main types of abdominal wall defects: omphalocele and gastroschisis. Omphalocele is an opening in the center of the abdominal wall where the umbilical cord meets the abdomen. Organs (typically the intestines, stomach, and liver) protrude through the opening into the umbilical cord and are covered by the same protective membrane that covers the umbilical cord. Gastroschisis is a defect in the abdominal wall, usually to the right of the umbilical cord, through which the large and small intestines protrude (although other organs may sometimes bulge out). There is no membrane covering the exposed organs in gastroschisis. Fetuses with omphalocele may grow slowly before birth (intrauterine growth retardation) and they may be born prematurely. Individuals with omphalocele frequently have multiple birth defects, such as a congenital heart defect. Additionally, underdevelopment of the lungs is often associated with omphalocele because the abdominal organs normally provide a framework for chest wall growth. When those organs are misplaced, the chest wall does not form properly, providing a smaller than normal space for the lungs to develop. As a result, many infants with omphalocele have respiratory insufficiency and may need to be supported with a machine to help them breathe ( mechanical ventilation). Rarely, affected individuals who have breathing problems in infancy experience recurrent lung infections or asthma later in life. -

Hospital Readmission Among Infants with Gastroschisis
Journal of Perinatology (2011) 31, 546–550 r 2011 Nature America, Inc. All rights reserved. 0743-8346/11 www.nature.com/jp ORIGINAL ARTICLE Hospital readmission among infants with gastroschisis AP South1,2, JJ Wessel1,2, A Sberna1, M Patel1 and AL Morrow1 1Division of Neonatology, Perinatal Institute, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA and 2Intestinal Rehabilitation Program, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, USA Introduction Objective: Infants with gastroschisis have significant perinatal morbidity Gastroschisis is a congenital abdominal wall defect that results in including long hospitalizations and feeding intolerance. Two thirds are evisceration of the bowel into the amniotic space. The birth premature and 20% are growth restricted. Despite these known risk factors prevalence is increasing, affecting B4.5 per 10 000 births.1 While for post-natal complications, little is known about readmission for infants in-hospital morbidity and mortality are well described, there is with gastroschisis. Our objective was to determine the frequency and limited information regarding post-discharge outcomes. Infants indication for hospital readmission after initial discharge among infants with gastroschisis have multiple risk factors for poor long-term with gastroschisis. outcome, including prematurity in two thirds,2 and poor in utero Study Design: Retrospective cohort study. All surviving infants treated growth in 20%.3 Despite absence of extreme prematurity in most for gastroschisis at Cincinnati Children’s Hospital Medical Center, born cases, all infants with gastroschisis are at risk for the development between January 2006 and December 2008 were included. Main outcome of necrotizing enterocolitis with subsequent bowel injury or loss. -

11 Visceral and Parietal Anomalies
6505 BIOL 5720 − INTRODUCTION TO FETAL MEDICINE 11. VISCERAL AND PARIETAL ANOMALIES Arlet G. Kurkchubasche, M.D. Francois I. Luks, M.D. ABDOMINAL WALL DEFECTS Definitions - Omphalocele (also called exomphalos) § Defect is central, involving the umbilicus § Often covered by a membrane, “protecting” viscera; membrane may be ruptured § >30 % have associated anomalies - Chromosomal anomalies: trisomy 18 - “Upper midline” defects: Pentalogy of Cantrell (including heart, pericardium, pleural) - “Lower midline” defects: cloacal exstrophy § Etiology: depends on type; unclear - Gastroschisis (laparoschisis) § Defect is always too the side of an intact umbilicus; usually right of midline § Never covered by a membrane § Associated anomalies are rare, except (presumably secondary) intestinal ones (atresia) § Correlation with young maternal age § 4-5 times more common than omphalocele Diagnosis - Ultrasound very sensitive, and highly specific: § Position of defect and umbilical cord insertion (omphalocele vs. gastroschisis) § Difficult < 16 weeks; not possible < 12 weeks (‘physiologic’ omphalocele at 8-11 wk) § Importance of finding associated anomalies: - Chromosomal (amniocentesis) (omphalocele) - Heart, bladder, pelvis (exstrophy), limbs: omphalocele - Major limb/body wall deformities: rare form of severe amniotic band syndrome sometimes associated with gastroschisis – highly lethal 1 BIOL 6505 § Gastrointestinal anomalies: intestinal loop distension not specific/sensitive for atresia § Grading: “giant” omphalocele contains liver; small omphalocele = “hernia of the cord” - Alpha-fetoprotein (AFP) elevated (amniotic fluid and maternal serum): reflects ‘leakage’ of body proteins through any breach in fetal skin: gastroschisis, spina bifida Prenatal management - Alterations in time, place and mode of delivery § Decision to deliver in tertiary center (with neonatal ICU and surgical services) § C/Section:usually not necessary, except for giant omphalocele (liver trauma) § Early delivery: - Controversial. -

Gastroschisis and Omphalocele
Gastroschisis and Omphalocele The two most common congenital abdominal wall At delivery, the ABC (airway, breathing, circulation) rule defects are gastroschisis and omphalocele. Both involve should be followed for babies with gastroschisis or incomplete closure of the abdominal wall during fetal omphalocele. Immediately afterward, protection of the development, and for both, their cause is unknown. A herniated contents and management of evaporative loss gastroschisis is usually an isolated congenital defect, should be accomplished. Abdominal contents should be whereas a baby with an omphalocele often has chromo- wrapped in warm, saline-soaked gauze and covered with some anomalies, cardiac conditions, and other major birth plastic wrap. Alternatively, the baby should be placed in defects. a sterile bowel bag up to the nipple line. Preventing evap- orative fluid loss is particularly important for the baby A gastroschisis is a herniation of abdominal contents with gastroschisis because of the lack of the protective through a defect in the abdominal wall, usually just to the membranous covering of the abdominal contents. Dili- right of the umbilicus. An omphalocele is a herniation of gent observation of the color and perfusion of the abdom- abdominal contents into the umbilical cord itself. The con- inal contents of a baby with gastroschisis is imperative. tents of a gastroschisis are directly exposed to amniotic The baby should be placed on his or her right side with fluid, whereas the contents of an omphalocele are usually abdominal contents supported with additional gauze or covered with a protective membranous sac. blankets to prevent kinking of the mesentery blood ves- sels. An echocardiogram also should be considered to rule out potential cardiac anomalies (Escobar & Caty, 2016). -

Abdominal Wall Defects—Current Treatments
children Review Abdominal Wall Defects—Current Treatments Isabella N. Bielicki 1, Stig Somme 2, Giovanni Frongia 3, Stefan G. Holland-Cunz 1 and Raphael N. Vuille-dit-Bille 1,* 1 Department of Pediatric Surgery, University Children’s Hospital of Basel (UKBB), 4056 Basel, Switzerland; [email protected] (I.N.B.); [email protected] (S.G.H.-C.) 2 Department of Pediatric Surgery, University Children’s Hospital of Colorado, Aurora, CO 80045, USA; [email protected] 3 Section of Pediatric Surgery, Department of General, Visceral and Transplantation Surgery, 69120 Heidelberg, Germany; [email protected] * Correspondence: [email protected]; Tel.: +41-61-704-27-98 Abstract: Gastroschisis and omphalocele reflect the two most common abdominal wall defects in newborns. First postnatal care consists of defect coverage, avoidance of fluid and heat loss, fluid administration and gastric decompression. Definitive treatment is achieved by defect reduction and abdominal wall closure. Different techniques and timings are used depending on type and size of defect, the abdominal domain and comorbidities of the child. The present review aims to provide an overview of current treatments. Keywords: abdominal wall defect; gastroschisis; omphalocele; treatment 1. Gastroschisis Citation: Bielicki, I.N.; Somme, S.; 1.1. Introduction Frongia, G.; Holland-Cunz, S.G.; Gastroschisis is one of the most common congenital abdominal wall defects in new- Vuille-dit-Bille, R.N. Abdominal Wall borns. Children born with gastroschisis have a full-thickness paraumbilical abdominal Defects—Current Treatments. wall defect, which is associated with evisceration of bowel and sometimes other organs Children 2021, 8, 170. -

Human Milk Versus Formula After Gastroschisis Repair: Effects on Time to Full Feeds and Time to Discharge
Journal of Perinatology (2013) 33, 627–630 & 2013 Nature America, Inc. All rights reserved 0743-8346/13 www.nature.com/jp ORIGINAL ARTICLE Human milk versus formula after gastroschisis repair: effects on time to full feeds and time to discharge JA Kohler Sr, AM Perkins and WT Bass OBJECTIVE: To determine if the choice of enteral feeds after gastroschisis repair relates to the time to achieve full feeds and time to discharge. STUDY DESIGN: A retrospective study of infants with gastroschisis from 2000 to 2010 examined demographics, days at closure, days at initiation of feeds, days to full feeds, time to discharge and length of stay. RESULT: Ninety infants were identified, 22 received (human milk) HM exclusively, 15 were fed 450% HM, 16 were fed o50% HM and 26 were fed only cow milk-based formulas. Infants fed exclusively HM had significantly shorter times to full enteral feedings (median 5 days versus 7 days, P ¼ 0.03). The time from initiation of feedings to hospital discharge, which accounts for initiation age, significantly favored the exclusively HM-fed infants (median 7 days versus 10 days, P ¼ 0.01). CONCLUSION: Exclusive HM feeding after gastroschisis repair decreases time to achieve full enteral feeds and time to discharge. Journal of Perinatology (2013) 33, 627–630; doi:10.1038/jp.2013.27; published online 21 March 2013 Keywords: total parenteral nutrition; parenteral nutrition-associated liver disease; intestinal permeability INTRODUCTION METHODS Gastroschisis is a congenital defect of the ventral abdominal wall. Study population The lesion consists of a small full-thickness periumbilical cleft This retrospective study included all patients who were admitted to the usually to the right of the umbilicus, which allows for the neonatal intensive care unit of the Children’s Hospital of The King’s herniation of abdominal contents into the amniotic sac. -

Gastroschisis
Gastroschisis This guideline was updated in May 2015 by Dr Renuka Bhat with input from members of the New Zealand Maternal Fetal Medicine Network. Background Fetal gastroschisis is usually often diagnosed at Nuchal translucency or routine anomaly scan. Underlying cause is still unknown, but is believed to be related to vascular compromise of the omphalomesenteric artery during embryonic development. Numerous studies have reported a rising incidence of gastroschisis. Risk factors include young maternal age, smoking and use of vasoactive agents. A survival rate of liveborn infants with gastroschisis is 90 – 95%. The risk of intra-uterine fetal death is about 10% and its association with fetal distress is well known. Once the diagnosis is clarified (where possible) options can be discussed with the woman and her support. If the woman continues the pregnancy, continued care with fetal medicine input/ LMC is indicated. The follow-up will depend on the situation. 2015 May Gastroschisis: Objective To guide the accurate diagnosis, investigation and management of women presenting with fetal gastroschisis. To provide a consistent approach to the care of women with fetal gastroschisis which takes into consideration individual women’s views and wishes regarding care plan. 2 Definition • Fetal gastroschisis is defined as full thickness anterior abdominal wall defect with bowel protruding through the defect • It usually occurs on the right side of a normally inserting umbilical cord • The defect is not covered by membrane Differential Diagnosis • Omphalocele and associated syndromes (e.g. Beckwith-Wiedermann, pentalogy of Cantrell) • Amniotic banding • Limb- body wall complex Important History • Age and ethnicity Gastroschisis: May 2015 May Gastroschisis: • Any drug use particularly vaso-active drugs • Past obstetric history, any anomalies / syndromes • Any family history of note. -

Intestinal Malrotation: a Diagnosis to Consider in Acute Abdomen In
Submitted on: 05/20/2018 Approved on: 08/07/2018 CASE REPORT Intestinal malrotation: a diagnosis to consider in acute abdomen in newborns Antônio Augusto de Andrade Cunha Filho1, Paula Aragão Coimbra2, Adriana Cartafina Perez-Bóscollo3, Robson Azevedo Dutra4, Katariny Parreira de Oliveira Alves5 Keywords: Abstract Intestinal obstruction, Intestinal malrotation is an anomaly of the midgut, resulting from an embryonic defect during the phases of herniation, Acute abdomen, rotation, and fixation. The objective is to report a case of complex diagnostics and approach. The diagnosis was made Gastrointestinal tract. surgically in a patient presenting with hemodynamic instability, abdominal distension, signs of intestinal obstruction, and pneumoperitoneum on abdominal X-ray, with suspected grade III necrotizing enterocolitis. During surgery, a volvulus resulting from poor intestinal rotation was found at a distance of 12 cm from the ileocecal valve. Hemodynamic instability and abdominal distension recurred, and another exploratory laparotomy was required to correct new intestinal perforations. Therefore, early diagnosis with surgical correction before a volvulus appears is essential. Abdominal Doppler ultrasonography has been promising for early diagnosis. 1 Academic in Medicine - Federal University of the Triângulo Mineiro - Uberaba - Minas Gerais - Brazil 2 Resident in Pediatric Intensive Care - Federal University of the Triângulo Mineiro - Uberaba - Minas Gerais - Brazil 3 Associate Professor - Federal University of the Triângulo Mineiro - Uberaba - Minas Gerais - Brazil. 4 Adjunct Professor - Federal University of the Triângulo Mineiro - Uberaba - Minas Gerais - Brazil 5 Academic in Medicine - Federal University of the Triângulo Mineiro - Uberaba - Minas Gerais - Brazil Correspondence to: Antônio Augusto de Andrade Cunha Filho. Universidade Federal do Triângulo Mineiro, Acadêmico de Medicina - Uberaba - Minas Gerais - Brasil. -

CSW Gastroschisis Pathway Team for the November 18, 2015 Go Live
Gastroschisis v.2.0 Citation Information Summary of Version Changes Explanation of Evidence Ratings PHASE I (PRENATAL) Inclusion Criteria · All pregnancies complicated by fetal gastroschisis Exclusion Criteria · None Referrals Neonatology Maternal Fetal Medicine Pediatric Surgery Minimum Fetal Surveillance: Ultrasound performed every 3-4 weeks after diagnosis for the following Prenatal visit: (use prenatal ultrasound checklist): Gastroschisis slide show ! · Fetal growth Increase · Amniotic fluid volume surveillance · Gastroschisis defect · Bowel diameter (intra- and extra-abdominal) If other · Stomach dimension non-gastroschisis · Bowel wall thickness (intra- and extra-abdominal) obstetric, · Superior mesenteric artery and vein patency and velocity maternal or fetal · Gastric herniation (or other organ herniation) ! indications · Any other organ abnormalities Indicators for Delivery Starting at 32 weeks: Gastroschisis alone is · Non Stress test twice weekly not an indication for · Weekly ultrasound for AFI preterm delivery Anatomic abnormalities related to the gastroschisis are not an indication for preterm delivery Timing for Delivery: · Base the timing of delivery solely on maternal and obstetric indications · Deliver at 39 weeks in the absence of maternal, fetal or obstetric indications · Avoid preterm delivery in the absence of maternal, fetal or obstetric indications Phase Change Mode of Delivery: · Gastrochisis alone is not an indication for C-section · Deliver vaginally and reserve cesarean delivery for maternal, fetal or obstetric -

Gastroschisis Guidelines
Newborn Critical Care Center (NCCC) Clinical Guidelines Management of Gastroschisis OBJECTIVE To develop an evidence-based standard of care for the medical and surgical management of gastroschisis Exclusions: This guideline does not apply to patients with complex gastroschisis (including volvulus, atresia, necrotic bowel, or bowel perforation). PRE-OPERATIVE MANAGEMENT Delivery Room Avoid bag/mask ventilation when possible; determine the need for intubation and mechanical ventilation based on clinical status. Place warm, pre-soaked gauze roll over bowel during resuscitation if needed. Use latex‐free products. Examine the bowel to determine if there is any torsion, ischemia, atresia, perforation, or visceral organ involvement. Place patient in right side‐lying position to prevent kinking of the bowel. Reposition as appropriate to prevent torsion/kinking of bowel. Weigh infant prior to wrapping bowel. Wrap exposed bowel and viscera with gauze roll pre-soaked in warm saline. Place wrapped bowel and lower body up to the axillae into "bowel bag" and secure bag opening loosely across upper chest. Minimize handling of bowel and monitor color and perfusion of bowel continuously. Insert 10Fr Replogle (sump tube) to low, continuous suction for decompression. Ask for check type and screen to be sent on cord blood. Upon Admission Use the Neonatal Abdominal Wall Defect Admission Order Set. Closely monitor blood pressure, perfusion (peripheral and bowel), and temperature (avoid hypothermia). Maintain NPO status with Replogle to low, continuous suction. Notify Pediatric Surgery for evaluation and closure planning. Keep gauze dressing moist and bowel bag in place until surgical intervention. Place peripheral IV for parenteral fluids and antibiotics. There is no contraindication to using an umbilical venous catheter (UVC) if needed. -

Gastroschisis: a State-Of-The-Art Review
children Review Gastroschisis: A State-of-the-Art Review Vishwanath Bhat 1, Matthew Moront 2 and Vineet Bhandari 1,* 1 Division of Neonatology, Department of Pediatrics, The Children’s Regional Hospital at Cooper, Cooper Medical School of Rowan University, One Cooper Plaza, Camden, NJ 08103, USA; [email protected] 2 Division of Pediatric Surgery, Department of Pediatrics, The Children’s Regional Hospital at Cooper, Cooper Medical School of Rowan University, One Cooper Plaza, Camden, NJ 08103, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-856-342-6156 or +1-856-342-2000 (ext. 1089752); Fax: +1-856-342-8007 Received: 9 November 2020; Accepted: 14 December 2020; Published: 17 December 2020 Abstract: Gastroschisis, the most common type of abdominal wall defect, has seen a steady increase in its prevalence over the past several decades. It is identified, both prenatally and postnatally, by the location of the defect, most often to the right of a normally-inserted umbilical cord. It disproportionately affects young mothers, and appears to be associated with environmental factors. However, the contribution of genetic factors to the overall risk remains unknown. While approximately 10% of infants with gastroschisis have intestinal atresia, extraintestinal anomalies are rare. Prenatal ultrasound scans are useful for early diagnosis and identification of features that predict a high likelihood of associated bowel atresia. The timing and mode of delivery for mothers with fetuses with gastroschisis have been somewhat controversial, but there is no convincing evidence to support routine preterm delivery or elective cesarean section in the absence of obstetric indications. -

Gastroschisis Information for Parents/Carers What Is Gastroschisis? Gastroschisis Means “Stomach Cleft”
Oxford University Hospitals NHS Trust The Children’s Hospital Gastroschisis Information for parents/carers What is gastroschisis? Gastroschisis means “stomach cleft”. Usually, during early pregnancy, the baby’s intestine develops inside the umbilical cord and then moves inside their abdomen (tummy) after a few weeks. In gastroschisis, the abdominal wall does not fully develop. This means some of the baby’s intestine escapes through a hole in their abdominal wall. In babies with gastroschisis the part of the intestine which is outside their abdomen is exposed to amniotic fluid in the womb and then air when the baby is born. This can cause damage to the intestine. The exposed intestine may also become twisted as it floats in the amniotic fluid. This twisting can cut off the blood supply to the intestine, again causing damage. The damage that may be caused can include a dead portion of the intestine (where blood supply has been completely cut off), a hole in the intestine and a blockage in the intestine. Gastroschisis is a rare condition with only 4 to 5 babies out of every 10,000 being born with it. It is not known exactly what causes gastroschisis but it is more likely to happen if you have been ill or had an infection either before or during your pregnancy, or if you had or have a drug, cigarette or alcohol dependency. How is gastroschisis diagnosed? Gastroschisis is usually diagnosed during routine prenatal ultrasound scans. Part of the baby’s intestine will be able to be seen outside of their abdomen. If it is not identified before birth, gastroschisis will be seen immediately when your baby is born.