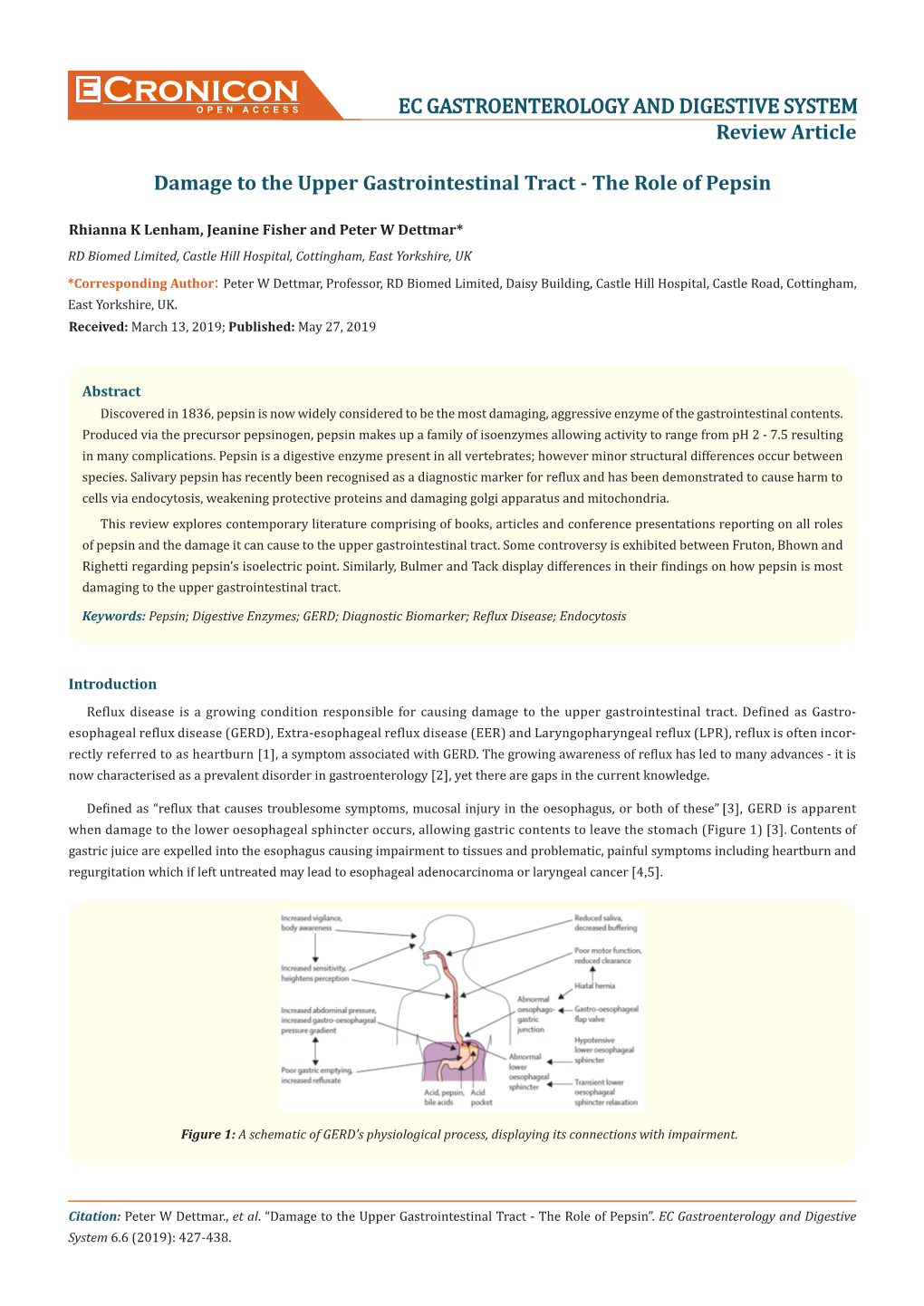
Cronicon OPEN ACCESS EC GASTROENTEROLOGY and DIGESTIVE SYSTEM Review Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Laryngopharyngeal Reflux (LPR) and Gastroesophageal Reflux (GERD)
Laryngopharyngeal Reflux (LPR) and Gastroesophageal Reflux (GERD) Laryngopharyngeal reflux (LPR) is an inflammatory condition defined as the backflow of gastric contents into the laryngopharynx, where it comes in contact with the tissues of the upper aerodigestive tract. LPR is characterized by chronic inflammation of the laryngopharynx and, more broadly, the tissues of the upper aerodigestive tract. The mechanism of LPR requires bypassing both the upper and lower esophageal sphincters to achieve extraesophageal reflux of gastric contents. This is in contrast to gastroesophageal reflux disease (GERD), which involves backflow of gastric contents into the esophagus bypassing only the lower esophageal sphincter. J.A. Koufman, J.E. Aviv, R.R. Casiano, et al. Laryngopharyngeal reflux: position statement of the committee on speech, voice, and swallowing disorders of the American Academy of Otolaryngology- Head and Neck Surgery Otolaryngol Head Neck Surg, 127 (2002), pp. 32-35. J.R. Lechien, C. Finck, P. Costa de Araujo, et al. Voice outcomes of laryngopharyngeal reflux treatment: a systematic review of 1483 patients. Eur Arch Otorhinolaryngol, 274 (2016), pp. 1-23. Anatomy and Physiology Over time, liquid or aerosolized gastric contents, including acid, bile, and pepsin inflame the tissue of the laryngopharynx, leading to symptoms including cough, throat clearing, mucus sensation, globus sensation, and hoarseness as well as laryngeal findings such as postcricoid edema, arytenoid mucosal erythema, pachydermia, and pseudosulcus. Ford CN. Evaluation and management of laryngopharyngeal reflux. JAMA 2005;294:1534–1540. Noordzij P, Khidr A, Evans B, et al. Omeprazole in treatment of reflux laryngitis. Laryngoscope 2001;111:2147–2151. Although gastroesophageal reflux GERD similarly involves the reflux of gastric contents, LPR, also referred to as extraesophageal or atypical reflux is a distinct diagnosis, is often present without the esophagitis, frank regurgitation or heartburn associated with GERD, and only 20% of LPR patients have frank GERD symptoms. -

Reflux Advice Sheet
Avoid tight clothing around your waist: It is best to take Gaviscon Advance as the Bending from the knees when lifting very last thing you take before going to and moving may also help. bed. It can also be of benefit after meals and before strenuous exercise. You should Some people find it helpful to keep a food not take it at the same time as taking your diary to identify any particular foods or PPI or other anti-acid medication, as it can eating habits which make their symptoms make them less effective. worse. For advice on any medications you have Are there any medicines I can been prescribed or purchased over the take to help? counter speak to your GP or pharmacist. Your consultant or GP may have prescribed a medicine known as a PPI or Proton Pump Inhibitor. Examples include Lanzoprazole and Omeprazole. These prevent the secretion of acid into the stomach. For the most effective treatment of LPR these should be taken half an hour before meals. For the medication to be effective, you should take it for a continuous period of time once or twice a day, as prescribed. If The Trust provides free symptoms do not improve go to your GP to monthly health talks on a Reflux Advice review the type and amount of medication. variety of medical conditions It may take a couple of attempts to find and treatments. For more information visit the combination that works best for you. www.uhb.nhs.uk/health-talks.htm or Sheet call 0121 371 4323. -

Gastroesophageal and Laryngopharyngeal Reflux Associated with Laryngeal Malignancy: a Systematic Review and Meta-Analysis
Accepted Manuscript Gastroesophageal and Laryngopharyngeal Reflux Associated with Laryngeal Malignancy: A Systematic Review and Meta-Analysis Sean M. Parsel, DO, Eric L. Wu, MD, Charles A. Riley, MD, Edward D. McCoul, MD, MPH PII: S1542-3565(18)31150-9 DOI: https://doi.org/10.1016/j.cgh.2018.10.028 Reference: YJCGH 56150 To appear in: Clinical Gastroenterology and Hepatology Accepted Date: 8 October 2018 Please cite this article as: Parsel SM, Wu EL, Riley CA, McCoul ED, Gastroesophageal and Laryngopharyngeal Reflux Associated with Laryngeal Malignancy: A Systematic Review and Meta-Analysis, Clinical Gastroenterology and Hepatology (2018), doi: https://doi.org/10.1016/ j.cgh.2018.10.028. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. ACCEPTED MANUSCRIPT Title : Gastroesophageal and Laryngopharyngeal Reflux Associated with Laryngeal Malignancy: A Systematic Review and Meta-Analysis Sean M. Parsel, DO 1, Eric L. Wu, MD 1, Charles A. Riley, MD 2, and Edward D. McCoul, MD, MPH 1, 3, 4 1 Tulane University School of Medicine, Department of Otolaryngology—Head and Neck Surgery, New Orleans, LA 2 Weill Cornell Medical Center, Department of Otolaryngology—Head and Neck Surgery, New York, NY 3 Ochsner Clinic Foundation, Department of Otorhinolaryngology, New Orleans, LA 4 University of Queensland School of Medicine, Ochsner Clinical School, New Orleans, LA Short title: Reflux and Laryngeal Malignancy Grant support: none Correspondence Edward D. -

Laryngopharyngeal Reflux
International Journal of Otolaryngology Laryngopharyngeal Reflux Guest Editors: Wolfgang Issing, Petros D. Karkos, Oliver Reichel, and Marcus Hess Laryngopharyngeal Reflux International Journal of Otolaryngology Laryngopharyngeal Reflux Guest Editors: Wolfgang Issing, Petros D. Karkos, Oliver Reichel, and Marcus Hess Copyright © 2012 Hindawi Publishing Corporation. All rights reserved. This is a special issue published in “International Journal of Otolaryngology.” All articles are open access articles distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Editorial Board Rolf-Dieter Battmer, Germany Ludger Klimek, Germany Leonard P. Rybak, USA Robert Cowan, Australia Luiz Paulo Kowalski, Brazil Shakeel Riaz Saeed, UK P. H. Dejonckere, The Netherlands Roland Laszig, Germany Michael D. Seidman, USA Joseph E. Dohar, USA Charles Monroe Myer, USA Mario A. Svirsky, USA Paul J. Donald, USA Jan I. Olofsson, Norway Ted Tew fik, Canada R. L. Doty, USA Robert H. Ossoff,USA Paul H. Van de Heyning, Belgium David W. Eisele, USA JeffreyP.Pearson,UK Blake S. Wilson, USA Alfio Ferlito, Italy Peter S. Roland, USA B. J. Yates, USA Contents Laryngopharyngeal Reflux, Petros D. Karkos, Wolfgang Issing, Oliver Reichel, and Marcus Hess Volume 2012, Article ID 926806, 2 pages Chronic Cough, Reflux, Postnasal Drip Syndrome, and the Otolaryngologist,DeborahC.Sylvester, Petros D. Karkos, Casey Vaughan, James Johnston, Raghav C. Dwivedi, Helen Atkinson, and Shah Kortequee Volume 2012, Article ID 564852, 5 pages Impact of Laparoscopic Fundoplication for the Treatment of Laryngopharyngeal Reflux: Review of the Literature, Guilherme da Silva Mazzini and Richard Ricachenevsky Gurski Volume 2012, Article ID 291472, 4 pages Eosinophilic Esophagitis for the Otolaryngologist, Petros D. -

Laryngopharyngeal Reflux Is Associated with Nasal Septal Deviation
Eur J Rhinol Allergy 2020; 3(1): 1-3 Original Article Laryngopharyngeal Reflux is Associated with Nasal Septal Deviation Eugene Wong , Nathaniel Deboever , Niranjan Sritharan , Narinder Singh Department of Otolaryngology Head and Neck Surgery, University of Sydney Westmead Hospital, Sydney, Australia Abstract Objective: Laryngopharyngeal reflux (LPR) is defined as a retrograde flow of gastric contents into the larynx and hy- popharynx. However, a possible pathophysiological contribution from nasal resistance has been proposed, according to which increased nasal resistance associated with septal deviation may cause increased respiratory effort, resulting in a more negative intrathoracic pressure, which may, in turn, overcome the upper esophageal sphincter and lead to the retrograde passage of gastric contents. The aim of this study was to investigate whether septal deviation of adequate severity necessitating septoplasty is associated with an increased use of proton pump inhibitors (PPIs) in comparison with the general population. Material and Methods: This retrospective single-center cohort study investigated the usage of PPIs in patients undergoing septoplasty. Hospital databases were searched to identify patients aged 18-85 years who underwent sep- toplasty from January 2012 to December 2016. Electronic medical records were reviewed to collect details pertaining to demographic variables, usage of PPIs, smoking and drinking status, and other comorbidities. A control group of subjects who underwent an unrelated procedure (arthroscopy) was also sampled. Results: The data of 200 patients (29% females, mean age 40.8±14.8 years) who underwent septoplasties were com- pared with those of 200 control subjects (39.5% females, mean age 45.3±15.0 years) who underwent arthroscopies. -

Pediatric Gastroesophageal Reflux Clinical Practice
SOCIETY PAPER Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition ÃRachel Rosen, yYvan Vandenplas, zMaartje Singendonk, §Michael Cabana, jjCarlo DiLorenzo, ôFrederic Gottrand, #Sandeep Gupta, ÃÃMiranda Langendam, yyAnnamaria Staiano, zzNikhil Thapar, §§Neelesh Tipnis, and zMerit Tabbers ABSTRACT This document serves as an update of the North American Society for Pediatric INTRODUCTION Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European n 2009, the joint committee of the North American Society for Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Pediatric Gastroenterology, Hepatology, and Nutrition (NASP- 2009 clinical guidelines for the diagnosis and management of gastroesophageal GHAN)I and the European Society for Pediatric Gastroenterology, refluxdisease(GERD)ininfantsandchildrenandisintendedtobeappliedin Hepatology, and Nutrition (ESPGHAN) published a medical posi- daily practice and as a basis for clinical trials. Eight clinical questions addressing tion paper on gastroesophageal reflux (GER) and GER disease diagnostic, therapeutic and prognostic topics were formulated. A systematic (GERD) in infants and children (search until 2008), using the 2001 literature search was performed from October 1, 2008 (if the question was NASPGHAN guidelines as an outline (1). Recommendations were addressed -

Diet and Lifestyle Changes for Reducing Reflux And
HERE PLACE PLACE STAMP STAMP Diet and lifestyle changes for reducing reflux and LPR LPRD • Cut out caffeine and alcohol, especially Laryngopharyngeal Reflux Disease in the late evening and before bedtime as Chronic cough these allow reflux to occur more easily. Frequent throat clearing •Avoid carbonated drinks or acidic foods like juice, especially before bedtime. Excessive mucous in the throat •Eliminate fatty, fried, or spicy foods Intermittent hoarseness especially at the last meal of the day. Post nasal drip sensation •Stop eating at least 3 hours before Sensation of lump in throat going to bed or laying down. •Evaluate if you might have sleep apnea. Symptoms include loud snoring, Northwestern Medicine non-restful sleep, daytime fatigue. Department of Otolaryngology •Elevate the head of your bed by 4-6 Head and Neck Surgery 675 N. St. Clair Street, inches. Galter, Suite 15-200 •Lose weight if you are overweight. Chicago, IL, 60611 Tel: 312-695-8182 •If you smoke tobacco, quit! Smoking Fax: 312-695-7851 www.ent.nm.org worsens reflux and makes your larynx more sensitive to damage. What is LPR? How do I know if I have LPR? How is LPR treated? Laryngopharyngeal reflux (LPR), also called laryngopharyngeal reflux disease (LPRD), If you experience symptoms such as throat There are two main ways to treat LPR: extraesophogeal reflux, reflux laryngitis, and clearing, chronic hoarseness, difficulty medications and changes to your behavior. posterior laryngitis, is a common diagnosis swallowing, a feeling of a lump in the throat In very rare cases, surgery may be hypothesized to be caused by the backflow of stomach contents into the throat and back of your or a cough, for several weeks you might have recommended to help prevent acid reflux. -

Laryngopharyngeal Reflux: Diagnosis, Treatment and Latest Research
Review Eur Surg DOI 10.1007/s10353-016-0385-5 Laryngopharyngeal reflux: diagnosis, treatment and latest research G. L. Falk1,2,3 · S. J. Vivian4 Received: 13 December 2015 / Accepted: 13 January 2016 © Springer-Verlag Wien 2016 Summary Aim Aim A review of the recent changes in understand- ing of laryngopharyngeal and extra-oesophageal reflux Review the recent changes in the evaluation of cause, symptoms. investigation and therapy in the evolving area of extra- Method Literature search over 7 years (2008–2015) oesophageal symptoms of reflux disease. and relevant historical cited articles. Results Modern investigation more clearly shows a subgroup of patients with intermittent full column Method oesophago-gastric-reflux-causing symptoms. Multiple other sites in the lung, head and neck may also be impli- Ongoing review of the literature has been pursued by the cated in the reflux disease process. senior author (GLF) of PubMed and the National Centre Conclusion Understanding of extra-oesophageal for Biotechnology Information (NCBI) at the National reflux symptomology is evolving. New equipment and Library of Medicine (NLM). Search was conducted techniques suggest further areas of research, and as yet monthly using (“laryngopharyngeal reflux”[MeSH] OR effective therapy remains elusive for some. LARYNGOPHARYNGEAL REFLUX[Title/Abstract]) OR ((COUGH[Title/Abstract] OR “cough”[MeSH]) AND Keywords Laryngopharyngeal reflux · (“gastroesophageal reflux”[MeSH] OR “GASTROESOPH- Gastro-oesophageal reflux · AGEAL REFLUX”[Title/Abstract] OR “GASTROOESOPH- Laparoscopic fundoplication AGEAL REFLUX”[Title/Abstract] OR “gastroesophageal reflux”[MeSH Terms] OR REFLUX[Title/Abstract])) for the years 2008–2015. Relevant articles were extracted pro- gressively and topics searched on PubMed as required from 2008 onward. -

Laryngopharyngeal Reflux Disease
Northwestern Memorial Hospital Patient Education CONDITIONS AND DISEASES Laryngopharyngeal Reflux Disease Laryngopharyngeal reflux (LPR), also called laryngopharyngeal reflux disease (LPRD), extraesophogeal reflux, reflux laryngitis, and posterior laryngitis, is a common diagnosis. It is thought to be caused by the backflow of stomach contents or nasal mucus into the throat and back of your nose. Being overweight, having sleep apnea, or following certain dietary and lifestyle habits can increase your chances of having LPR. Adults, seniors and children If you have any can suffer from LPR symptoms. questions, please Symptoms of LPRD ask your nurse or Adults with LPRD may have the following symptoms: ■ Sour taste in your throat physician. ■ More mucus in your throat ■ Frequent throat clearing ■ Post nasal drip ■ Hoarseness ■ Sore throat ■ Difficulty swallowing ■ Feeling that something is stuck in your throat Testing for LPRD If your physician thinks that you may have LPRD, he or she will examine your throat. An otolaryngologist (or ear, nose and throat physician) will use a special camera called an endoscope to look at your throat. If your throat and/or voice box is swollen and/or red, you may have LPRD that requires treatment. Your physician may recommend that you see a gastroenterologist (stomach and bowel specialist) or have further testing. A barium swallow test or a 24 pH-metry test may be needed if there are concerns about your symptoms or findings. Treatments for laryngopharyngeal reflux LPRD symptoms may resolve with medications, diet/lifestyle changes or both. Medications for LPRD LPRD may be treated with medications called proton pump inhibitors (PPI). -

Laryngopharyngeal Reflux; PPI = Proton Pump Inhibitors; RSS-12 = Reflux Symptom Score-12
Journal of Clinical Medicine Review Laryngopharyngeal Reflux: A State-of-the-Art Algorithm Management for Primary Care Physicians 1,2,3,4,5, , 1,4,5, 6 7 Jerome R. Lechien * y , Sven Saussez y, Vinciane Muls , Maria R. Barillari , 8 2,3,5, 9, Carlos M. Chiesa-Estomba , Stéphane Hans z and Petros D. Karkos z 1 Department of Human Anatomy and Experimental Oncology, Mons School of Medicine, UMONS Research Institute for Health Sciences and Technology, University of Mons (UMons), B7000 Mons, Belgium; [email protected] 2 Department of Otolaryngology-Head & Neck Surgery, Foch Hospital, School of Medicine, UFR Simone Veil, Université Versailles Saint-Quentin-en-Yvelines (Paris Saclay University), 92150 Paris, France; [email protected] 3 Department of Otolaryngology-Head & Neck Surgery, Ambroise Paré Hospital, APHP, Paris Saclay University, 92150 Paris, France 4 Department of Otolaryngology-Head & Neck Surgery, CHU Saint-Pierre, Faculty of Medicine, University Libre de Bruxelles, 1000 Brussels, Belgium 5 Department of Otolaryngology-Head & Neck Surgery, CHU Ambroise Paré, 92150 Paris, France 6 Division of Gastroenterology and Endoscopy, CHU Saint-Pierre, Faculty of Medicine, University Libre de Bruxelles, 1000 Brussels, Belgium; [email protected] 7 Division of Phoniatrics and Audiology, Department of Mental and Physical Health and Preventive Medicine, University of Naples SUN, 34103 Naples, Italy; [email protected] 8 Department of Otorhinolaryngology-Head & Neck Surgery, Hospital Universitario Donostia, 00685 San Sebastian, Spain; [email protected] 9 Department of Otorhinolaryngology and Head and Neck Surgery, AHEPA University Hospital, Thessaloniki Medical School, 54621 Thessaloniki, Greece; [email protected] * Correspondence: [email protected]; Tel.: +32-65-373-584 Authors have equally contributed to the paper’s supervision and should be considered as co-first authors. -

The Prevalence of Laryngopharyngeal Reflux in the English Population
Eur Arch Otorhinolaryngol (2012) 269:2219–2225 DOI 10.1007/s00405-012-2028-1 LARYNGOLOGY The prevalence of laryngopharyngeal reflux in the English population Tawakir Kamani • Susannah Penney • Indu Mitra • Vijay Pothula Received: 12 December 2011 / Accepted: 23 March 2012 / Published online: 11 May 2012 Ó Springer-Verlag 2012 Abstract Although symptoms of laryngopharyngeal Keywords Laryngopharyngeal reflux Á reflux (LPR) symptoms are commonly seen in the ENT Gastro-oesophageal reflux disease clinic, their aetiology and prevalence in the population remain unknown. Lifestyle changes have been seen to be effective in symptom relief. We aimed to establish the Introduction prevalence of these symptoms and identify any associated factors. Pseudo-random sampling was performed on 2,000 Laryngopharyngeal reflux (LPR) is defined as the retro- adults that were sent a validated questionnaire containing grade movement of gastric contents into the larynx and the Reflux Symptom Index (RSI) and questions on their pharynx leading to a diversity of upper aero digestive health and lifestyle. 45.8 % of the 378 responders were tract symptoms. LPR has also been termed as extra- male. The mean RSI was 8.3. 30 % had an RSI of more esophageal or silent reflux. Patients most commonly than 10, of which 75 % had symptoms of gastro-oesoph- present with the symptoms of hoarseness, foreign body ageal reflux disease (r = 0.646 at p = 0.01). Patients with sensation within the throat, sore throat, dysphagia, post- depression and irritable bowel syndrome are more likely to nasal drip, excessive throat mucous, chronic cough and have LPR symptoms. LPR symptoms are highly prevalent repeated throat clearing [1, 2]. -

Detecting the Other Reflux Disease
Amin Madani, HBSc; Leigh Sowerby, MD; James C. Gregor, MD, Detecting the other refl ux FRCPC; Eric Wong, MD, MClSc(FM), CCFP; Kevin Fung, MD, disease FRCSC, FACS Schulich School of Laryngopharyngeal refl ux is a disorder, unlike GERD, Medicine & Dentistry (Mr. Madani and that few patients (and too few physicians) are familiar Dr. Wong); Department of Otolaryngology–Head and with. Misdiagnosis is common—unless you know what Neck Surgery (Dr. Sowerby); Department of Otolaryngology, to look for. Division of Head and Neck Oncology and Reconstructive Surgery (Dr. Fung); and Department of Medicine (Dr. Gregor), aryngopharyngeal refl ux (LPR), the retrograde move- University of Western Ontario, PRACTICE ment of gastric content into the upper aerodigestive London, ON, Canada RECOMMENDATIONS tract, is a common—and commonly underdiagnosed— kevin.fung@ L lhsc.on.ca › Suspect laryngopharyngeal condition. Characterized by infl ammation of the laryngophar- refl ux (LPR) in a patient ynx, LPR can coexist with gastroesophageal refl ux disease The authors reported no potential with chronic laryngitis; confl ict of interest relevant to this (GERD), but it is a distinct disorder.1 In GERD, the lower article. 50% to 60% of such cases esophageal sphincter malfunctions, whereas LPR involves a are related to LPR. B dysfunctional upper esophageal sphincter. › Refer patients with risk fac- Because both conditions involve acid refl ux, LPR is some- tors for head and neck cancer times mistaken for GERD. Often, too, patients and physicians or whose symptoms persist alike attribute LPR’s signs and symptoms, which are largely despite lifestyle modification and medical management nonspecifi c, to other causes.