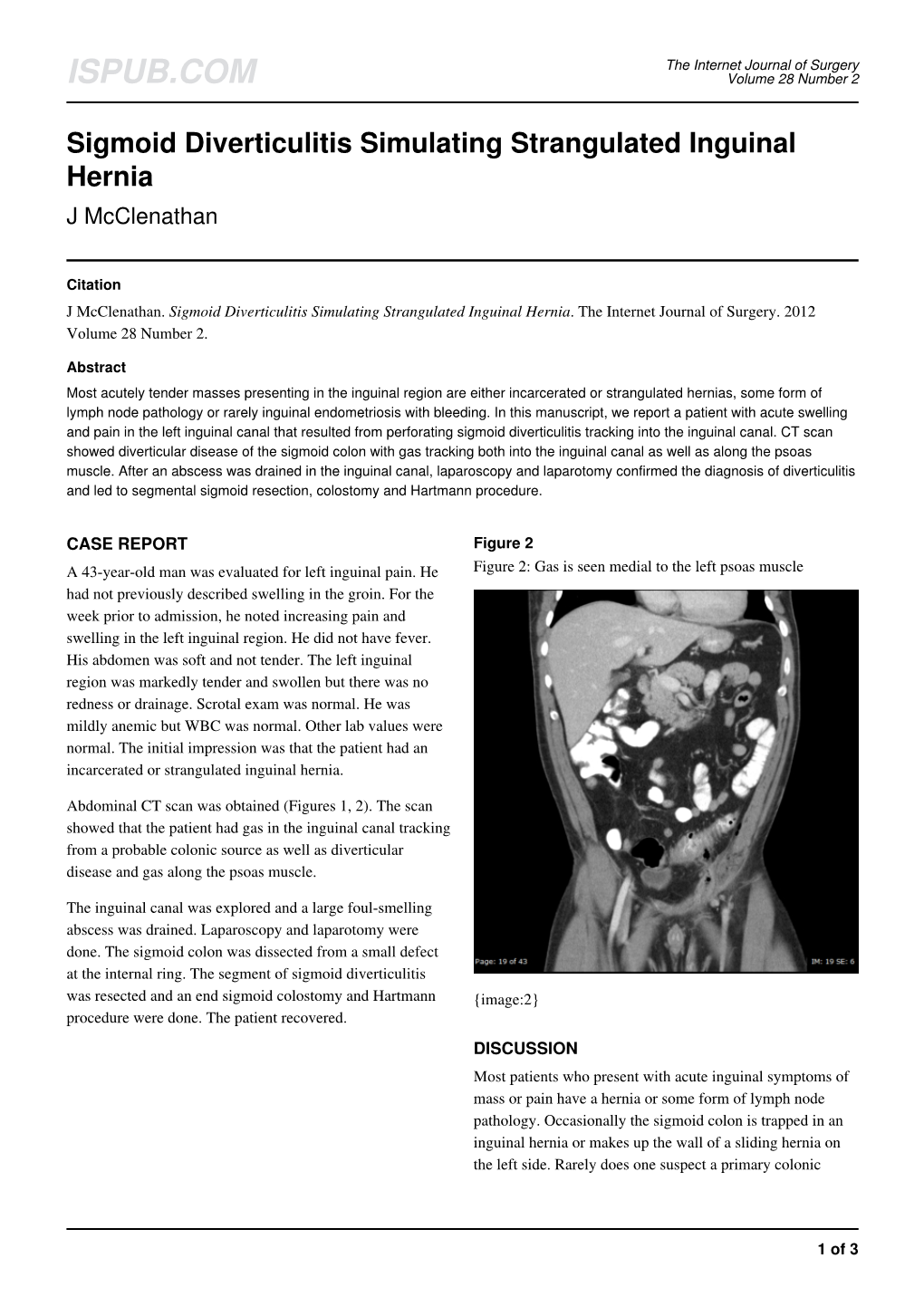
Sigmoid Diverticulitis Simulating Strangulated Inguinal Hernia J Mcclenathan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diverticular Abscess Presenting As a Strangulated Inguinal Hernia: Case Report and Review of the Literature
Ulster Med J 2007; 76 (2) 107-108 Presidential Address 107 Case Report Diverticular Abscess Presenting as a Strangulated Inguinal Hernia: Case Report and review of the literature. S Imran H Andrabi, Ashish Pitale*, Ahmed AS El-Hakeem Accepted 22 December 2006 ABSTRACT noted nausea, anorexia and increasing abdominal pain. She had no previous history of any surgery or trauma and was on Potentially life threatening diseases can mimic a groin hernia. warfarin for atrial fibrillation. We present an unusual case of diverticulitis with perforation and a resulting abscess presenting as a strangulated inguinal hernia. The features demonstrated were not due to strangulation of the contents of the hernia but rather pus tracking into the hernia sac from the peritoneal cavity. The patient underwent sigmoid resection and drainage of retroperitoneal and pericolonic abscesses. Radiological and laboratory studies augment in reaching a diagnosis. The differential diagnosis of inguinal swellings is discussed. Key Words: Diverticulitis, diverticular perforation, diverticular abscess, inguinal hernia INTRODUCTION The association of complicated inguinal hernia and diverticulitis is rare1. Diverticulitis can present as left iliac fossa pain, rectal bleeding, fistulas, perforation, bowel obstruction and abscesses. Our patient presented with a diverticular perforation resulting in an abscess tracking into the inguinal canal and clinically masquerading as a Fig 2. CT scan showing inflammatory changes with strangulated inguinal hernia. The management warranted an stranding of the subcutaneous fat in the left groin and a exploratory laparotomy and drainage of pus. large bowel diverticulum CASE REPORT On admission, she had a tachycardia (pulse 102 beats/min) and a temperature of 37.5OC. -

Clinical Acute Abdominal Pain in Children
Clinical Acute Abdominal Pain in Children Urgent message: This article will guide you through the differential diagnosis, management and disposition of pediatric patients present- ing with acute abdominal pain. KAYLEENE E. PAGÁN CORREA, MD, FAAP Introduction y tummy hurts.” That is a simple statement that shows a common complaint from children who seek “M 1 care in an urgent care or emergency department. But the diagnosis in such patients can be challenging for a clinician because of the diverse etiologies. Acute abdominal pain is commonly caused by self-limiting con- ditions but also may herald serious medical or surgical emergencies, such as appendicitis. Making a timely diag- nosis is important to reduce the rate of complications but it can be challenging, particularly in infants and young children. Excellent history-taking skills accompanied by a careful, thorough physical exam are key to making the diagnosis or at least making a reasonable conclusion about a patient’s care.2 This article discusses the differential diagnosis for acute abdominal pain in children and offers guidance for initial evaluation and management of pediatric patients presenting with this complaint. © Getty Images Contrary to visceral pain, somatoparietal pain is well Pathophysiology localized, intense (sharp), and associated with one side Abdominal pain localization is confounded by the or the other because the nerves associated are numerous, nature of the pain receptors involved and may be clas- myelinated and transmit to a specific dorsal root ganglia. sified as visceral, somatoparietal, or referred pain. Vis- Somatoparietal pain receptors are principally located in ceral pain is not well localized because the afferent the parietal peritoneum, muscle and skin and usually nerves have fewer endings in the gut, are not myeli- respond to stretching, tearing or inflammation. -

Incarcerated Gallbladder in Inguinal Hernia: a Case Report and Literature
Tajti Jr. et al. BMC Gastroenterol (2020) 20:425 https://doi.org/10.1186/s12876-020-01569-5 CASE REPORT Open Access Incarcerated gallbladder in inguinal hernia: a case report and literature review János Tajti Jr., József Pieler, Szabolcs Ábrahám, Zsolt Simonka, Attila Paszt and György Lázár* Abstract Background: Treating hernias is one of the oldest challenges in surgery. The gallbladder as content in the case of abdominal hernias has only been reported in a few cases in the current literature. Cholecyst has only been described in the content of an inguinofemoral hernia in one case to date. Case presentation: A 73-year-old female patient was admitted to the Emergency Department due to complaints in the right inguinal area, which had started 1 day earlier. The patient complained of cramp-like abdominal pain and nausea. Physical examination confrmed an apple-sized, irreducible hernia in the right inguinal region. Abdominal ultrasound confrmed an oedematous intestinal loop in a 70-mm-long hernial sac, with no circulation detected. Abdominal X-ray showed no signs of passage disorder. White blood cell count and C-reactive protein level were elevated, and hepatic enzymes were normal in the laboratory fndings. Exploration was performed via an inguinal incision on the right side, an uncertain cystic structure was found in the hernial sac, and several small abnormal masses were palpated there. The abdominal cavity was explored from the middle midline laparotomy. During the exploration, the content of the hernial sac was found to be the fundus of the signifcantly ptotic, large gallbladder. Cholecystectomy and Bassini’s repair of the inguinal hernia were performed safely. -

Pediatric Hernia
Pediatric Surgery Pediatric Hernia Pediatric Hernias: Definitions, Diagnosis and Treatment Hernia repair is among the most common type of general surgical procedure performed in children each year. The two most common types of congenital hernias in children are umbilical and inguinal hernias. The infor- mation below offers information on symptoms, diagnosis and treatment of these medical conditions. Umbilical Hernia Umbilical hernias are fairly common among newborns and infants younger than 6 months. Caused when the umbilical ring fails to close after birth, umbilical hernias present as an outward bulging in the abdominal area at the umbilicus. Umbilical hernias can vary in width from less than 1 cm to more than 5 cm and may seem to expand when the child cries or strains. Although the exact incidence of umbilical hernias in children is unknown, they are reported slightly more often in African Americans. Symptoms and Diagnosis • Present as a soft swelling at the navel that bulges when the baby or child sits up, cries or strains and usually disappears when the baby or child lies flat. • Usually painless. • Often detected on physical exam, without the need for additional testing. Treatment • Often closes by 1 or 2 years of age. • Surgery needed when hernia has not closed by 2 to 4 years of age. • Emergency surgery required if intestinal blood supply is cut off (strangulation). Inguinal Hernias There are two types of inguinal hernias — direct and indirect. Direct inguinal hernias are very rare in children and are caused by a weakness in the abdominal wall that allows intestines to protrude through. -

Patient Selection Criteria
M∙ACS MACS Patient Selection Criteria The objective is to screen, on a daily basis, the Acute Care Surgical service “touches” at your hospital to identify patients who meet criteria for further data entry. The specific patient diseases/conditions that we are interested in capturing for emergent general surgery (EGS) are: 1. Acute Appendicitis 2. Acute Gallbladder Disease a. Acute Cholecystitis b. Choledocholithiasis c. Cholangitis d. Gallstone Pancreatitis 3. Small Bowel Obstruction a. Adhesive b. Hernia 4. Emergent Exploratory Laparotomy (Refer to the ex-lap algorithm under the Diseases or Conditions section below for inclusion/exclusion criteria.) The daily census for patients admitted to the Acute Care Surgery Service or seen as a consult will have to be screened. There may be other sources to accomplish this screening such as IT and we are interested in learning about these sources from you. From this census, a list can be compiled of patients with the aforementioned diseases/conditions. The first level of data entry involves capture and entry of the patient into the MACS Qualtrics database. All patients with the identified diseases/conditions will have data entered regardless of whether or not they received an operation during admission/ED visit. The second level of data entry takes place if an existing MACS patient returns to the hospital (ED or admission) or has outcome events identified within the 30-day post-operative time frame if the patient had surgery, or within 30 days from discharge for the non-operative patients. You will see that we are capturing diagnostic, interventional, and therapeutic data that extend beyond what is typically captured for MSQC patients. -

Management of Incidental Amyand Hernia with a Case Report
CASE REPORT East J Med 24(4): 551-553, 2019 DOI: 10.5505/ejm.2019.82787 Management of Incidental Amyand Hernia With A Case Report Tolga Kalayci*, Ümit Haluk Iliklerden Department of General Surgery,Yuzuncu Yil University Faculty of Medicine,Van,Turkey ABSTRACT The presence of appendix vermiformis in inguinal hernia is known as Amyand hernia. Amyand hernia is a rare condition estimated to account for approximately 1% of all inguinal hernias. In our case we want to show our approach to incidental Amyand hernia. An 80-year-old male patient was received at urology service at Van Yuzuncu Yil University Department of Medicine because of prostatic symptoms. There were comorbid factors like hypertension,chronic obstructive lung disease and geriatric age. On surgery with spinal anesthesia, surgeons invited us to evaluate his left inguinal hernia. We evaluated hernia and saw distal ileal segments, proximal right colonic segments and inflamme appendix at hernia defect. Because of appendix inflammation we performed appendectomy. Hernia was repaired with mesh. We put a drain at surgery area. At postoperative first day, the patient discharged with drain. The fifth day of post-surgery, the drain was pulled out. At the time of 1st and 3rd month check of the patient, there was no problem about surgery. Amyand hernia is one of the rare conditions encountered by the surgeon during hernia surgery. The surgeon must know the Rosanoff and Bassoon Classification of Amyand Hernia to successfully manage Amyand hernia surgery. The surgeon also must know the situation in which case an appendectomy should be performed and in which case the mesh should be used. -

Surgical Management of Primary Crohn's Disease
Open Access Austin Journal of Gastroenterology Special Article - Crohn’s Disease and Colitis Surgical Management of Primary Crohn’s Disease Makni A*, Magherbi H, El Héni A, Daghfous A, Rebai W, Chebbi F, Fterich F, Ksantini R, Jouini Abstract M, Kacem M and Ben Safta Z Inflammatory bowel disease is a chronic gastrointestinal condition that is Department of General Surgery ‘A’, La Rabta Hospital, characterized by chronic gastrointestinal inflammation. The management of Tunisia Crohn’s disease is complex and requires skill, knowledge and experience with *Corresponding author: Makni Amin, Department current advances in the field. Over the past several years, there have been of General Surgery ‘A’, La Rabta Hospital, Jabbari 1007, a number of achievements and progress made in the care and management Tunis, Tunis El Manar University, Faculty of Medicine of of this disorder. The diagnostic tools have greatly improved. The therapeutic Tunis, 15 Rue Djebel Akhdhar, Tunisia armamentarium has expanded. The genetics of IBD has become more detailed and the role of the gut microbiome has been better defined. The evolution Received: February 14, 2017; Accepted: March 13, of biological agents has revolutionized the way we approach this disease. 2017; Published: March 24, 2017 However, surgery is still required in more than 80% of patients with Crohn’s disease (CD). This article aims to study the epidemiological, anatomical and therapeutic principles of surgical forms of CD. Keywords: Crohn’s disease; Surgery; Recurrence; Stricture; Fistula Introduction we should assess the severity and type of symptoms, failure of medical treatment, the onset of adverse effects and surgical risk/ Surgery is required in more than 80% of patients with Crohn’s benefit. -

A Case of Richter's Hernia Presenting After a Previous Inguinal
International Surgery Journal Bali S et al. Int Surg J. 2016 Aug;3(3):1688-1690 http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902 DOI: http://dx.doi.org/10.18203/2349-2902.isj20162778 Case Report A case of Richter’s hernia presenting after a previous inguinal herniorrhaphy Sharadendu Bali, Maneshwar Singh Utaal*, Navdeep Garg Department of Surgery, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India Received: 11 June 2016 Accepted: 15 July 2016 *Correspondence: Dr. Maneshwar Singh Utaal, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Richter hernia also known as partial enterocele is the protrusion or/and strangulation of only a part of the circumference of the intestinal antimesenteric border through a small defect of the abdominal wall. These comprise around 10 percent of strangulated hernias, which itself represent a small percent in overall hernia cases, hence are very rare. If left untreated, the affected bowel segment becomes ischemic and finally gangrenous, and it should be kept in mind that patients with Richter hernia develop gangrene much faster than ‘ordinary’ strangulated hernias. This is a case report of a 69-year-old male with a history of herniorrhaphy for left inguinal hernia 22 years back presenting with swelling in left groin region for 4 days with sudden onset of left-sided acute abdominal pain and vomiting for 1 day. -

Allergic Response Is Due to an Unknown Allergen Strangulated
Postgrad Med J: first published as 10.1136/pgmj.29.332.323 on 1 June 1953. Downloaded from June 1953 Clinical Section 323 curring in the above case is difficult to correlate. allergic response is due to an unknown allergen Before the appearance of rash on the face the and the finding of tuberculosis is just a coincident. patient gave a history of sore throat and joint pains, Whatever may have been the cause of the original and as the throat swab and the E.N.T. reports illness, this case clearly emphasizes the point were both negative it is suggested that initially which MacKenna (I95I) makes in his excellent she had subclinical tubercular infection of her review on the pathogenesis and treatment of all tonsils which, when the patient's resistance was forms of lupus erythematosus, that unless the lowered after the pelvic operation, spread to the etiology of the disease is well established no cervical glands and later by the blood stream treatment can be of lasting value and that perhaps causing miliary changes in kidneys, spleen and more than one factor is responsible for this intestinal glands as observed at necropsy. It is dreaded malady. difficult to understand why the lungs escaped this miliary invasion. Lupus erythematosus of the face Summary can be regarded as an allergic response in the A case presenting an unusual combination of collagen tissue of the face and the harmful agent, lupus erythematosus, periarteritis nodosa and as subsequent course showed, may have been a miliary tuberculosis, not hitherto recorded, is tubercular focus. -

S PATIENT INFORMATION Oregon Surgical Specialists
S PATIENT INFORMATION oregon surgical specialists Hernia (Updated 10.08) A hernia is a weakness in the wall of your abdomen. When you lift a heavy load, or when pressure in the abdomen increases, as when you cough, abdominal organs and tissues push against the wall. If the pressure is enough, they can push though at the weak spot, bulging out in a lump that you may be able to feel under your skin. This is not always painful, and you may be able to push the lump back inside Then it is called a reducible hernia. Unfortunately, weak areas in your abdominal wall do not heal on their own but usually become weaker with aging and activity. If part of your intestine protrudes through a hernia, it can become trapped (incarcerated), strangling the intestine and causing a bowel obstruction. This can become a life-threatening situation, requiring emergency surgery to repair the damage. Thus, it is best to treat and repair a hernia before an emergency arises. The abdominal wall is made up of layers that provide strength, including muscle, fat, connective tissue, and peritoneum. The most common kinds of hernias are called inguinal, umbilical, and femoral, because of the natural weak spots in the wall in those locations: the inguinal (groin), umbilical (naval), and femoral areas (just below the groin). A fourth common kind of hernia is an incisional hernia, which occurs where the incision from a previous surgery has created a weakened area. A less common condition is a Hiatal hernia which occur at the top of the stomach, when a weak spot in the diaphragm allows the stomach to move up into the chest cavity. -

Guide to Understanding Hernias Hernias Do Not Heal by Themselves and May Continue to Worsen If Ignored
Guide to Understanding Hernias Hernias do not heal by themselves and may continue to worsen if ignored. Let our specialists treat your hernia before it becomes an emergency. What Is a Hernia? A hernia is a very common health condition in men and women and occurs when internal tissue or part of an organ bulges through a weak muscle into a place where it doesn’t belong. Hernias usually occur either because of a natural weakness in the abdominal wall or from excessive strain on the abdominal wall, such as the strain from heavy lifting, substantial weight gain or persistent coughing. The most common types of hernias include: Groin (inguinal) Hernia The most common type of hernia, the inguinal hernia, occurs when a structure in your abdomen — typically Signs and Symptoms part of your small intestine or fatty tissue — bulges Not all hernias cause symptoms. However, if you have through your abdominal wall and into your inner groin. a hernia, you may experience any of the following Inguinal hernias most often occur in men. symptoms: Upper Thigh (femoral) Hernia • A bulge on one or both sides of your groin (the bulge More commonly known in women than men, a femoral may appear to go away while you’re lying down) hernia occurs when fatty tissue or part of the intestine • Pain in the groin area, particularly while you exercise, bulges through into your outer groin. lift, strain, have a bowel movement or cough (the pain Hiatal Hernia or discomfort usually goes away when you rest) This happens when the upper part of your stomach • Sharp abdominal pain bulges into your chest through a small opening in your • Discomfort in the groin area, such as itching, aching, diaphragm (the muscle separating your abdomen from burning, heaviness or weakness your chest). -

A Case Report of Unexpected Pathology Within an Incarcerated Ventral Hernia
Accepted Manuscript Title: A case report of unexpected pathology within an incarcerated ventral hernia Authors: Erica D. Kane, Katharine R. Bittner, Michelle Bennet, John R. Romanelli, Neal E. Seymour, Jacqueline J. Wu PII: S2210-2612(17)30310-3 DOI: http://dx.doi.org/doi:10.1016/j.ijscr.2017.07.004 Reference: IJSCR 2618 To appear in: Received date: 5-5-2017 Revised date: 13-6-2017 Accepted date: 3-7-2017 Please cite this article as: Kane Erica D, Bittner Katharine R, Bennet Michelle, Romanelli John R, Seymour Neal E, Wu Jacqueline J.A case report of unexpected pathology within an incarcerated ventral hernia.International Journal of Surgery Case Reports http://dx.doi.org/10.1016/j.ijscr.2017.07.004 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. A case report of unexpected pathology within an incarcerated ventral hernia Erica D. Kane, MD, MPHa; Katharine R. Bittner, MDa; Michelle Bennet, BSb; John R. Romanelli, MDa; Neal E. Seymour, MDa; Jacqueline J. Wu, MDa a: Department of Surgery, Baystate Medical Center, University of Massachusetts Medical School, Springfield, MA. b: Tufts University School of Medicine, Boston, MA. Corresponding author: Erica Kane, MD, MPH Baystate Medical Center, Department of Surgery 759 Chestnut Street Springfield, Ma 01199 Mobile: 314-974-0458 Work: 413-794-5165 Fax: 413-794-1835 Email: [email protected] Authors’ email addresses: Katharine R.