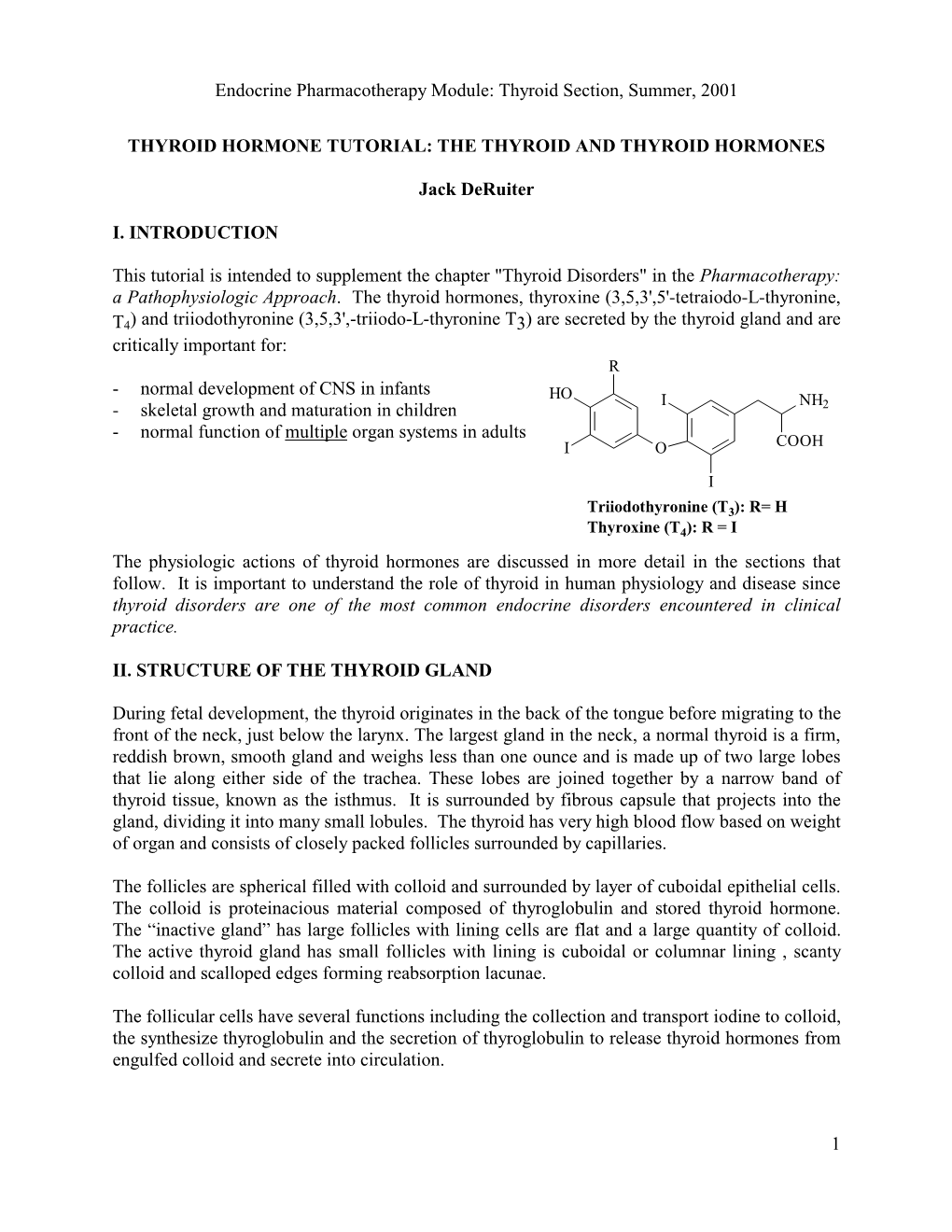
Endocrine Pharmacotherapy Module: Thyroid Section, Summer, 2001
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Actions of Vasoactive Intestinal Peptide on the Rat Adrenal Zona Glomerulosa
51 Actions of vasoactive intestinal peptide on the rat adrenal zona glomerulosa J P Hinson, J R Puddefoot and S Kapas1 Molecular and Cellular Biology Section, Division of Biomedical Sciences, St Bartholomew’s and The Royal London School of Medicine and Dentistry, Queen Mary and Westfield College, Mile End Road, London E1 4NS, UK 1Oral Diseases Research Centre, St Bartholomew’s and The Royal London School of Medicine and Dentistry, 2 Newark Street, London E1 2AT, UK (Requests for offprints should be addressed to J P Hinson) Abstract Previous studies, by this group and others, have shown that The response to VIP in adrenals obtained from rats fed vasoactive intestinal peptide (VIP) stimulates aldosterone a low sodium diet was also investigated. Previous studies secretion, and that the actions of VIP on aldosterone have found that adrenals from animals on a low sodium secretion by the rat adrenal cortex are blocked by â diet exhibit increased responsiveness to VIP. Specific VIP adrenergic antagonists, suggesting that VIP may act by binding sites were identified, although the concentration the local release of catecholamines. The present studies or affinity of binding sites in the low sodium group was not were designed to test this hypothesis further, by measur- significantly different from the controls. In the low sodium ing catecholamine release by adrenal capsular tissue in group VIP was found to increase catecholamine release to response to VIP stimulation. the same extent as in the control group, however, in Using intact capsular tissue it was found that VIP caused contrast to the control group, the adrenal response to VIP a dose-dependent increase in aldosterone secretion, with a was not altered by adrenergic antagonists in the low concomitant increase in both adrenaline and noradrenaline sodium group. -

Affect Breast Cancer Risk
HOW HORMONES AFFECT BREAST CANCER RISK Hormones are chemicals made by the body that control how cells and organs work. Estrogen is a female hormone made mainly in the ovaries. It’s important for sexual development and other body functions. From your first monthly period until menopause, estrogen stimulates normal breast cells. A higher lifetime exposure to estrogen may increase breast cancer risk. For example, your risk increases if you start your period at a young age or go through menopause at a later age. Other hormone-related risks are described below. Menopausal hormone therapy Pills Menopausal hormone therapy (MHT) is The U.S. Food and Drug Administration also known as postmenopausal hormone (FDA) recommends women use the lowest therapy and hormone replacement dose that eases symptoms for the shortest therapy. Many women use MHT pills to time needed. relieve hot flashes and other menopausal Any woman currently taking or thinking symptoms. MHT should be used at the Birth control about taking MHT pills should talk with her lowest dose and for the shortest time pills (oral doctor about the risks and benefits. contraceptives) needed to ease menopausal symptoms. Long-term use can increase breast cancer Vaginal creams, suppositories Current or recent use risk and other serious health conditions. and rings of birth control pills There are 2 main types of MHT pills: slightly increases breast Vaginal forms of MHT do not appear to cancer risk. However, estrogen plus progestin and estrogen increase the risk of breast cancer. However, this risk is quite small alone. if you’ve been diagnosed with breast cancer, vaginal estrogen rings and suppositories are because the risk of Estrogen plus progestin MHT breast cancer for most better than vaginal estrogen creams. -

HORMONES and SPORT Insulin, Growth Hormone and Sport
13 HORMONES AND SPORT Insulin, growth hormone and sport P H Sonksen Guy’s, King’s and St Thomas’ School of Medicine, St Thomas’ Hospital, London SE1 7EH, UK; Email: [email protected] Abstract This review examines some interesting ‘new’ histories of blood rather than urine samples. The first method has a insulin and reviews our current understanding of its window of opportunity lasting about 24 h after an injec- physiological actions and synergy with GH in the regu- tion and is most suitable for ‘out of competition’ testing. lation of metabolism and body composition. It reviews the The second method has reasonable sensitivity for as long as history of GH abuse that antedates by many years the 2 weeks after the last injection of GH and is uninfluenced awareness of endocrinologists to its potent anabolic actions. by extreme exercise and suitable for post-competition Promising methods for detection of GH abuse have been samples. This method has a greater sensitivity in men than developed but have yet to be sufficiently well validated to in women. The specificity of both methods seems accept- be ready for introduction into competitive sport. So far, ably high but lawyers need to decide what level of there are two promising avenues for detecting GH abuse. scientific probability is needed to obtain a conviction. Both The first uses immunoassays that can distinguish the methods need further validation before implementation. isomers of pituitary-derived GH from the monomer of Research work carried out as part of the fight against recombinant human GH. The second works through doping in sport has opened up a new and exciting area of demonstrating circulating concentrations of one or more endocrinology. -

Thyroid Hormones in Fetal Growth and Prepartum Maturation
A J FORHEAD and A L FOWDEN Thyroid hormones and fetal 221:3 R87–R103 Review development Thyroid hormones in fetal growth and prepartum maturation A J Forhead1,2 and A L Fowden1 Correspondence should be addressed 1Department of Physiology, Development and Neuroscience, University of Cambridge, Physiology Building, to A L Fowden Downing Street, Cambridge CB2 3EG, UK Email 2Department of Biological and Medical Sciences, Oxford Brookes University, Oxford OX3 0BP, UK [email protected] Abstract The thyroid hormones, thyroxine (T4) and triiodothyronine (T3), are essential for normal Key Words growth and development of the fetus. Their bioavailability in utero depends on " thyroid hormones development of the fetal hypothalamic–pituitary–thyroid gland axis and the abundance " intrauterine growth of thyroid hormone transporters and deiodinases that influence tissue levels of bioactive " maturation hormone. Fetal T4 and T3 concentrations are also affected by gestational age, nutritional and " neonatal adaptation endocrine conditions in utero, and placental permeability to maternal thyroid hormones, which varies among species with placental morphology. Thyroid hormones are required for the general accretion of fetal mass and to trigger discrete developmental events in the fetal brain and somatic tissues from early in gestation. They also promote terminal differentiation of fetal tissues closer to term and are important in mediating the prepartum maturational effects of the glucocorticoids that ensure neonatal viability. Thyroid hormones act directly through anabolic effects on fetal metabolism and the stimulation of fetal oxygen Journal of Endocrinology consumption. They also act indirectly by controlling the bioavailability and effectiveness of other hormones and growth factors that influence fetal development such as the catecholamines and insulin-like growth factors (IGFs). -

Recent Advances in Vasoactive Intestinal Peptide Physiology And
F1000Research 2019, 8(F1000 Faculty Rev):1629 Last updated: 28 NOV 2019 REVIEW Recent advances in vasoactive intestinal peptide physiology and pathophysiology: focus on the gastrointestinal system [version 1; peer review: 4 approved] Mari Iwasaki1, Yasutada Akiba 1,2, Jonathan D Kaunitz 1,3 1Greater Los Angeles Veterans Affairs Healthcare System, Los Angeles, CA, USA 2Department of Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA 3Departments of Medicine and Surgery, UCLA School of Medicine, Los Angeles, CA, USA First published: 12 Sep 2019, 8(F1000 Faculty Rev):1629 ( Open Peer Review v1 https://doi.org/10.12688/f1000research.18039.1) Latest published: 12 Sep 2019, 8(F1000 Faculty Rev):1629 ( https://doi.org/10.12688/f1000research.18039.1) Reviewer Status Abstract Invited Reviewers Vasoactive intestinal peptide (VIP), a gut peptide hormone originally 1 2 3 4 reported as a vasodilator in 1970, has multiple physiological and pathological effects on development, growth, and the control of neuronal, version 1 epithelial, and endocrine cell functions that in turn regulate ion secretion, published nutrient absorption, gut motility, glycemic control, carcinogenesis, immune 12 Sep 2019 responses, and circadian rhythms. Genetic ablation of this peptide and its receptors in mice also provides new insights into the contribution of VIP towards physiological signaling and the pathogenesis of related diseases. F1000 Faculty Reviews are written by members of Here, we discuss the impact of VIP on gastrointestinal function and the prestigious F1000 Faculty. They are diseases based on recent findings, also providing insight into its possible commissioned and are peer reviewed before therapeutic application to diabetes, autoimmune diseases and cancer. -

Diabetes Is a Disease in Which the Body's Ability to Produce Or Respond
Early Signs and Symptoms of diabetes: Early symptoms of diabetes, especially type 2 diabetes, can be subtle or seemingly harmless. Over time, however, you may Diabetes is a disease in which the develop diabetes complications, even if you body’s ability to produce or respond to haven't had diabetes symptoms. In the the hormone insulin is impaired, United States alone, more than 8 million resulting in abnormal metabolism of people have undiagnosed diabetes, Treatments: carbohydrates and elevated levels of according to the American Diabetes Association. Understanding possible glucose (sugar) in the blood. • Insulin therapy diabetes symptoms can lead to early • Oral medications diagnosis and treatment and a lifetime of Diabetes can be broken down into • better health. If you're experiencing any of Diet changes two types, Type 1 and Type 2. Type 1 • Exercise diabetes involves the the following diabetes signs and symptoms, see your doctor. body attacking itself by The medications you take vary by mistake, this then the type of diabetes and how well the causes the body to stop making insulin. With medicine controls you blood glucose levels. Type 2 diabetes the Type 1 diabetics must have insulin. Type 2 body does not respond may or may not include insulin and may just like it should to the be controlled with diet and exercise alone. insulin the pancreas is If you notice any of these changes notify making. Your body tells the pancreas that it needs to make more insulin since the your health care provider. The earlier • insulin that is already there is not working. -

PROGESTERONE? PO Box12004 Like Estrogen, Which Gets Much More Public Attention, Progesterone Is a Female Sex Hormone
FOLD FOLD FOLD DO NOT PRINT DO NOT PRINT DO NOT PRINT Overland Park,KS66282 WHAT IS PROGESTERONE? PO Box12004 Like estrogen, which gets much more public attention, progesterone is a female sex hormone. Women produce it in the ovaries and adrenal glands, and during pregnancy in the placenta. With all the talk about estrogen, progesterone is sometimes left behind as the forgotten female hormone. UNDERSTANDING WHAT ARE HORMONES AND HOW DO THEY WORK? IS PROGESTIN THE SAME THING AS PROGESTERONE? Hormones are our bodies’ chemical messengers. PROGESTERONE They travel through the bloodstream to trigger certain No. Although these terms are often used interchangeably, activities or changes in the body. Hormones work by they do not mean the same thing. Progesterone refers binding to specialized areas of cells known as receptor to the hormone produced in the body, or produced sites. There they initiate a chain of events in specific from a plant source but still chemically identical to cells or organs. For example, progesterone has been human progesterone. In contrast, progestin is a known to initiate a calming effect in the brain, hormone that is synthetically produced and may differ reducing anxiety. in structure to progesterone. You may also have heard of progestogens. This is a general term that applies WHAT DOES PROGESTERONE DO? to the category of both natural and synthetic hormones that act like progesterone in the uterus. See the During the reproductive years, progesterone prepares difference in the molecular structure depicted below. the uterine lining (or womb) for pregnancy. Each month, progesterone levels rise following ovulation. -

Testosterone: a Metabolic Hormone in Health and Disease
D M KELLY and T H JONES Testosterone metabolic hormone 217:3 R25–R45 Review Testosterone: a metabolic hormone in health and disease Daniel M Kelly1 and T Hugh Jones1,2 Correspondence should be addressed to 1Department of Human Metabolism, Medical School, The University of Sheffield, Sheffield S10 2RX, UK 2Robert T H Jones Hague Centre for Diabetes and Endocrinology, Barnsley Hospital NHS Foundation Trust, Gawber Road, Barnsley S75 Email 2EP, UK [email protected] Abstract Testosterone is a hormone that plays a key role in carbohydrate, fat and protein metabolism. Key Words It has been known for some time that testosterone has a major influence on body fat " metabolism composition and muscle mass in the male. Testosterone deficiency is associated with an " testosterone increased fat mass (in particular central adiposity), reduced insulin sensitivity, impaired " type 2 diabetes glucose tolerance, elevated triglycerides and cholesterol and low HDL-cholesterol. All these " metabolic syndrome factors are found in the metabolic syndrome (MetS) and type 2 diabetes, contributing to cardiovascular risk. Clinical trials demonstrate that testosterone replacement therapy improves the insulin resistance found in these conditions as well as glycaemic control and also reduces body fat mass, in particular truncal adiposity, cholesterol and triglycerides. The mechanisms by which testosterone acts on pathways to control metabolism are not fully clear. There is, however, an increasing body of evidence from animal, cell and clinical studies that testosterone at the molecular level controls the expression of important regulatory proteins involved in Journal of Endocrinology glycolysis, glycogen synthesis and lipid and cholesterol metabolism. The effects of testosterone differ in the major tissues involved in insulin action, which include liver, muscle and fat, suggesting a complex regulatory influence on metabolism. -

Gender-Affirming Hormone Therapy
GENDER-AFFIRMING HORMONE THERAPY Julie Thompson, PA-C Medical Director of Trans Health, Fenway Health March 2020 fenwayhealth.org GOALS AND OBJECTIVES 1. Review process of initiating hormone therapy through the informed consent model 2. Provide an overview of masculinizing and feminizing hormone therapy 3. Review realistic expectations and benefits of hormone therapy vs their associated risks 4. Discuss recommendations for monitoring fenwayhealth.org PROTOCOLS AND STANDARDS OF CARE fenwayhealth.org WPATH STANDARDS OF CARE, 2011 The criteria for hormone therapy are as follows: 1. Well-documented, persistent (at least 6mo) gender dysphoria 2. Capacity to make a fully informed decision and to consent for treatment 3. Age of majority in a given country 4. If significant medical or mental health concerns are present, they must be reasonably well controlled fenwayhealth.org INFORMED CONSENT MODEL ▪ Requires healthcare provider to ▪ Effectively communicate benefits, risks and alternatives of treatment to patient ▪ Assess that the patient is able to understand and consent to the treatment ▪ Informed consent model does not preclude mental health care! ▪ Recognizes that prescribing decision ultimately rests with clinical judgment of provider working together with the patient ▪ Recognizes patient autonomy and empowers self-agency ▪ Decreases barriers to medically necessary care fenwayhealth.org INITIAL VISITS ▪ Review history of gender experience and patient’s goals ▪ Document prior hormone use ▪ Assess appropriateness for gender affirming medical -

EFFECTS of FEMINIZING HORMONE THERAPY (ESTROGEN) Effects in RED Are Permanent Changes
EFFECTS OF FEMINIZING HORMONE THERAPY (ESTROGEN) Effects in RED are permanent changes. Effect First noticeable: Maximum effect: Breast enlargement 3-6 months 2-3 years Softening of skin, less 3-6 months Unknown oily skin Slower, thinner growth 6-12 months 3 years or more of facial and body hair Decrease in male Hair loss stops in 1-3 1-2 years pattern baldness months but hair does not grow back Decreased muscle mass 3-6 months 1-2 years / strength Body fat redistribution 3-6 months 2-5 years (more fat on buttocks, hips, thighs, face) Decreased libido (sex 1-3 months 1-2 years drive) Decreased spontaneous 1-3 months 3-6 months erections Decreased volume 3-6 months 2-3 years (shrinking) of the testes Decreased sperm Variable Variable production/Infertility What are the emotional and intellectual effects of estrogen? People are very different so their emotional and intellectual changes vary widely. People taking estrogen have reported: ● feeling more emotional and more in touch with their feelings ● crying more easily ● mood swings ● depression or sadness ● thinking differently, having different ways of looking at things ● feeling “more like myself” when taking a hormone that aligns with gender identity; feeling more comfortable in one’s body What estrogen does not do: ● change a person’s bone structure ● change a person’s height ● stop the growth of facial hair or eliminate a beard ● cause male pattern balding on the scalp to grow back ● raise the pitch of the voice to a higher level ● provide reliable birth control ● protect against sexually transmitted infections What are the risks of taking estrogen? The major risks are: ● blood clots ― can result in stroke or even death ● gallbladder disease ● liver disease ● weight gain ● high cholesterol which causes heart disease ● high blood pressure EFFECTS OF MASCULINIZING HORMONE THERAPY (TESTOSTERONE) Effects in RED are permanent changes. -

Testosterone Replacement Therapy Initiation and Follow-Up Evaluation in VA Male Patients
Department of Veterans Affairs Office of Inspector General Office of Healthcare Inspections Report No. 15-03215-154 Healthcare Inspection Testosterone Replacement Therapy Initiation and Follow-Up Evaluation in VA Male Patients April 11, 2018 Washington, DC 20420 In addition to general privacy laws that govern release of medical information, disclosure of certain veteran health or other private information may be prohibited by various federal statutes including, but not limited to, 38 U.S.C. §§ 5701, 5705, and 7332, absent an exemption or other specified circumstances. As mandated by law, OIG adheres to privacy and confidentiality laws and regulations protecting veteran health or other private information in this report. Report Suspected Wrongdoing in VA Programs and Operations 1-800-488-8244 www.va.gov/oig VA Office of Inspector General Testosterone Replacement Therapy Initiation and Follow-up Evaluation in VA Male Patients Abbreviations CPG Clinical Practice Guidelines EHR electronic health record FDA Food and Drug Administration FSH follicle-stimulating hormone FY fiscal year LH luteinizing hormone TRT testosterone replacement therapy VHA Veterans Health Administration VA Criteria for Use VA Pharmacy Benefits Management Services, Medical Advisory Panel, and Veterans Integrated Service Network Pharmacist Executives Testosterone Replacement Therapy (TRT) Criteria for Use VA Office of Inspector General Testosterone Replacement Therapy Initiation and Follow-up Evaluation in VA Male Patients Table of Contents Executive Summary .................................................................................................. -

Growth Hormone Improves Nerve Regeneration, Muscle Re
www.nature.com/scientificreports OPEN Growth Hormone Improves Nerve Regeneration, Muscle Re-innervation, and Functional Received: 29 June 2018 Accepted: 17 January 2019 Outcomes After Chronic Published: xx xx xxxx Denervation Injury Joseph Lopez1, Amy Quan1, Joshua Budihardjo1, Sinan Xiang1, Howard Wang1, Kiron Koshy1, Christopher Cashman 2, W. P. Andrew Lee1, Ahmet Hoke 2, Sami Tufaha1 & Gerald Brandacher1 This study investigates the efcacy of systemic growth hormone (GH) therapy in ameliorating the deleterious efects of chronic denervation (CD) injury on nerve regeneration and resulting motor function. Using a forelimb CD model, 4 groups of Lewis rats were examined (n = 8 per group): Group-1 (negative control) 8 weeks of median nerve CD followed by ulnar-to-median nerve transfer; Group-2 (experimental) 8 weeks of median nerve CD followed by ulnar-to-median nerve transfer and highly purifed lyophilized pituitary porcine GH treatment (0.6 mg/day); Group-3 (positive control) immediate ulnar-to-median nerve transfer without CD; Group-4 (baseline) naïve controls. All animals underwent weekly grip strength testing and were sacrifced 14 weeks following nerve transfer for histomorphometric analysis of median nerve regeneration, fexor digitorum superfcialis atrophy, and neuromuscular junction reinnervation. In comparison to untreated controls, GH-treated animals demonstrated enhanced median nerve regeneration as measured by axon density (p < 0.005), axon diameter (p < 0.0001), and myelin thickness (p < 0.0001); improved muscle re-innervation (27.9% vs 38.0% NMJs re-innervated; p < 0.02); reduced muscle atrophy (1146 ± 93.19 µm2 vs 865.2 ± 48.33 µm2; p < 0.02); and greater recovery of motor function (grip strength: p < 0.001).