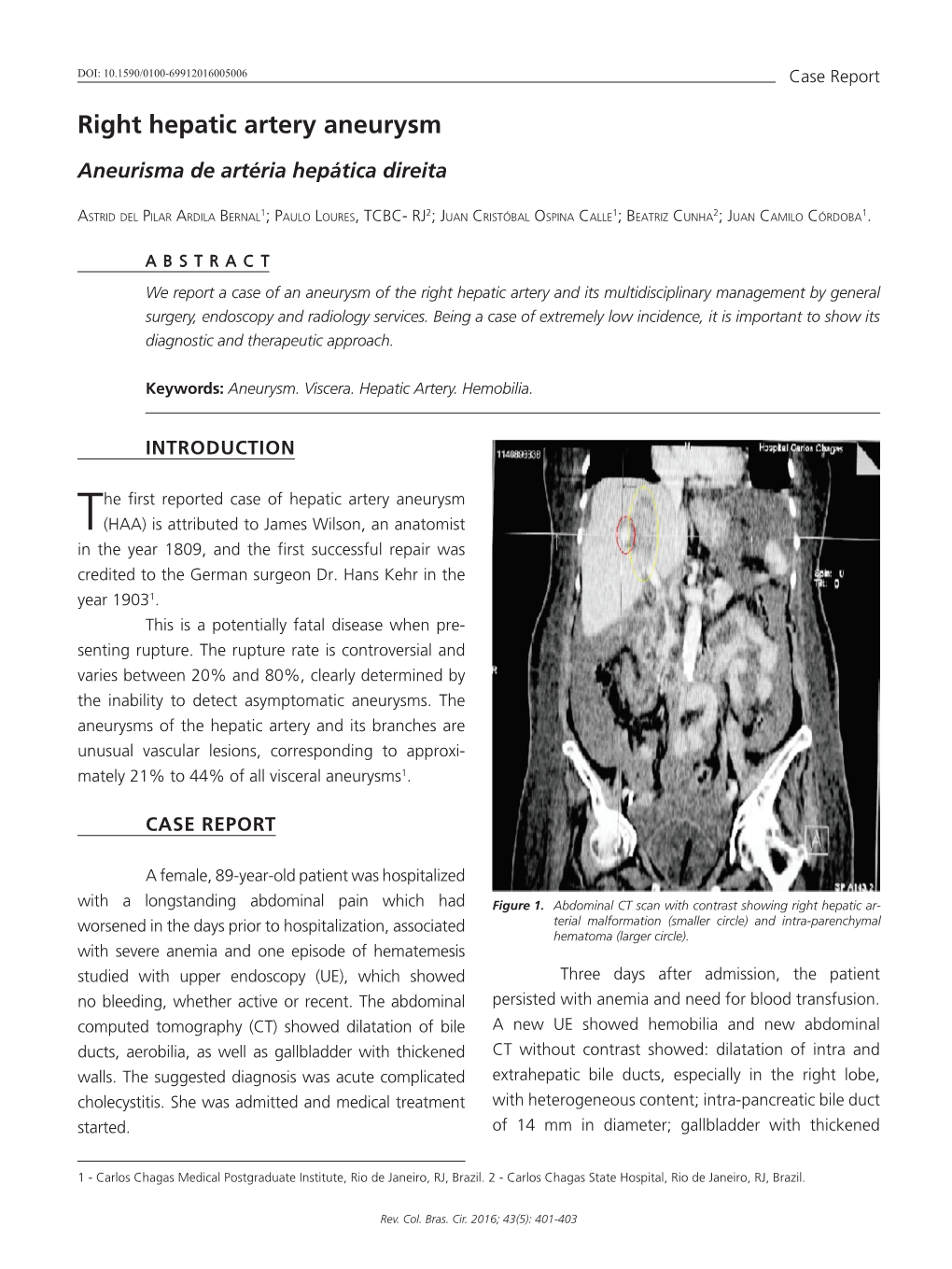
Right Hepatic Artery Aneurysm
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Intraperitoneal Haemorrhagefrom Anterior Abdominal
490 CLINICAL REPORTS Postgrad Med J: first published as 10.1136/pgmj.69.812.490 on 1 June 1993. Downloaded from Postgrad Med J (1993) 69, 490-493 © The Fellowship of Postgraduate Medicine, 1993 Intraperitoneal haemorrhage from anterior abdominal wall varices J.B. Hunt, M. Appleyard, M. Thursz, P.D. Carey', P.J. Guillou' and H.C. Thomas Departments ofMedicine and 1Surgery, St Mary's Hospital Medical School, Imperial College, London W2 INY, UK Summary: Patients with oesophageal varices frequently present with gastrointestinal haemorrhage but bleeding from varices at other sites is rare. We present a patient with hepatitis C-induced cirrhosis and partial portal vein occlusion who developed spontaneous haemorrhage from anterior abdominal wall varices into the rectus abdominus muscle and peritoneal cavity. Introduction Portal hypertension is most often seen in patients abdominal pain of sudden onset. Over the pre- with chronic liver disease but may also occur in ceding 3 months he had noticed abdominal and those with portal vein occlusion. Thrombosis ofthe ankle Four years earlier chronic active swelling. by copyright. portal vein is recognized in both cirrhotic patients,' hepatitis had been diagnosed in Egypt and treated those with previous abdominal surgery, sepsis, with prednisolone and azathioprine. neoplasia, myeloproliferative disorders,2 protein Examination revealed a well nourished, jaun- C3 or protein S deficiency.4 diced man with stigmata of chronic liver disease Oesophageal varices develop when the portal who was anaemic and shocked with a pulse of pressure is maintained above 12 mmHg.5 Patients 100mm and blood pressure 60/20 mmHg. The with oesophageal varices often present with severe abdomen was distended, diffusely tender and there haematemesis. -

Mimickers of Acute Appendicitis
Appendicitis Mimics, Thompson et al. Mimickers of Acute Appendicitis Joel P. Thompson, M.D., MPH, Dhana Selvaraj, M.D., Refky Nicola, D.O. Department of Imaging Sciences, University of Rochester Medical Center, Rochester, NY Introduction of patients.2,3 The presence of intravenous and enteric contrast aids in identification of the appendix.3 Acute abdominal pain is the most common reason The appendix arises from the cecum inferior to the for an emergency department visit among patients age ileocecal junction (Fig. 1). MDCT signs of acute 15 and older, a large portion of them will complain of 1 appendicitis include appendiceal diameter > 7 mm pain localizing to the right lower quadrant. While with peri-appendiceal stranding of the mesenteric fat appendicitis is the most common cause of the surgical (Fig. 2A).4 Both findings are present in up to 93% of abdomen, a wide variety of acute gastrointestinal, appendicitis cases identified on MDCT.5 The diagnosis genitourinary, and gynecological pathologic processes of appendicitis should not be made using appendiceal can present in similar fashion (Table 1). Acute diameter alone; wall thickening and increased gastrointestinal diseases, such as Crohn’s disease, enhancement should also be present.6 Additional infectious enterocolitis, mesenteric adenitis, cecal findings include the presence of an appendicolith, diverticulitis, Meckel’s diverticulitis, epiploic cecal apical thickening (“arrowhead sign”), mesenteric appendagitis, and omental infarcts can present with adenopathy, fluid in the paracolic gutter, and the right lower quadrant. In addition, acute genitourinary presence of phlegmon.5 A focal wall defect, diseases, such as pyelonephritis and ureterolithiasis, extraluminal air, or presence of an abscess are signs of can present with similar symptoms. -

Hemoperitoneum in Peritoneal Dialysis, a Red Flag? Case Report
Rev. Colomb. Nefrol. 2015; 2(1): 70 -75. http//www.revistanefrologia.org Rev. Colomb.Case Nefrol. report 2015; 2(1): 70 - 75 http//doi.org/10.22265/acnef.2.1.200 Hemoperitoneum in peritoneal dialysis, a red flag? Case report. Sylvia Quiñones Sussman1, Carolina Larrarte Arenas1, Freddy Ardila Celis2 1 Department, Unit missing, RTS-Agencia Santa Clara, Bogotá, Colombia. 2 Department, Unit missing, Clinical Development RTS / Baxter Colombia. Abstract Hemoperitoneum is a complication of peritoneal dialysis. Its differential diagnosis is broad and the approach is based on its clinical manifestation and severity. It is important to evaluate all the causes of hemoperito- neum and to consider that it may be life risking. This is a case of a patient on long term peritoneal dialysis with hemoperitoneum, whose study showed calcifying peritonitis as the underlying condition. Key words: hemoperitoneum, peritoneal dialysis, calcifying peritonitis, sclerosing encapsulating peritonitis. ¿Hemoperitoneo en diálisis peritoneal, un signo de alarma? Resumen El hemoperitoneo es una complicación de la diálisis peritoneal. Su diagnóstico diferencial es amplio y el enfoque se basa en el cuadro clínico y su severidad. Es necesario evaluar todas las causas del hemoperitoneo y tener en cuenta que tienen manifestaciones diferentes y que algunas arriesgan la vida del paciente. A con- tinuación se describe un caso de un paciente con largo tiempo en diálisis peritoneal con hemoperitoneo, en quien el estudio sugiere peritonitis calcificante como enfermedad de base. Palabras -

Peritoneal Sclerosis and Massive Hemoperitoneum: Case Report and Short Review
Urology & Nephrology Open Access Journal Case Report Open Access Peritoneal sclerosis and massive hemoperitoneum: case report and short review Abstract Volume 7 Issue 3 - 2019 Secondary Peritoneal Sclerosis has been reported in several cases but is especially frequent Daniel Gonzalez Nunez, Jhordan Guzman, among chronic peritoneal dialysis users, being its most serious complication. Clinical suspicion in chronic PD users is no challenge as intestinal symptoms and hypoalbuminemia Felipe Matteus Acuna, Juan Guillermo Ramos, appear and radiological confirmation is usually achieved before the need for surgery and Juliana Ordonez intra abdominal findings prove confirmatory. A case report of a 37-year-old male patient Department of Surgery, Hospital Universitario Clinica San Rafael, Universidad Militar Nueva Granada, Bogota, Colombia with a 13 year long peritoneal dialysis in whom laparotomy findings were a massive hemoperitoneum, parietal/visceral peritoneum, small/large bowel and mesentery with Correspondence: Daniel Gonzalez Nunez, Department of chronic inflammatory changes, thickening and dark-brown coloration. As a distinctive Surgery, Hospital Universitario Clinica San Rafael, Universidad feature a gastroepiploic artery branch in the gastric curvature was identified with persistent Militar Nueva Granada, Bogota, Colombia, Tel +5713108667653, oozing and hemostasis was achieved. No intestinal obstruction was evident. Postoperative Email was uneventful. In patients undergoing peritoneal dialysis a hemorrhagic effluent from the catheter or -

Spontaneous Hemoperitoneum, Due to Bleeding from Retroperitoneal Varices, in a Cirrhotic Patient
CASE REPORT Spontaneous hemoperitoneum, due to bleeding from retroperitoneal varices, in a cirrhotic patient: a case report Ahmad Abutaka1, Renol Mathew Koshy1, Abdulrahman Abu Sabeib1, Adriana Toro2 & Isidoro Di Carlo1,3 1Department of General Surgery, Hamad General Hospital, Al Rayyan Road, 3050, Doha Qatar 2Department of Surgery, Barone Romeo Hospital, via Mazzini 14, 98066 Patti, Italy 3Department of Surgical Sciences and Advanced Technologies “G.F. Ingrassia”, University of Catania, via Santa Sofia 78, 95100 Catania, Italy Correspondence Key Clinical Message Renol Mathew Koshy, Department of General Surgery, Hamad General Hospital, Al Hemoperitoneum from retroperitoneal varices in cirrhotic is very rare. This Rayyan Road, 3050 Doha, Qatar. condition should be taken into account based on anamnesis, clinical features, Tel: +974 55748825; and laboratory findings; but due to the unstable presentation, diagnosis remains E-mail: [email protected] a challenge. Emergency laparotomy could be effective treatment, but the prog- nosis remains poor related to the hepatic reserve. Funding Information No sources of funding were declared for this study. Keywords Cirrhosis, hemoperitoneum, hemorrhagic shock, portal hypertension, varices. Received: 26 July 2015; Revised: 26 August 2015; Accepted: 28 September 2015 Clinical Case Reports 2016; 4(1): 51–53 doi: 10.1002/ccr3.427 Introduction his body had a strong smell of alcohol. The patient was intubated and ventilated. His abdomen was found to be Spontaneous hemoperitoneum is a rare and catastrophic distended and tense, with an everted umbilicus; his bowel complication of portal hypertension [1], mainly affecting sounds were negative and a digital rectal examination patients with liver cirrhosis. Rupture of retroperitoneal showed no blood or masses. -

Spontaneous Hemoperitoneum from a Ruptured Gastrointestinal Stromal Tumor
Open Access Case Report DOI: 10.7759/cureus.9338 Spontaneous Hemoperitoneum From a Ruptured Gastrointestinal Stromal Tumor Jordan Shively 1 , Charles Ebersbacher 2 , William T. Walsh 1 , Matthew T. Allemang 1 1. General Surgery, Cleveland Clinic South Pointe Hospital, Warrensville Heights, USA 2. General Surgery, Ohio University Heritage College of Osteopathic Medicine, Warrensville Heights, USA Corresponding author: Jordan Shively, [email protected] Abstract This is a case report of a ruptured gastrointestinal stromal tumor (GIST) presenting as spontaneous hemoperitoneum. The patient was a 63-year-old female with a past medical history of hypertension and ulcerative colitis who presented to the emergency department with worsening epigastric pain. The patient denied history of trauma, previous surgeries, or forceful vomiting. She was not on anticoagulation. Vital signs at presentation were stable. A CT scan of abdomen/pelvis revealed a large amount of fluid in the upper abdomen with high attenuation material adjacent to the greater curvature of the stomach concerning for hemoperitoneum. Diagnostic laparoscopy revealed a significant amount of blood along the upper abdominal viscera. The procedure was converted to an upper midline laparotomy after identifying a necrotic, extremely friable 7 x 6 x 3 cm pedunculated mass with active hemorrhage on the posterior aspect of the greater curvature. A wedge resection was performed to remove the mass with grossly negative margins. An intraoperative frozen section revealed a stromal tumor with spindle cells. Final pathology revealed a pT3N0M0 stromal tumor with histologic spindle cells and a high mitotic rate (24/5 mm2) consistent with a high-grade GIST. Given tumor rupture at presentation, the patient was started on imatinib therapy for a minimum duration of three years. -

Spontaneous Hemoperitoneum in Sigmoid Diverticular Disease
ACS Case Reviews in Surgery Vol. 2, No. 5 Spontaneous Hemoperitoneum in Sigmoid Diverticular Disease AUTHORS: CORRESPONDENCE AUTHOR: Sukhmine Nedopil, MD; Sukhmine Nedopil, MD Shahin Foroutan, MD, FACS Department of Surgery 500 West Hospital Rd French Camp, CA 95231 Email: [email protected] Phone: 916-835-5368 Background A 52-year-old man presented with acute abdominal pain and hemoperitoneum. Summary Intraperitoneal hemorrhage from colonic diverticulum is rare. We report a case of a 52-year-old man with hemoperitoneum diagnosed by computed tomography scan of the abdomen and pelvis with intravenous contrast. Postoperative histopathological findings revealed the cause of hemoperitoneum as erosion of sigmoid diverticulum into a serosal vessel. This subsequently caused the vessel to bleed intraperitoneally. The operation included sigmoid resection and temporary colostomy placement. Postoperative colonoscopy did not find any dysplastic pathology in the rectal stump or colon. Patient was anastomosed three months later. Conclusion Diverticular disease has a spectrum of presentation. Hemorrhage from diverticular disease is more commonly intraluminal presenting with lower gastrointestinal bleed. We present a case of extraluminal hemorrhage in diverticular disease. This highlights a rare but potentially life-threatening complication of colonic diverticular disease. Keywords hemoperitoneum, diverticulum, sigmoid colon, bleeding DISCLOSURE STATEMENT: The authors have no conflicts of interest to disclose. To Cite: Nedopil S, Foroutan S. Spontaneous Hemoperitoneum in Sigmoid Diverticular Disease. ACS Case Reviews in Surgery. 2020;2(5):48–51. American College of Surgeons – 48 – ACS Case Reviews. 2020;2(5):48-51 ACS Case Reviews in Surgery Nedopil S, Foroutan S Case Description A 52-year-old man presented to the emergency department with severe abdominal pain that progressed over three days associated with nausea and chills. -

Endometriosis and Perinatal Outcome – a Systematic Review of the Literature
Current Women’s Health Reviews, 2012, 8, 121-130 121 Endometriosis and Perinatal Outcome – A Systematic Review of the Literature Sevasti Masouridou*, Apostolos Mamopoulos, Georgios Mavromatidis and Vassilios Karagiannis 3rd University Department Obstetrics & Gynaecology, Aristotle University of Thessaloniki, Medical School, 546 22 Thessaloniki, Greece Abstract: Objective: To assess any possible adverse effects of endometriosis on pregnancy outcome and complications, as well as in the postpartum period. Study Design: A systematic review of the literature. Data Sources: We searched all publications in Pubmed, Scopus and the Cochrane Library with the key words endometriosis, pregnancy outcome, preeclampsia, preterm birth, small-for gestational age babies (SGA) and postpartum. Eligibility Criteria for Selecting Studies: All studies reporting on endometriosis and perinatal outcome until December 2009. Results: According to the available bibliographic data, we found 38 reported cases of pregnancies, four being twin pregnancies, complicated by endometriosis (Table 1). Studies referring to specific pregnancy complications (preterm birth, small-for-gestational age babies, preeclampsia and postpartum complications) were limited to a total of 12 publications [61-63, 69, 75, 80, 82-86]. The few reported complications during pregnancy included hemoperitoneum and spontaneous bleeding [1, 9-21], perforations of the jejunum, appendix and sigmoid colon [22-24], urohemoperitoneum [25], deciduosis of the appendix [26], deciduosis of the omentum [27], infected endometrioma [28], hemoperitoneum and hemothorax [29], catamenial pneumothorax [30], endometriosis imitating a bladder tumor [31], decidualization mimicking ovarian malignancy [32], rupture of ovarian endometriotic cyst [23, 33], and rupture of the uterus affected by endometriosis [34] (Table 1). Data regarding the effect of endometriosis on preterm birth, small-for gestational age babies and preeclampsia, both in spontaneous pregnancies as well as in those conceived by Assisted Reproductive Techniques (ART) were conflicting. -

Ruptured Hepatocellular Carcinoma in a Child with Budd-Chiari Syndrome
C A S E R E P O R T Ruptured Hepatocellular Carcinoma in a Child with Budd-Chiari Syndrome ANANDINI SURI, VARUN K SHARMA, PRAJAKTA R RANADE, #SHAJI MARAR AND *AABHA NAGRAL From Departments of Pediatrics, #Interventional Radiology and *Gastroenterology, Jaslok hospital and Research Centre, Mumbai, India. Correspondence to: Dr Aabha Nagral, Background: Hepatocellular carcinoma is an uncommon complication described in 7, Snehasagar, Prabhanagar, Prabhadevi, patients with Budd-Chiari syndrome. Case characteristics: A 12-year-old boy with Budd- Mumbai 400 025, India. Chiari syndrome, who was earlier treated with Transjugular intrahepatic porto-systemic [email protected]. shunt (TIPS), presented with acute onset hemoperitoneum and hypotension. Outcome: It Received: August 04, 2015; was diagnosed to be a case of ruptured hepatocellular carcinoma. Message: Successful Initial review: October 20, 2015; Accepted: TIPS may not prevent the development of hepatocellular carcinoma, and children with Budd July 09, 2016. Chiari syndrome should be monitored for the same. Keywords: Complication, Hemoperitoneum, Liver tumor, TIPS. udd-Chiari Syndrome (BCS) is a progressive response, but after 6 months developed stent occlusion. disease leading to portal hypertension, liver He underwent TIPS procedure with 10 mm × 60 mm dysfunction, hepatopulmonary syndrome, GORE VIATORR stent. The portosystemic gradient Band cirrhosis. Hepatocellular carcinoma reduced from 28 mmHg to 3 mmHg. There were no (HCC) is a rare but potential complication of BCS. It has immediate complications. On follow-up, ascites subsided been reported in few adult patients despite undergoing and weight improved (from <5th centile to 25th centile). radiological intervention like Transjugular Intrahepatic He had no further variceal bleeds. -
Two Cases of Gastrointestinal Stromal Tumour Presenting Uncommonly As
Hong Kong J Radiol. 2016;19:132-6 | DOI: 10.12809/hkjr1615376 CASE REPORT Two Cases of Gastrointestinal Stromal Tumour Presenting Uncommonly as Intraperitoneal Rupture in Patients Prescribed Warfarin RCH Nung1, SSM Wong1, RKL Lee1, ABW Chan2, YYP Lee1 Departments of 1Imaging and Interventional Radiology, and 2Anatomical and Cellular Pathology, Prince of Wales Hospital, Shatin, Hong Kong ABSTRACT Gastrointestinal stromal tumour (GIST) is the most common mesenchymal neoplasm of the gastrointestinal tract. Common presentations of GIST include early satiety, indigestion, bloating, vague abdominal pain, and gastrointestinal bleeding. Intraperitoneal rupture is an uncommon presentation of GIST. We have encountered two patients prescribed warfarin, who presented with intraperitoneal haemorrhage as their initial presentation of gastric GIST. Computed tomography (CT) revealed a submucosal gastric mass with intralesional and intraperitoneal haemorrhage. The diagnosis of ruptured GIST was made based on CT findings. These two cases are, to the best of our knowledge, the first two cases with rupture and intraperitoneal haemorrhage as the initial presentation of gastric GIST while on warfarin. Key Words: Gastrointestinal stromal tumors; Hemorrhage; Rupture; Warfarin 中文摘要 服用華法林患者出現罕見的胃腸道間質瘤腹腔內破裂後被確診為 胃腸道間質瘤:兩例報告 農智行、王先民、李嘉樂、陳碧雲、李艷萍 胃腸道間質瘤(GIST)是胃腸道最常見的間質腫瘤。GIST的常見症狀包括易飽、消化不良、腹脹、 腹部疼痛和消化道出血。腹腔內破裂是GIST的一種罕見的症狀。本文報告兩名服食華法林的GIST 病人出現腹腔內破裂。CT顯示粘膜下胃腫塊及病變內和腹腔出血。後因CT檢查結果而被確診為 GIST。據我們所知,這兩個為首個類似的病例。 INTRODUCTION (GI) tract and commonly presents after 50 years of age. Gastrointestinal stromal tumour (GIST) is the most It arises from the muscularis propria and expresses common mesenchymal neoplasm of the gastrointestinal transmembrane receptor tyrosine kinase encoded by Correspondence: Dr Ryan Nung, Department of Imaging and Interventional Radiology, Prince of Wales Hospital, Shatin, Hong Kong. Tel: (852) 2632 1248; Email: [email protected] Submitted: 9 Nov 2015; Accepted: 26 Nov 2015. -

Nonoperative Management of Blunt Hepatic Injury: an Eastern Association for the Surgery of Trauma Practice Management Guideline
GUIDELINE Nonoperative management of blunt hepatic injury: An Eastern Association for the Surgery of Trauma practice management guideline Nicole A. Stassen, MD, Indermeet Bhullar, MD, Julius D. Cheng, MD, Marie Crandall, MD, Randall Friese, MD, Oscar Guillamondegui, MD, Randeep Jawa, MD, Adrian Maung, MD, Thomas J. Rohs, Jr, MD, Ayodele Sangosanya, MD, Kevin Schuster, MD, Mark Seamon, MD, Kathryn M. Tchorz, MD, Ben L. Zarzuar, MD, and Andrew Kerwin, MD BACKGROUND: During the last century, the management of blunt force trauma to the liver has changed from observation and expectant management in the early part of the 1900s to mainly operative intervention, to the current practice of selective operative and nonoperative management. These issues were first addressed by the Eastern Association for the Surgery of Trauma in the Practice Management Guidelines for Nonoperative Management of Blunt Injury to the Liver and Spleen published online in 2003. Since that time, a large volume of literature on these topics has been published requiring a reevaluation of the previous Eastern Association for the Surgery of Trauma guideline. METHODS: The National Library of Medicine and the National Institutes of Health MEDLINE database were searched using PubMed (www.pubmed.gov). The search was designed to identify English-language citations published after 1996 (the last year included in the previous guideline) using the keywords liver injury and blunt abdominal trauma. RESULTS: One hundred seventy-six articles were reviewed, of which 94 were used to create the current practice management guideline for the selective nonoperative management of blunt hepatic injury. CONCLUSION: Most original hepatic guidelines remained valid and were incorporated into the greatly expanded current guidelines as appropriate. -

A Complication of Paracentesis Due to Hyperfibrinolysis: Hemoperitoneum
isord D ers od & lo T r B f a n o s l f a u n s r Journal of i o u n o Smith et al., J Blood Disorders Transf 2013, S:3 J ISSN: 2155-9864 Blood Disorders & Transfusion DOI: 10.4172/2155-9864.S3-005 Case Report OpenOpen Access Access A Complication of Paracentesis Due to Hyperfibrinolysis: Hemoperitoneum Elliot Smith1, Stephen H Caldwell2 and Neeral L Shah2* 1Department of Medicine, University of Virginia, Charlottesville, VA, USA 2Division of Gastroenterology and Hepatology, University of Virginia, Charlottesville, VA, USA Abstract Paracentesis is a commonly performed procedure associated with minimal risk of complication. We report a case of a cirrhotic patient who developed hemoperitoneum after paracentesis. This adverse outcome was attributed to a state of hypefibrinolysis. We describe a patient with end stage liver disease and ascites who developed a severe bleeding complication from a large volume paracentesis. Five days after the paracentesis, the patient developed a large abdominal wall hematoma. The patient was treated with a course of systemic epsilon- aminocaproic acid and the bleeding resolved. Hyperfibrinolysis is the phenomenon of excessive clot breakdown and has been noted to increase the risk of procedural complications. The diagnosis of hyperfibrinolysis is clinically determined and therefore is often overlooked. This case demonstrates the need for increased recognition of this entity to ensure rapid and proper treatment of hyperfibrinolysis with anti-fibrinolytics. Keywords: Paracentesis; Hemoperitoneum; Hyperfibrinolysis leading to transfusion of 2 units of packed red blood cells. A CT scan was performed and localized the hematoma to the subcutaneous tissue Introduction without involvement of the peritoneal cavity (Figure 2).