Costochondritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treatment of a Female Collegiate Rower with Costochondritis: a Case Report
Treatment of a female collegiate rower with costochondritis: a case report Terry L. Grindstaff 1, James R. Beazell2, Ethan N. Saliba1, Christopher D. Ingersoll3 1Curry School of Education and Department of Athletics, University of Virginia, USA, 2University of Virginia- HEALTHSOUTH, USA, 3Central Michigan University, USA Rib injuries are common in collegiate rowing. The purpose of this case report is to provide insight into examination, evaluation, and treatment of persistent costochondritis in an elite athlete as well as propose an explanation for chronic dysfunction. The case involved a 21 year old female collegiate rower with multiple episodes of costochondritis over a 1-year period of time. Symptoms were localized to the left third costosternal junction and bilaterally at the fourth costosternal junction with moderate swelling. Initial interventions were directed at the costosternal joint, but only mild, temporary relief of symptoms was attained. Reexamination findings included hypomobility of the upper thoracic spine, costovertebral joints, and lateral ribs. Interventions included postural exercises and manual therapies directed at the lateral and posterior rib structures to improve rib and thoracic spine mobility. Over a 3-week time period pain experienced throughout the day had subsided (visual analog scale – VAS 0/10). She was able to resume running and elliptical aerobic training with minimal discomfort (VAS 2/10) and began to reintegrate into collegiate rowing. Examination of the lateral ribs, cervical and thoracic spine should be part of the comprehensive evaluation of costochondritis. Addressing posterior hypomobility may have allowed for a more thorough recovery in this case study. Keywords: Costochondritis, Joint mobilization, Rib, Thoracic spine Chest and rib injuries have a high prevalence (26%) self-limiting condition2 allowing individuals to among female rowers.1–3 Pain which is localized to continue athletic participation as symptoms allow. -

Part 1 the Thorax ECA1 7/18/06 6:30 PM Page 2 ECA1 7/18/06 6:30 PM Page 3
ECA1 7/18/06 6:30 PM Page 1 Part 1 The Thorax ECA1 7/18/06 6:30 PM Page 2 ECA1 7/18/06 6:30 PM Page 3 Surface anatomy and surface markings The experienced clinician spends much of his working life relating the surface anatomy of his patients to their deep structures (Fig. 1; see also Figs. 11 and 22). The following bony prominences can usually be palpated in the living subject (corresponding vertebral levels are given in brackets): •◊◊superior angle of the scapula (T2); •◊◊upper border of the manubrium sterni, the suprasternal notch (T2/3); •◊◊spine of the scapula (T3); •◊◊sternal angle (of Louis) — the transverse ridge at the manubrio-sternal junction (T4/5); •◊◊inferior angle of scapula (T8); •◊◊xiphisternal joint (T9); •◊◊lowest part of costal margin—10th rib (the subcostal line passes through L3). Note from Fig. 1 that the manubrium corresponds to the 3rd and 4th thoracic vertebrae and overlies the aortic arch, and that the sternum corre- sponds to the 5th to 8th vertebrae and neatly overlies the heart. Since the 1st and 12th ribs are difficult to feel, the ribs should be enu- merated from the 2nd costal cartilage, which articulates with the sternum at the angle of Louis. The spinous processes of all the thoracic vertebrae can be palpated in the midline posteriorly, but it should be remembered that the first spinous process that can be felt is that of C7 (the vertebra prominens). The position of the nipple varies considerably in the female, but in the male it usually lies in the 4th intercostal space about 4in (10cm) from the midline. -

Type of Breathing- Slow, Rapid, Deep, Shal
Primary survey check pulse; type of pulse- slow, rapid, weak, strong check breathing; type of breathing- slow, rapid, deep, shallow maintain open airway; clear blood vomitus check to see that airway is unobstructed help the athlete find the most comfortable posistion for breathing be prepared to prefrom artificial ventilation and CPR if needed transport to emergency facility Secondary seurvey history what happend? What is the mechanism of injury? When did it happen? Have you ever had any injury to this region before? Have you ever been ill or had a recent episode of mononucleosis? Was there a direct blow? If so by what? Where were you hit? Back, chest, or abdominal area? How large was the area of contact? Did you go to the bathroom prior to practice? Where does it hurt? Point to the area of pain how severe is the pain? What kind of do you have? Sharp, dull, achy, throbbing, radiating what increase the pain? What relieves the pain? Have the symptoms been constant or intermittent? Does the pain increase during respiration or movement? Is the pain located in the chest wall or does it feel deeper or inside the cavity? Do you have any referred pain to your shoulders? Kehr’s sign? Do you have any refferred pain to your flanks? Did you feel anything at the time of injury? Did you hear any sounds at the time of injury? Do you have any crepitation? Possible rib fx or costochondral separation do you feel any tightness, cramping, or rigidity of the abdominal musculature? Do you feel nauseaqted? Do you have any difficulty breathing? Have you urinated -

Evaluation of Abdominal Pain in the Emergency Department Hartmut Gross, M.D., FACEP
Evaluation of Abdominal Pain in the Emergency Department Hartmut Gross, M.D., FACEP Abdominal pain complaints comprise about 5% of all Emergency Department visits. The etiology of the pain may be any of a large number of processes. Many of these causes will be benign and self-limited, while others are medical urgencies or even surgical emergencies. As with any complaint in the ED, the worst diagnosis is always entertained first. Therefore, there is one thought, which the ED practitioner must maintain in the foreground of his mind: “Is there a life threatening process?” Etiology A breakdown of the most common diagnoses of abdominal pain presentations is listed below. Note that nearly half of the time, “unknown origin” is the diagnosis made. This is a perfectly acceptable conclusion, after a proper work-up has ruled out any life threatening illness. Common Diagnoses of Non-traumatic Abdominal Pain in the ED 1 Abdominal pain of unknown origin 41.3% 2 Gastroenteritis 6.9% 3 Pelvic Inflammatory Disease 6.7% 4 Urinary Tract Infection 5.2% 5 Ureteral Stone 4.3% 6 Appendicitis 4.3% 7 Acute Cholecystitis 2.5% 8 Intestinal Obstruction 2.5% 9 Constipation 2.3% 10 Duodenal Ulcer 2.0% 11 Dysmenorrhea 1.8% 12 Simple Pregnancy 1.8% 13 Pyelonephritis 1.7% 14 Gastritis 1.4% 15 Other 12.8% From Brewer, RJ., et al, Am J Surg 131: 219, 1976. Two important factors modify the differential diagnosis in patients who present with abdominal pain: sex and age. Other common diagnoses of abdominal pain in men and women are as follows. -

Pain Pathways in Orthopaedic Practice J
Postgrad Med J: first published as 10.1136/pgmj.38.437.157 on 1 March 1962. Downloaded from POSTGRAD. MED. J. (I962), 38, I57 PAIN PATHWAYS IN ORTHOPAEDIC PRACTICE J. D. G. TROUP, M.R.C.S., L.R.C.P.* Aberdeen DESPITE Steindler's (1959) admirable lectures on of which time is one of the most significant, have the subject, pain in orthopiedic practice remains a to obtain before pain can be appreciated in tissues difficult problem. To some extent the difficulty is remote from a primary lesion, and when the pain is exaggerated by the adoption of diagnoses based on present, so too are palpably pathological changes. pathological processes which are insusceptible of It is probably true that a peripheral pathway for proof-diagnoses for which it is impossible to pain can be excited centrally or by any stimulus establish an association between symptoms and proximal to it, but the pathway cannot be estab- their alleged origin, let alone a direct causal link. lished in the first place without initial pathological For instance a nipped zygapophyseal synovial changes in the periphery. fringe may well cause acute symptoms, but as there is no means of examining the synovia of The Appreciation of Pain zygapophyseal joints, to make this the diagnosis The appreciation of pain is divided into two is purely speculative. Nevertheless pathological parts; first the sensory component-where it is and guesswork of this sort is regrettably common, and what it feels like, and secondly the affective when some of the latest advances in neuro- component which dictates to what extent the pain by copyright. -

96-2314: DOROTHY G. ULRICH and U.S. POSTAL SERVIC
U. S. DEPARTMENT OF LABOR Employees’ Compensation Appeals Board ____________ In the Matter of DOROTHY G. ULRICH and U.S. POSTAL SERVICE, POST OFFICE, Pass Christian, Miss. Docket No. 96-2314; Submitted on the Record; Issued July 17, 1998 ____________ DECISION and ORDER Before MICHAEL J. WALSH, GEORGE E. RIVERS, WILLIE T.C. THOMAS The issue is whether appellant has met her burden of proof in establishing that she sustained osteoarthritis, costochondritis, floating rib syndrome or rib impingement syndrome beginning September 12, 1995 causally related to factors of her federal employment. On December 18, 1995 appellant, then a former part-time flexible distribution clerk, filed an occupational disease claim, alleging that she sustained osteoarthritis, plantar fascitis, costochondritis, floating ribs syndrome, rib impingement syndrome, shoulder arthritis and second degree cystocele and that these conditions were related to her performance of duties as a part-time flexible distribution clerk. Appellant indicated that she first became aware of these conditions in November 1994 and became aware they were work related on January 11, 1995. Appellant was terminated from her position effective September 22, 1995. On February 5, 1996 the employing establishment controverted appellant’s claim, asserting that she had failed to demonstrate a causal relationship between the claimed conditions and factors of her federal employment. In a decision dated June 18, 1996, the Office of Workers’ Compensation Programs accepted appellant’s claim for temporary aggravation of bilateral plantar fascitis and temporary aggravation of shoulder arthritis only. In a decision dated June 19, 1996, the Office reiterated the accepted conditions and found that appellant had not established that the claimed conditions of osteoarthritis in the legs, arms, wrists and hips, costochondritis, floating rib syndrome or rib impingement syndrome were related to or aggravated by her federal employment. -
Pseudoanginal Chest Pain Associated with Vagal Nerve Stimulation: a Case Report James B
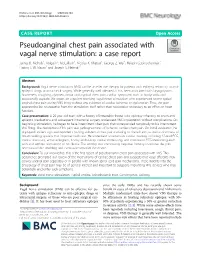
Nichols et al. BMC Neurology (2020) 20:144 https://doi.org/10.1186/s12883-020-01693-5 CASE REPORT Open Access Pseudoanginal chest pain associated with vagal nerve stimulation: a case report James B. Nichols1, Abigail P. McCallum1, Nicolas K. Khattar1, George Z. Wei1, Rakesh Gopinathannair2, Haring J. W. Nauta1 and Joseph S. Neimat1* Abstract Background: Vagal nerve stimulation (VNS) can be an effective therapy for patients with epilepsy refractory to anti- epileptic drugs or intracranial surgery. While generally well tolerated, it has been associated with laryngospasm, hoarseness, coughing, dyspnea, throat and atypical chest pain, cardiac symptoms such as bradycardia and occasionally asystole. We report on a patient receiving vagal nerve stimulation who experienced severe typical anginal chest pain during VNS firing without any evidence of cardiac ischemia or dysfunction. Thus, the pain appeared to be neuropathic from the stimulation itself rather than nociceptive secondary to an effect on heart function. Case presentation: A 29-year-old man, with a history of intractable frontal lobe epilepsy refractory to seven anti- epileptic medications and subsequent intracranial surgery, underwent VNS implantation without complications. On beginning stimulation, he began to have intermittent chest pain that corresponded temporally to his intermittent VNS firing. The description of his pain was pathognomonic of ischemic cardiac chest pain. On initial evaluation, he displayed Levine’s sign and reported crushing substernal chest pain radiating to the left arm, as well as shortness of breath walking upstairs that improved with rest. He underwent an extensive cardiac workup, including 12-lead ECG, cardiac stress test, echocardiogram, 12-day ambulatory cardiac monitoring, and continuous ECG monitoring each with and without stimulation of his device. -

Surgical Treatment of Angina Pectoris He Extensive
SURGICAL TREATMENT OF ANGINA PECTORIS INGA LINDGREN, M.D., AND HERBERT OLIVECRONA, M.D. Neurosurgical Clinic, Serafimerlasarettet, (Director: Professor H. Olivecrona) and IVth Medical Service, St. Erik's Hospital (Director: Professor H. Berglund), Stockholm, Sweden (Received for publication October ~3, 1946) HE EXTENSIVE researches of Blumgart I have shown that the structural basis for coronary pain is an arteriosclerotic process with obstruction T or obliteration of one or more coronary arteries before an adequate collateral circulation has been developed. On the other hand, if the develop- ment of the collateral circulation has kept pace with the progressive arterial narrowing, myocardial damage and pain are absent even if one or more of the coronary arteries are obstructed. If the increased blood supply to the myocardium demanded by muscu- lar exercise cannot be delivered through the ordinary or collateral channels, coronary pain results. A short rest is usually sufficient to restore the circula- tory balance and the pain subsides. Dilatation of the coronary arteries by nitroglycerine hastens the process and may, if the drug is taken before muscular exertion, prevent an anticipated attack. Vasoconstriction, on the other hand, is an important factor in anginal pain. Practically every sufferer from angina pectoris is worse in the winter; his capacity for muscular work is much less in cold weather. Sudden cooling from any cause is frequently sufficient to bring on an attack. Freedberg, 7 in a series of experiments, has been able to show the effect of cooling upon the exercise tolerance in angina pectoris. He found by testing the same patient's capacity for exercise at different temperatures that the tolerance was much less at temperatures of 7-13~ (45-55~ than at ~4~ (75~ His in- vestigations thus lend experimental support to clinical experience that cold weather has a bad effect on sufferers from angina pectoris. -
Skeleton of the Spine and the Thorax
SKELETON OF THE SPINE AND THE THORAX Pages 37- 42 and 54 - 57 Skeleton of the spine Vertebral Column . forms the basic structure of the trunk . consists of 33-34 vertebrae and intervertebral discs . 7 cervical, 12 thoracic, 5 lumbar = true vertebrae . sacrum and coccyx fused = false vertebrae Vertebra . all vertebrae have certain features in common (vertebral body, vertebral arch and seven processes) and regional differences . vertebral body . vetrebral arch pedicle lamina spinous process transverse process articular processes . vertebral foramen . vetrebral notch Cervical vertebrae . transverse foramen (foramen transversarium) in the transverse process . transverse processes of cervical vertebrae end laterally in two projection for attachment of cervical muscles anterior tubercle and posterior tubercle . bifid spinous process . C6 - tuberculum caroticum . C7 - vertebra prominens Atlas C1 . a ring-shaped bone . has neither a boby nor a spinous process . lateral masses . anterior and posterior arches . anterior and posterior tubercles . superior and inferior articular surfaces . articular facet for dens Axis C2 . serves as the pivot about which the rotation of the head occurs . odontoid process = dens . anterior articular facet Thoracic vertebrae . spinous process is long and running posteroinferiorly . superior costal facet . inferior costal facet . transverse process has an articulating facet for the tubercle of a rib = costal facet . the body is heart-shaped Lumbar vertebrae . massive bodies . accessory process - on the posterior surface of the base of each transverse process . mammilary process - on the posterior surface of the superior articular process . costal process Sacrum solid triangular bone . base . wings (alae) . apex . dorsal surface median crest intermediate crest lateral crest posterior sacral foramina superior art. processes . -

1 the Thoracic Wall I
AAA_C01 12/13/05 10:29 Page 8 1 The thoracic wall I Thoracic outlet (inlet) First rib Clavicle Suprasternal notch Manubrium 5 Third rib 1 2 Body of sternum Intercostal 4 space Xiphisternum Scalenus anterior Brachial Cervical Costal cartilage plexus rib Costal margin 3 Subclavian 1 Costochondral joint Floating ribs artery 2 Sternocostal joint Fig.1.3 3 Interchondral joint Bilateral cervical ribs. 4 Xiphisternal joint 5 Manubriosternal joint On the right side the brachial plexus (angle of Louis) is shown arching over the rib and stretching its lowest trunk Fig.1.1 The thoracic cage. The outlet (inlet) of the thorax is outlined Transverse process with facet for rib tubercle Demifacet for head of rib Head Neck Costovertebral T5 joint T6 Facet for Tubercle vertebral body Costotransverse joint Sternocostal joint Shaft 6th Angle rib Costochondral Subcostal groove joint Fig.1.2 Fig.1.4 A typical rib Joints of the thoracic cage 8 The thorax The thoracic wall I AAA_C01 12/13/05 10:29 Page 9 The thoracic cage Costal cartilages The thoracic cage is formed by the sternum and costal cartilages These are bars of hyaline cartilage which connect the upper in front, the vertebral column behind and the ribs and intercostal seven ribs directly to the sternum and the 8th, 9th and 10th ribs spaces laterally. to the cartilage immediately above. It is separated from the abdominal cavity by the diaphragm and communicates superiorly with the root of the neck through Joints of the thoracic cage (Figs 1.1 and 1.4) the thoracic inlet (Fig. -

Abdominal Pain
10 Abdominal Pain Adrian Miranda Acute abdominal pain is usually a self-limiting, benign condition that irritation, and lateralizes to one of four quadrants. Because of the is commonly caused by gastroenteritis, constipation, or a viral illness. relative localization of the noxious stimulation to the underlying The challenge is to identify children who require immediate evaluation peritoneum and the more anatomically specific and unilateral inner- for potentially life-threatening conditions. Chronic abdominal pain is vation (peripheral-nonautonomic nerves) of the peritoneum, it is also a common complaint in pediatric practices, as it comprises 2-4% usually easier to identify the precise anatomic location that is produc- of pediatric visits. At least 20% of children seek attention for chronic ing parietal pain (Fig. 10.2). abdominal pain by the age of 15 years. Up to 28% of children complain of abdominal pain at least once per week and only 2% seek medical ACUTE ABDOMINAL PAIN attention. The primary care physician, pediatrician, emergency physi- cian, and surgeon must be able to distinguish serious and potentially The clinician evaluating the child with abdominal pain of acute onset life-threatening diseases from more benign problems (Table 10.1). must decide quickly whether the child has a “surgical abdomen” (a Abdominal pain may be a single acute event (Tables 10.2 and 10.3), a serious medical problem necessitating treatment and admission to the recurring acute problem (as in abdominal migraine), or a chronic hospital) or a process that can be managed on an outpatient basis. problem (Table 10.4). The differential diagnosis is lengthy, differs from Even though surgical diagnoses are fewer than 10% of all causes of that in adults, and varies by age group. -

Foramen in Xiphoid Process of Sternum
[Sabnis et. al., Vol.7 (Iss.12): December 2019] ISSN- 2350-0530(O), ISSN- 2394-3629(P) Index Copernicus Value (ICV 2018): 86.20 DOI: https://doi.org/10.29121/granthaalayah.v7.i12.2019.317 Science FORAMEN IN XIPHOID PROCESS OF STERNUM Dr Anjali Sabnis 1, Dr. Prakash Mane 2 1 Professor and head, Department of Anatomy, MGM Medical College, Navi Mumbai 2 Tutor, Department of Anatomy, MGM Medical College, Navi Mumbai Abstract Xiphoid process is smallest and distal component of manubrium sternum which is located in epigastrium. Variations in size and shape of xiphoid process are commonly observed. During teaching sternum to 1st M.B.B.S. students of MGM Medical College, Navi Mumbai, two small foramina in two different xiphoid processes were noticed. Though presence of foramen in xiphoid process is not uncommon, their presence should not be ignored. During assessment of injuries in autopsy, post-mortem examination and radiological reporting knowledge of xiphoid process and foramina in xiphoid process will be helpful. Keywords: Foramen; Xiphoid Process; Manubrium; Sternum; Perforation. Cite This Article: Dr Anjali Sabnis, and Dr. Prakash Mane. (2019). “FORAMEN IN XIPHOID PROCESS OF STERNUM.” International Journal of Research - Granthaalayah, 7(12), 239-242. https://doi.org/10.29121/granthaalayah.v7.i12.2019.317. 1. Introduction Sternum is a flat bone which forms anterior boundary of thoracic wall. Prosternum or manubrium, mesosternum or body and metasternum or xiphoid process are the three components of sternum. The distal and smallest component is xiphoid process which is located in epigastrium. Xiphoid process is derived from the Greek word “xiphos” means straight sword1.