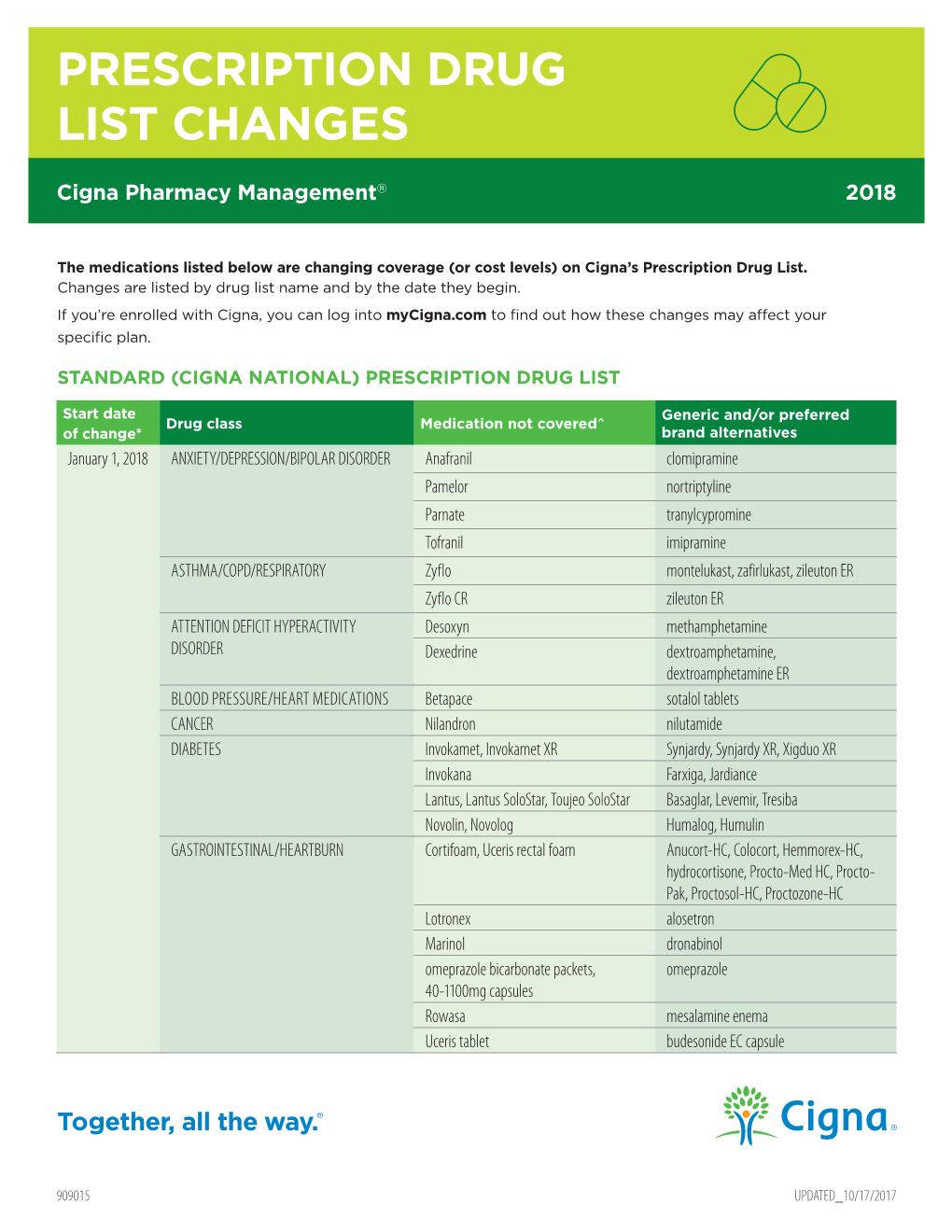
Prescription Drug List Changes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Use of Ceftaroline Fosamil in Children: Review of Current Knowledge and Its Application
Infect Dis Ther (2017) 6:57–67 DOI 10.1007/s40121-016-0144-8 REVIEW Use of Ceftaroline Fosamil in Children: Review of Current Knowledge and its Application Juwon Yim . Leah M. Molloy . Jason G. Newland Received: November 10, 2016 / Published online: December 30, 2016 Ó The Author(s) 2016. This article is published with open access at Springerlink.com ABSTRACT infections, CABP caused by penicillin- and ceftriaxone-resistant S. pneumoniae and Ceftaroline is a novel cephalosporin recently resistant Gram-positive infections that fail approved in children for treatment of acute first-line antimicrobial agents. However, bacterial skin and soft tissue infections and limited data are available on tolerability in community-acquired bacterial pneumonia neonates and infants younger than 2 months (CABP) caused by methicillin-resistant of age, and on pharmacokinetic characteristics Staphylococcus aureus, Streptococcus pneumoniae in children with chronic medical conditions and other susceptible bacteria. With a favorable and those with invasive, complicated tolerability profile and efficacy proven in infections. In this review, the microbiological pediatric patients and excellent in vitro profile of ceftaroline, its mechanism of action, activity against resistant Gram-positive and and pharmacokinetic profile will be presented. Gram-negative bacteria, ceftaroline may serve Additionally, clinical evidence for use in as a therapeutic option for polymicrobial pediatric patients and proposed place in therapy is discussed. Enhanced content To view enhanced content for this article go to http://www.medengine.com/Redeem/ 1F47F0601BB3F2DD. Keywords: Antibiotic resistance; Ceftaroline J. Yim (&) fosamil; Children; Methicillin-resistant St. John Hospital and Medical Center, Detroit, MI, Staphylococcus aureus; Streptococcus pneumoniae USA e-mail: [email protected] L. -

Adverse Drug Reactions Sample Chapter
Sample copyright Pharmaceutical Press www.pharmpress.com 5 Drug-induced skin reactions Anne Lee and John Thomson Introduction Cutaneous drug eruptions are one of the most common types of adverse reaction to drug therapy, with an overall incidence rate of 2–3% in hos- pitalised patients.1–3 Almost any medicine can induce skin reactions, and certain drug classes, such as non-steroidal anti-inflammatory drugs (NSAIDs), antibiotics and antiepileptics, have drug eruption rates approaching 1–5%.4 Although most drug-related skin eruptions are not serious, some are severe and potentially life-threatening. Serious reac- tions include angio-oedema, erythroderma, Stevens–Johnson syndrome and toxic epidermal necrolysis. Drug eruptions can also occur as part of a spectrum of multiorgan involvement, for example in drug-induced sys- temic lupus erythematosus (see Chapter 11). As with other types of drug reaction, the pathogenesis of these eruptions may be either immunological or non-immunological. Healthcare professionals should carefully evalu- ate all drug-associated rashes. It is important that skin reactions are identified and documented in the patient record so that their recurrence can be avoided. This chapter describes common, serious and distinctive cutaneous reactions (excluding contact dermatitis, which may be due to any external irritant, including drugs and excipients), with guidance on diagnosis and management. A cutaneous drug reaction should be suspected in any patient who develops a rash during a course of drug therapy. The reaction may be due to any medicine the patient is currently taking or has recently been exposed to, including prescribed and over-the-counter medicines, herbal or homoeopathic preparations, vaccines or contrast media. -

Pristiq (Desvenlafaxine Succinate) – First-Time Generic
Pristiq® (desvenlafaxine succinate) – First-time generic • On March 1, 2017, Teva launched AB-rated generic versions of Pfizer’s Pristiq (desvenlafaxine succinate) 25 mg, 50 mg, and 100 mg extended-release tablets for the treatment of major depressive disorder. — Teva launched the 25 mg tablet with 180-day exclusivity. — In addition, Alembic/Breckenridge, Mylan, and West-Ward have launched AB-rated generic versions of Pristiq 50 mg and 100 mg extended-release tablets. — Greenstone’s launch plans for authorized generic versions of Pristiq 25 mg, 50 mg, and 100 mg tablets are pending. — Lupin and Sandoz received FDA approval of AB-rated generic versions of Pristiq 50 mg and 100 mg tablets on June 29, 2015. Lupin’s and Sandoz’s launch plans are pending. • Other serotonin-norepinephrine reuptake inhibitors approved for the treatment of major depressive disorder include desvenlafaxine fumarate, duloxetine, Fetzima™ (levomilnacipran), Khedezla™ (desvenlafaxine) , venlafaxine, and venlafaxine extended-release. • Pristiq and the other serotonin-norepinephrine reuptake inhibitors carry a boxed warning for suicidal thoughts and behaviors. • According to IMS Health data, the U.S. sales of Pristiq were approximately $883 million for the 12 months ending on December 31, 2016. optumrx.com OptumRx® specializes in the delivery, clinical management and affordability of prescription medications and consumer health products. We are an Optum® company — a leading provider of integrated health services. Learn more at optum.com. All Optum® trademarks and logos are owned by Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owners. This document contains information that is considered proprietary to OptumRx and should not be reproduced without the express written consent of OptumRx. -

Desvenlafaxine
https://providers.amerigroup.com CONTAINS CONFIDENTIAL PATIENT INFORMATION desvenlafaxine Prior Authorization of Benefits (PAB) Form Complete form in its entirety and fax to: Prior Authorization of Benefits Center at 1-844-512-9004 Provider Help Desk 1-800-454-3730 1. PATIENT INFORMATION 2. PHYSICIAN INFORMATION Patient Name: Prescribing Physician: Patient ID #: Physician Address: Patient DOB: Physician Phone #: Date of Rx: Physician Fax #: Patient Phone #: Physician Specialty: Patient Email Address: Physician DEA: Physician NPI #: Physician Email Address: 3. MEDICATION 4. STRENGTH 5. DIRECTIONS 6. QUANTITY PER 30 DAYS desvenlafaxine Specify: 7. DIAGNOSIS: 8. APPROVAL CRITERIA: CHECK ALL BOXES THAT APPLY NOTE: Any areas not filled out are considered not applicable to your patient & MAY AFFECT THE OUTCOME of this request. □ Yes □ No Documentation of a previous trial and therapy failure at a therapeutic dose with two preferred generic SSRIs* has been provided If No: □ Yes □ No Documented evidence is provided that the use of these agents would be medically contraindicated □ Yes □ No Documentation of a previous trial and therapy failure at a therapeutic dose with one preferred generic SNRI** has been provided If No: □ Yes □ No Documented evidence is provided that the use of these agents would be medically contraindicated □ Yes □ No Documentation of a previous trial and therapy failure at a therapeutic dose with one non-SSRI/SNRI generic antidepressant** has been provided If No: □ Yes □ No Documented evidence is provided that the use of these -

CT Myelogram Drugs to Avoid Hold for 48 Hours Before and 12 Hours After Your Myelogram UVA Neuroradiology
CT Myelogram Drugs to Avoid Hold for 48 Hours Before and 12 Hours After Your Myelogram UVA Neuroradiology Generic Name (Brand Name) Cidofovir (Vistide) Acetaminophen/butalbital (Allzital; Citalopram (Celexa) Bupap) Clomipramine (Anafranil) Acetaminophen/butalbital/caffeine Clonidine (Catapres; Kapvay) (Fioricet; Butace) Clorazepate (Tranxene-T) Acetaminophen/butalbital/caffeine/ Clozapine (Clozaril; FazaClo; Versacloz) codeine (Fioricet with codeine) Cyclizine (No Brand Name) Acetaminophen/caffeine (Excedrin) Cyclobenzaprine (Flexeril) Acetaminophen/caffeine/dihydrocodeine Desipramine (Norpramine) (Panlor; Trezix) Desvenlafaxine (Pristiq; Khedezla) Acetaminophen/tramadol (Ultracet) Dexmethylphenidate (Focalin) Aliskiren (Tekturna) Dextroamphetamine (Dexedrine; Amitriptyline (Elavil) ProCentra; Zenzedi) Amitriptyline and chlordiazepoxide Dextroamphetamine and amphetamine (Limbril) (Adderall) Amoxapine (Asendin) Diazepam (Valium; Diastat) Aripiprazole (Abilify) Diethylpropion (No Brand Name) Armodafinil (Nuvigil) Dimenhydrinate (Dramamine) Asenapine (Saphris) Donepezil (Aricept) Aspirin/caffeine (BC Powder; Goody Doripenem (Doribax) Powder) Doxapram (Dopram) Atomoxetine (Strattera) Doxepin (Silenor) Baclofen (Gablofen; Lioresal) Droperidol (No Brand Name) Benzphetamine (Didrex; Regimex) Duloxetine (Cymbalta) Benztropine (Cogentin) Entacapone (Comtan) Bismuth Ergotamine and caffeine (Cafergot; subcitrate/metronidazole/tetracycline Migergot) (Pylera) Escitalopram (Lexapro) Bismuth subsalicylate (Pepto-Bismol) Fluoxetine (Prozac; Sarafem) -

Pharmaceuticals Appendix
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ADAPALENE 106685-40-9 ABANOQUIL 90402-40-7 ADAPROLOL 101479-70-3 ABECARNIL 111841-85-1 ADEMETIONINE 17176-17-9 ABLUKAST 96566-25-5 ADENOSINE PHOSPHATE 61-19-8 ABUNIDAZOLE 91017-58-2 ADIBENDAN 100510-33-6 ACADESINE 2627-69-2 ADICILLIN 525-94-0 ACAMPROSATE 77337-76-9 ADIMOLOL 78459-19-5 ACAPRAZINE 55485-20-6 ADINAZOLAM 37115-32-5 ACARBOSE 56180-94-0 ADIPHENINE 64-95-9 ACEBROCHOL 514-50-1 ADIPIODONE 606-17-7 ACEBURIC ACID 26976-72-7 ADITEREN 56066-19-4 ACEBUTOLOL 37517-30-9 ADITOPRIME 56066-63-8 ACECAINIDE 32795-44-1 ADOSOPINE 88124-26-9 ACECARBROMAL 77-66-7 ADOZELESIN 110314-48-2 ACECLIDINE 827-61-2 ADRAFINIL 63547-13-7 ACECLOFENAC 89796-99-6 ADRENALONE 99-45-6 ACEDAPSONE 77-46-3 AFALANINE 2901-75-9 ACEDIASULFONE SODIUM 127-60-6 AFLOQUALONE 56287-74-2 ACEDOBEN 556-08-1 AFUROLOL 65776-67-2 ACEFLURANOL 80595-73-9 AGANODINE 86696-87-9 ACEFURTIAMINE 10072-48-7 AKLOMIDE 3011-89-0 ACEFYLLINE CLOFIBROL 70788-27-1 -

Safety and Efficacy of Ceftaroline Fosamil in the Management of Community-Acquired Bacterial Pneumonia Heather F
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Scholarly Papers 2014 Safety and Efficacy of Ceftaroline Fosamil in the Management of Community-Acquired Bacterial Pneumonia Heather F. DeBellis Kimberly L. Barefield Philadelphia College of Osteopathic Medicine, [email protected] Follow this and additional works at: https://digitalcommons.pcom.edu/scholarly_papers Part of the Medicine and Health Sciences Commons Recommended Citation DeBellis, Heather F. and Barefield, Kimberly L., "Safety and Efficacy of Ceftaroline Fosamil in the Management of Community- Acquired Bacterial Pneumonia" (2014). PCOM Scholarly Papers. 1913. https://digitalcommons.pcom.edu/scholarly_papers/1913 This Article is brought to you for free and open access by DigitalCommons@PCOM. It has been accepted for inclusion in PCOM Scholarly Papers by an authorized administrator of DigitalCommons@PCOM. For more information, please contact [email protected]. Open Access: Full open access to Clinical Medicine Reviews this and thousands of other papers at http://www.la-press.com. in Therapeutics Safety and Efficacy of Ceftaroline Fosamil in the Management of Community- Acquired Bacterial Pneumonia Heather F. DeBellis and Kimberly L. Tackett South University School of Pharmacy, Savannah, GA, USA. ABSTR ACT: Ceftaroline fosamil is a new fifth-generation cephalosporin indicated for the treatment of community-acquired bacterial pneumonia (CABP). It possesses antimicrobial effects against both Gram-positive and Gram-negative bacteria, including methicillin-resistant Staphylococcus aureus (MRSA), but not against anaerobes. Organisms covered by this novel agent that are commonly associated with CABP are Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, Moraxella catarrhalis, and Klebsiella pneumoniae; however, ceftaroline fosamil lacks antimicrobial activity against Pseudomonas and Acinetobacter species. -

Methadone and Buprenorphine: Clinical Impact of Drug Interactions
11/03/2014 Methadone and Buprenorphine: Clinical Impact of Drug Interactions Elinore F. McCance-Katz, MD, PhD Disclosures None Adverse Drug Interactions • Accidents: leading cause of death in the USA in those aged 1–44 with highest rates in 25–44 y.o. • Poisoning: a leading cause of accidental deaths in the US – 145% increase in 1999–2007 – Opioids most frequently named drugs in poisonings • DDIs: a leading cause of accidental poisoning deaths in the USA (CDC, 2011) – Those exposed to DDIs between CYP450-metabolized opioids and other medications have higher medical costs (Summers et al, 2011) 1 11/03/2014 Underlying Reasons for DDIs • Many with opioid dependence have co-occurring medical and / or mental disorders • Patients believe prescribed drugs are ‘safe’ • Lack of patient education about adverse events that can occur • May not understand need to take as prescribed • Sharing / selling Pathophysiology of DDIs • Pharmacokinetic (PK) – What you do to the drug (or not) – With PK interactions, one drug causes an alteration in the concentration of another drug increasing risks of side effects or reduced effectiveness of the drug • Pharmacodynamic (PD) – What the drug or drugs do to you – With PD interactions, two drugs have additive effects or antagonistic effects Pharmacodynamic Interactions • PK interactions may have associated PD consequences • PD interactions can occur in the absence of a PK interaction • Two drugs with similar pharmacological characteristics interact synergistically – Increases potential toxicity of drug – Opioids -

Antidepressants, Other Review 04/14/2009
Antidepressants, Other Review 04/14/2009 Copyright © 2004 - 2009 by Provider Synergies, L.L.C. All rights reserved. Printed in the United States of America. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, digital scanning, or via any information storage and retrieval system without the express written consent of Provider Synergies, L.L.C. All requests for permission should be mailed to: Attention: Copyright Administrator Intellectual Property Department Provider Synergies, L.L.C. 5181 Natorp Blvd., Suite 205 Mason, Ohio 45040 The materials contained herein represent the opinions of the collective authors and editors and should not be construed to be the official representation of any professional organization or group, any state Pharmacy and Therapeutics committee, any state Medicaid Agency, or any other clinical committee. This material is not intended to be relied upon as medical advice for specific medical cases and nothing contained herein should be relied upon by any patient, medical professional or layperson seeking information about a specific course of treatment for a specific medical condition. All readers of this material are responsible for independently obtaining medical advice and guidance from their own physician and/or other medical professional in regard to the best course of treatment for their specific medical condition. This publication, inclusive of all forms contained herein, is intended to be -

Desvenlafaxine Drug Assessment Pristiq® in Major Depressive Report Disorder in Adults @DTB Navarre.Es More Cost for Less
03 2015 DESVENLAFAXINE DRUG ASSESSMENT Pristiq® in major depressive REPORT www.dtb.navarra.es disorder in adults @DTB_Navarre.es More cost for less... ABSTRACT Desvenlafaxine is an active me- tabolite of venlafaxine. Indications1 In the study against escitalopram4 flexible Treatment of major depressive disorder doses of desvenlafaxine were used (100 and In three placebo-controlled 200 mg daily) in postmenopausal women. No trials, the results on the reduc- 1 Mechanism of action advantage of desvenlafaxine over escitalopram tion in HAM-D17 score were not This is an active metabolite of venlafaxine, that was found. consistent. inhibits the reuptake of serotonine and nora- There is only one long-term study16 that eva- dernaline. Its bioavailability reaches up to 80% luated relapse prevention. Patients responding The most common adverse while elimination occurs without alteration after 8 weeks of treatment with desvenlafaxine effects are of gastrointestinal through the urine (45%) and metabolism by 50 mg daily and with a stable response up to origin or sleep disorders. There glucurono conjugation (19%). week 20 were randomized either to placebo or are no available long-term safe- desvenlafaxine 50 mg daily for 6 months. The ty data. Dosage and administration1 endpoint was time to relapse (defined as HAM- The recommended dose is 50 mg daily. The ta- D17 score ≥16), treatment withdrawal due to In the only head-to-head trial blets are swallowed wholly, with liquid with or unsatisfactory response, hospital admission carried out in post-menopause without food and at the same time. The increa- due to depression, suicide attempt or suicide. women, desvenlafaxine at high se in doses should be gradual and up to a maxi- Time to relapse was significantly lower in the doses did not show superiority mum of 200 mg daily and at intervals of at least case of placebo compared to desvenlafaxine versus escitalopram. -

Ceftaroline in Complicated Skin and Skin-Structure Infections
Infection and Drug Resistance Dovepress open access to scientific and medical research Open Access Full Text Article REVIEW Ceftaroline in complicated skin and skin-structure infections Paul O Hernandez1 Abstract: Ceftaroline is an advanced-generation cephalosporin antibiotic recently approved by Sergio Lema2 the US Food and Drug Administration for the treatment of complicated skin and skin-structure Stephen K Tyring3 infections (cSSSIs). This intravenous broad-spectrum antibiotic exerts potent bactericidal activity Natalia Mendoza2,4 by inhibiting bacterial cell wall synthesis. A high affinity for the penicillin-binding protein 2a (PBP2a) of methicillin-resistant Staphylococcus aureus (MRSA) makes the drug especially 1University of Texas School of Medicine at San Antonio, beneficial to patients with MRSA cSSSIs. Ceftaroline has proved in multiple well-conducted San Antonio, TX, 2Woodhull clinical trials to have an excellent safety and efficacy profile. In adjusted doses it is also recom- Medical and Mental Health Center, mended for patients with renal or hepatic impairment. Furthermore, the clinical effectiveness Brooklyn, NY, 3Department of Dermatology, University of Texas and high cure rate demonstrated by ceftaroline in cSSSIs, including those caused by MRSA Health Science Center at Houston, and other multidrug-resistant strains, warrants its consideration as a first-line treatment option 4 Houston, TX, USA; Department of for cSSSIs. This article reviews ceftaroline and its pharmacology, efficacy, and safety data to Dermatology, El -

Pharmacokinetic and Pharmacodynamic Interactions Between Antiepileptics and Antidepressants Domenico Italiano University of Messina, Italy
University of Kentucky UKnowledge Psychiatry Faculty Publications Psychiatry 11-2014 Pharmacokinetic and Pharmacodynamic Interactions between Antiepileptics and Antidepressants Domenico Italiano University of Messina, Italy Edoardo Spina University of Messina, Italy Jose de Leon University of Kentucky, [email protected] Right click to open a feedback form in a new tab to let us know how this document benefits oy u. Follow this and additional works at: https://uknowledge.uky.edu/psychiatry_facpub Part of the Psychiatry and Psychology Commons Repository Citation Italiano, Domenico; Spina, Edoardo; and de Leon, Jose, "Pharmacokinetic and Pharmacodynamic Interactions between Antiepileptics and Antidepressants" (2014). Psychiatry Faculty Publications. 40. https://uknowledge.uky.edu/psychiatry_facpub/40 This Article is brought to you for free and open access by the Psychiatry at UKnowledge. It has been accepted for inclusion in Psychiatry Faculty Publications by an authorized administrator of UKnowledge. For more information, please contact [email protected]. Pharmacokinetic and Pharmacodynamic Interactions between Antiepileptics and Antidepressants Notes/Citation Information Published in Expert Opinion on Drug Metabolism & Toxicology, v. 10, Issue 11, p. 1457-1489. © 2014 Taylor & Francis Group This is an Accepted Manuscript of an article published by Taylor & Francis Group in Expert Opinion on Drug Metabolism & Toxicology in Nov. 2014, available online: http://www.tandfonline.com/10.1517/ 17425255.2014.956081 Digital Object Identifier (DOI) http://dx.doi.org/10.1517/17425255.2014.956081 This article is available at UKnowledge: https://uknowledge.uky.edu/psychiatry_facpub/40 1 This is an Accepted Manuscript of an article published by Taylor & Francis Group in Expert Opinion on Drug Metabolism & Toxicology in Nov.