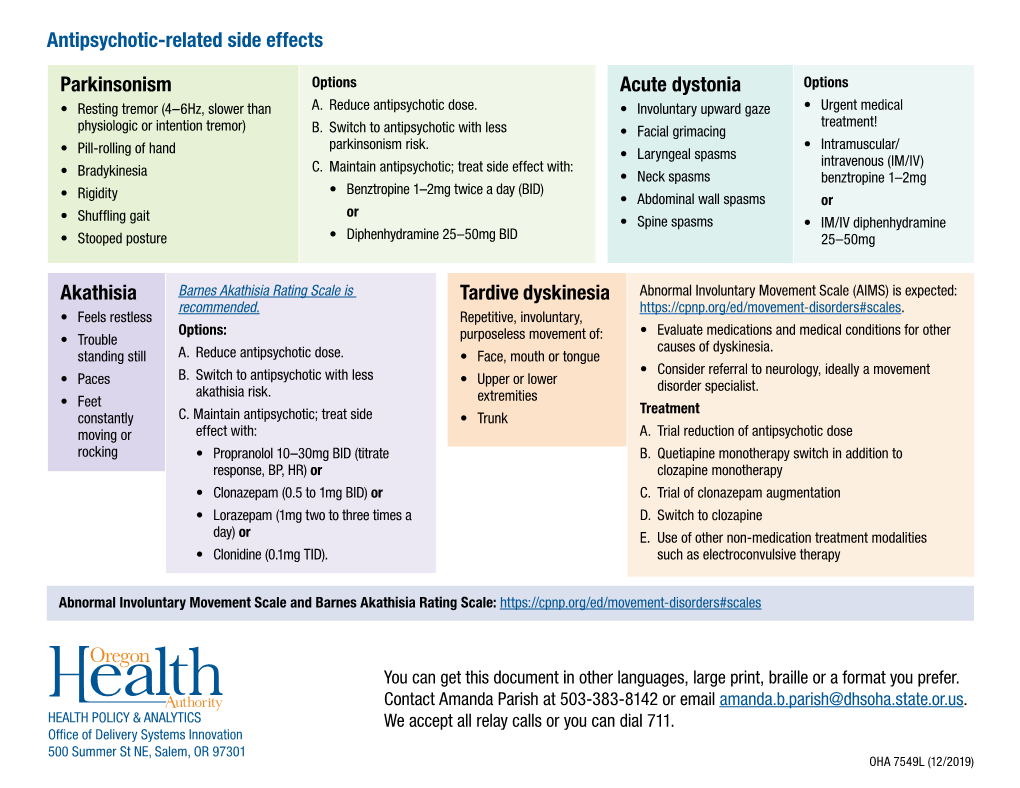
Antipsychotic-Related Side Effects Parkinsonism Akathisia Acute
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vocal Cord Dysfunction in Amyotrophic Lateral Sclerosis Four Cases and a Review of the Literature
NEUROLOGICAL REVIEW SECTION EDITOR: DAVID E. PLEASURE, MD Vocal Cord Dysfunction in Amyotrophic Lateral Sclerosis Four Cases and a Review of the Literature Maaike M. van der Graaff, MD; Wilko Grolman, MD, PhD; Erik J. Westermann, MD; Hans C. Boogaardt; Hans Koelman, MD, PhD; Anneke J. van der Kooi, MD, PhD; Marina A. Tijssen, MD, PhD; Marianne de Visser, MD, PhD e describe 4 patients with amyotrophic lateral sclerosis (ALS) and glottic nar- rowing due to vocal cord dysfunction, and review the literature found using the following search terms: amyotrophic lateral sclerosis, motor neuron disease, stri- dor, laryngospasm, vocal cord abductor paresis, and hoarseness. Neurological Wliterature rarely reports vocal cord dysfunction in ALS, in contrast to otolaryngology literature (4%- 30% of patients with ALS). Both infranuclear and supranuclear mechanisms may play a role. Vocal cord dysfunction can occur at any stage of disease and may account for sudden death in ALS. Treat- ment of severe cases includes acute airway management and tracheotomy. Arch Neurol. 2009;66(11):1329-1333 Amyotrophic lateral sclerosis (ALS) is a neu- (VCAP), it is potentially life threatening, as rodegenerative disease characterized by fea- a predominance of vocal cord adduction re- tures indicative of both upper and lower sults in glottic narrowing or even occlu- motor neuron degeneration. Initial manifes- sion. Assessment by an otolaryngologist is tations usually include weakness in the bul- then of the highest priority. Stridor is a well- bar region or weakness of the limbs. Progres- known symptom in multiple system atro- sive weakness leads to increasing disability phy and may also incidentally occur in other and respiratory insufficiency, resulting in neurodegenerative diseases.8-10 Laryngo- death. -

Diagnosis and Treatment of Multiple System Atrophy: an Update
ReviewSection Article Diagnosis and Treatment of Multiple System Atrophy: an Update Abstract the common parkinsonian variant (MSA-P) from PD. In his review provides an update on the diagnosis a clinicopathologic study1, primary neurologists (who Tand therapy of multiple system atrophy (MSA), a followed up the patients clinically) identified only 25% of sporadic neurodegenerative disorder characterised MSA patients at the first visit (42 months after disease clinically by any combination of parkinsonian, auto- onset) and even at their last neurological follow-up (74 nomic, cerebellar or pyramidal symptoms and signs months after disease onset), half of the patients were still and pathologically by cell loss, gliosis and glial cyto- misdiagnosed with the correct diagnosis in the other half plasmic inclusions in several brain and spinal cord being established on average 4 years after disease onset. structures. The term MSA was introduced in 1969 Mean rater sensitivity for movement disorder specialists although prior to this cases of MSA were reported was higher but still suboptimal at the first (56%) and last Gregor Wenning obtained an MD at the under the rubrics of striatonigral degeneration, olivo- (69%) visit. In 1998 an International Consensus University of Münster pontocerebellar atrophy, Shy-Drager syndrome and Conference promoted by the American Academy of (Germany) in 1991 and idiopathic orthostatic hypotension. In the late Neurology was convened to develop new and optimised a PhD at the University nineties, |-synuclein immunostaining was recognised criteria for a clinical diagnosis of MSA2, which are now of London in 1996. He received his neurology as the most sensitive marker of inclusion pathology in widely used by neurologists. -

Free PDF Download
European Review for Medical and Pharmacological Sciences 2021; 25: 4746-4756 Pathophysiology and management of Akathisia 70 years after the introduction of the chlorpromazine, the first antipsychotic N. ZAREIFOPOULOS1, M. KATSARAKI1, P. STRATOS1, V. VILLIOTOU, M. SKALTSA1, A. DIMITRIOU1, M. KARVELI1, P. EFTHIMIOU2, M. LAGADINOU2, D. VELISSARIS3 1Department of Psychiatry, General Hospital of Nikea and Pireus Hagios Panteleimon, Athens, Greece 2Emergency Department, University General Hospital of Patras, Athens, Greece 3Department of Internal Medicine, University of Patras School of Medicine, Athens, Greece Abstract. – OBJECTIVE: Akathisia is among CONCLUSIONS: Pharmacological manage- the most troubling effects of psychiatric drugs ment may pose a challenge in chronic akathi- as it is associated with significant distress on sia. Rotation between different pharmacologi- behalf of the patients, and it limits treatment ad- cal management strategies may be optimal in re- herence. Though it most commonly presents sistant cases. Discontinuation of the causative during treatment with antipsychotic drugs which drug and use of b-blockers, mirtazapine, benzo- block dopamine D2 receptors, Akathisia has al- diazepines or gabapentinoids for symptomatic so been reported during treatment with selec- relief is the basis of management. tive serotonin reuptake inhibitors (SSRIs), se- rotonin norepinephrine reuptake inhibitors (SN- Key Words: RIs), stimulants, mirtazapine, tetrabenazine and Aripiprazole, Extrapyramidal symptoms, Haloperi- other drugs. dol, -

Clinical Manifestation of Juvenile and Pediatric HD Patients: a Retrospective Case Series
brain sciences Article Clinical Manifestation of Juvenile and Pediatric HD Patients: A Retrospective Case Series 1, , 2, 2 1 Jannis Achenbach * y, Charlotte Thiels y, Thomas Lücke and Carsten Saft 1 Department of Neurology, Huntington Centre North Rhine-Westphalia, St. Josef-Hospital Bochum, Ruhr-University Bochum, 44791 Bochum, Germany; [email protected] 2 Department of Neuropaediatrics and Social Paediatrics, University Children’s Hospital, Ruhr-University Bochum, 44791 Bochum, Germany; [email protected] (C.T.); [email protected] (T.L.) * Correspondence: [email protected] These two authors contribute to this paper equally. y Received: 30 April 2020; Accepted: 1 June 2020; Published: 3 June 2020 Abstract: Background: Studies on the clinical manifestation and course of disease in children suffering from Huntington’s disease (HD) are rare. Case reports of juvenile HD (onset 20 years) describe ≤ heterogeneous motoric and non-motoric symptoms, often accompanied with a delay in diagnosis. We aimed to describe this rare group of patients, especially with regard to socio-medical aspects and individual or common treatment strategies. In addition, we differentiated between juvenile and the recently defined pediatric HD population (onset < 18 years). Methods: Out of 2593 individual HD patients treated within the last 25 years in the Huntington Centre, North Rhine-Westphalia (NRW), 32 subjects were analyzed with an early onset younger than 21 years (1.23%, juvenile) and 18 of them younger than 18 years of age (0.69%, pediatric). Results: Beside a high degree of school problems, irritability or aggressive behavior (62.5% of pediatric and 31.2% of juvenile cases), serious problems concerning the social and family background were reported in 25% of the pediatric cohort. -

Rest Tremor Revisited: Parkinson's Disease and Other Disorders
Chen et al. Translational Neurodegeneration (2017) 6:16 DOI 10.1186/s40035-017-0086-4 REVIEW Open Access Rest tremor revisited: Parkinson’s disease and other disorders Wei Chen1,2, Franziska Hopfner2, Jos Steffen Becktepe2 and Günther Deuschl1,2* Abstract Tremor is the most common movement disorder characterized by a rhythmical, involuntary oscillatory movement of a body part. Since distinct diseases can cause similar tremor manifestations and vice-versa,itischallengingtomakean accurate diagnosis. This applies particularly for tremor at rest. This entity was only rarely studied in the past, although a multitude of clinical studies on prevalence and clinical features of tremor in Parkinson’s disease (PD), essential tremor and dystonia, have been carried out. Monosymptomatic rest tremor has been further separated from tremor-dominated PD. Rest tremor is also found in dystonic tremor, essential tremor with a rest component, Holmes tremor and a few even rarer conditions. Dopamine transporter imaging and several electrophysiological methods provide additional clues for tremor differential diagnosis. New evidence from neuroimaging and electrophysiological studies has broadened our knowledge on the pathophysiology of Parkinsonian and non-Parkinsonian tremor. Large cohort studies are warranted in future to explore the nature course and biological basis of tremor in common tremor related disorders. Keywords: Tremor, Parkinson’s disease, Essential tremor, Dystonia, Pathophysiology Background and clinical correlates of tremor in common tremor re- Tremor is defined as a rhythmical, involuntary oscillatory lated disorders. Some practical clinical cues and ancillary movement of a body part [1]. Making an accurate diagnosis tests for clinical distinction are found [3]. Besides, accu- of tremor disorders is challenging, since similar clinical mulating structural and functional neuroimaging, as well entities may be caused by different diseases. -

Donepezil-Induced Cervical Dystonia in Alzheimer's Disease: a Case
□ CASE REPORT □ Donepezil-induced Cervical Dystonia in Alzheimer’s Disease: A Case Report and Literature Review of Dystonia due to Cholinesterase Inhibitors Ken Ikeda, Masaru Yanagihashi, Masahiro Sawada, Sayori Hanashiro, Kiyokazu Kawabe and Yasuo Iwasaki Abstract We herein report an 81-year-old woman with Alzheimer’s disease (AD) in who donepezil, a cholinesterase inhibitor (ChEI), caused cervical dystonia. The patient had a two-year history of progressive memory distur- bance fulfilling the NINCDS-ADRDA criteria for probable AD. Mini-Mental State Examination score was 19/30. The remaining examination was normal. After a single administration of donepezil (5 mg/day) for 10 months, she complained of dropped head. Neurological examination and electrophysiological studies sup- ported a diagnosis of cervical dystonia. Antecollis disappeared completely at 6 weeks after cessation of done- pezil. Dystonic posture can occur at various timings of ChEI use. Physicians should pay more attention to rapidly progressive cervical dystonia in ChEI-treated AD patients. Key words: Alzheimer’s disease, cholinesterase inhibitor, donepezil, cervical dystonia, dropped head, Pisa syndrome (Intern Med 53: 1007-1010, 2014) (DOI: 10.2169/internalmedicine.53.1857) Introduction Case Report Tardive dystonia syndrome is known as the complication An 81-year-old woman developed a progressive global in- of prolonged treatment with antipsychotic medications, par- tellectual deterioration for two years and visited our depart- ticularly classic antipsychotics. Pisa syndrome or pleurotho- ment. The first score of Mini-Mental State Examination tonus is a distinct form of tardive dystonia characterized by (MMSE) was 19/30. The remaining neurological examina- abnormal, sustained posturing with flexion of the neck and tion was normal, showing no parkinsonism. -

Part Ii – Neurological Disorders
Part ii – Neurological Disorders CHAPTER 14 MOVEMENT DISORDERS AND MOTOR NEURONE DISEASE Dr William P. Howlett 2012 Kilimanjaro Christian Medical Centre, Moshi, Kilimanjaro, Tanzania BRIC 2012 University of Bergen PO Box 7800 NO-5020 Bergen Norway NEUROLOGY IN AFRICA William Howlett Illustrations: Ellinor Moldeklev Hoff, Department of Photos and Drawings, UiB Cover: Tor Vegard Tobiassen Layout: Christian Bakke, Division of Communication, University of Bergen E JØM RKE IL T M 2 Printed by Bodoni, Bergen, Norway 4 9 1 9 6 Trykksak Copyright © 2012 William Howlett NEUROLOGY IN AFRICA is freely available to download at Bergen Open Research Archive (https://bora.uib.no) www.uib.no/cih/en/resources/neurology-in-africa ISBN 978-82-7453-085-0 Notice/Disclaimer This publication is intended to give accurate information with regard to the subject matter covered. However medical knowledge is constantly changing and information may alter. It is the responsibility of the practitioner to determine the best treatment for the patient and readers are therefore obliged to check and verify information contained within the book. This recommendation is most important with regard to drugs used, their dose, route and duration of administration, indications and contraindications and side effects. The author and the publisher waive any and all liability for damages, injury or death to persons or property incurred, directly or indirectly by this publication. CONTENTS MOVEMENT DISORDERS AND MOTOR NEURONE DISEASE 329 PARKINSON’S DISEASE (PD) � � � � � � � � � � � -

Lower Limb Dystonia
Who is Affected by Lower What Support is Available? Limb Dystonia? What is Lower Limb Dystonia? The Dystonia Medical Research Foundation Dystonia affects men, women, and children Dystonia is a neurological disorder that (DMRF) can provide educational resources, of all ages and backgrounds. In children, causes involuntary muscle contractions. self-help opportunities, contact with others, lower limb dystonia may be an early symp - These muscle contractions result in volunteer opportunities, and connection to tom of an inherited dystonia. In these cases , abnormal movements and postures, the greater dystonia community. Lower Limb the dystonia may eventually generalize to making it difficult for individuals to Dystonia affect additional areas of the body. Children control their body movements. The What is the DMRF? with cerebral palsy may have limb dystonia, movements and postures may be painful . The Dystonia Medical Research Foundation often with spasticity (muscle tightness and Dystonic movements are typically (DMRF) is a 501(c)3 non-profit organizatio n rigidity). Lower limb dystonia in children patterned and repetitive. that funds medical research toward a cure, may be misdiagnosed as club foot, leading promotes awareness and education, and to unnecessary orthopedic procedures that Lower limb dystonia refers to dystonic supports the well being of affected individuals can worsen dystonia. movements and postures in the leg, foot , and families. and/or toes. It may also be referred to as When seen in adults, lower limb dystonia focal dystonia of the foot or leg. Individ - seems to affect women more often than men. uals often have to adapt their gait while To learn more about dystonia Age of onset is typically in the mid-40s. -

Neuroleptic Malignant-Like Syndrome
An uncommon adverse effect of levodopa CASE REPORT withdrawal in a patient taking antipsychotic medication: neuroleptic malignant-like syndrome SP Man 文兆彪 A patient with symptoms suggestive of neuroleptic malignant syndrome after levodopa withdrawal is described. The patient presented with persistent high fever, stupor, autonomic dysfunction, rigidity, and rhabdomyolysis. He was successfully treated with intravenous dantrolene, resumption of levodopa, and forced alkaline diuresis. Doctors should be aware of the risk of abrupt cessation of dopamine agonists. Introduction Neuroleptic malignant syndrome (NMS) is an idiosyncratic, potentially fatal complication of treatment with antipsychotic drugs that manifests as fever, muscle rigidity, and autonomic and mental dysfunction.1 A similar clinical presentation has also been reported to develop after withdrawal from dopamine agonists.2,3 Some authors have used the terms neuroleptic malignant-like syndrome (NMLS) or parkinsonism hyperpyrexia syndrome, as well as acute akinesia or the malignant syndrome in Parkinson disease, for such a condition.4,5 The objective of this paper was to describe the first patient with NMLS in Hong Kong. Case report An 84-year-old Chinese man had chronic schizophrenia and was treated with chlorpromazine 50 mg at night for many years. Eighteen months prior to the index admission, chlorpromazine was replaced by olanzapine 20 mg daily as he had experienced extrapyramidal symptoms. He was also given levodopa 100 mg and benserazide 25 mg 3 times daily. He was admitted to Tuen Mun Hospital, Hong Kong, for a fever of 39.5ºC on 24 April 2010. He was conscious and did not have any specific symptoms. All medications, including olanzapine and levodopa, were stopped at admission as he was not permitted anything by mouth. -

Managing Migraine
NEUROLOGY/EXPERT CLINICAL MANAGEMENT Managing Migraine Benjamin W. Friedman, MD, MS* *Corresponding Author. E-mail: [email protected], Twitter: @benjaminbwf. 0196-0644/$-see front matter Copyright © 2016 by the American College of Emergency Physicians. http://dx.doi.org/10.1016/j.annemergmed.2016.06.023 A podcast for this article is available at www.annemergmed.com. alertness, and appetite. Allodynia, an alteration of Continuing Medical Education exam for this article is available at nociception that causes typically non-noxious sensory http://www.acep.org/ACEPeCME/. stimuli (such as brushing one’s hair or shaving one’s face) to be perceived as painful, develops as acute migraine duration [Ann Emerg Med. 2017;69:202-207.] increases. This is thought to indicate involvement of higher-order central nervous system sensory relay stations, Editor’s Note: The Expert Clinical Management series notably, the thalamus. consists of shorter, practical review articles focused on the optimal approach to a specific sign, symptom, disease, Migraine was once believed to be a vascular headache. procedure, technology, or other emergency department Advanced imaging studies do not support this description challenge. These articles–typically solicited from and indicate that migraine is a neurologic disorder involving recognized experts in the subject area–will summarize the dysfunctional nociceptive processing.3 Abnormally activated best available evidence relating to the topic while including sensory pathways turn non-noxious stimuli into headache, practical recommendations where the evidence is photophobia, phonophobia, and osmophobia. Cortical incomplete or conflicting. spreading depression, a slow wave of brain depolarization, underlies migraine aura but has not been demonstrated clearly in migraine patients without aura. -

Multiple Developmental Forms of Parkinsonism. the Basis for Further Research As to the Pathogenesis of Parkinsonism
J Neural Transm (2002) 109: 1469–1475 Mini-Review: Multiple developmental forms of parkinsonism. The basis for further research as to the pathogenesis of parkinsonism P. Riederer and P. Foley Clinical Neurochemistry, Clinic for Psychiatry and Psychotherapy and NPF-Center of Excellence Research Laboratories, University of Würzburg, Federal Republic of Germany Received September, 2002; accepted October 31, 2002 Summary. A range of extrapyramidal disturbances have been reported in children following early brain damage. In adults, damage to the basal ganglia can elicit abnormal motor activity in either direction; it would seem reason- able that the same would apply to damage occurring at an earlier develop- mental stage. The Viennese paediatrician Widhalm described a hypokinetic/ parkinsonoid syndrome (‘infantile hypokinetic-hypertonic syndrome with Parkinson symptomatic’) presented by a significant minority of the children with extrapyramidal movement disturbances, corresponding to the mild rigid- akinetic type of Parkinson’s disease. In contrast to classical parkinsonism, but consistent with some forms of post-encephalitic parkinsonism, the syndrome was reversible, although only after l-DOPA therapy. Widhalm’s observation that at least one form of childhood parkinsonism can be cured with l-DOPA also suggests that the amino acid plays a more active role than mere replace- ment therapy in children, perhaps also acting as a neurotrophic agent. It is proposed that environmental factors, including viral and risk factors associ- ated with pregnancy and birth, together with genetically determined lability, may increase the incidence of early hypokinesia/parkinsonism in particular and of Parkinson’s disease in later life by disturbing the immature basal ganglia at critical developmental stages. -

Aggression and Agitation in Dementia, None of Which Are Approved by the US Food and Drug Administration
REVIEW ARTICLE 07/09/2018 on SruuCyaLiGD/095xRqJ2PzgDYuM98ZB494KP9rwScvIkQrYai2aioRZDTyulujJ/fqPksscQKqke3QAnIva1ZqwEKekuwNqyUWcnSLnClNQLfnPrUdnEcDXOJLeG3sr/HuiNevTSNcdMFp1i4FoTX9EXYGXm/fCfl4vTgtAk5QA/xTymSTD9kwHmmkNHlYfO by https://journals.lww.com/continuum from Downloaded Aggression and Agitation CONTINUUM AUDIO Downloaded INTERVIEW AVAILABLE in Dementia ONLINE from By M. Uri Wolf, MD, FRCPC; Yael Goldberg, PhD, CPsych; https://journals.lww.com/continuum Morris Freedman, MD, FRCPC, FAAN CITE AS: CONTINUUM (MINNEAP MINN) 2018;24(3,BEHAVIORALNEUROLOGY AND PSYCHIATRY):783–803. ABSTRACT Address correspondence to by Dr M. Uri Wolf, Baycrest Health SruuCyaLiGD/095xRqJ2PzgDYuM98ZB494KP9rwScvIkQrYai2aioRZDTyulujJ/fqPksscQKqke3QAnIva1ZqwEKekuwNqyUWcnSLnClNQLfnPrUdnEcDXOJLeG3sr/HuiNevTSNcdMFp1i4FoTX9EXYGXm/fCfl4vTgtAk5QA/xTymSTD9kwHmmkNHlYfO PURPOSEOFREVIEW: This article reviews the treatment of aggression and Sciences, 3560 Bathurst St, agitation in dementia. Both nonpharmacologic and pharmacologic Toronto, ON M6A 2E1, Canada, approaches to responsive behaviors are discussed. Practical treatment [email protected]. strategies are applied to common behavioral symptoms. RELATIONSHIP DISCLOSURE: Drs Wolf and Goldberg report no disclosures. Dr Freedman serves RECENT FINDINGS: Aggressive and agitated behavior is common in dementia. as a trustee for the World Behavioral symptoms lead to reduced quality of life and distress for both Federation of Neurology and on patients and caregivers. They can also lead to poor outcomes and are the editorial boards