Active Detection of Tuberculosis: Tackling the Problem Head on in the Remote Area of Andaman and Nicobar Islands
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Recommendations on Improving Telecom Services in Andaman
Telecom Regulatory Authority of India Recommendations on Improving Telecom Services in Andaman & Nicobar Islands and Lakshadweep 22 nd July, 2014 Mahanagar Doorsanchar Bhawan Jawahar Lal Nehru Marg, New Delhi – 110002 CONTENTS CHAPTER-I: INTRODUCTION 1 CHAPTER- II: METHODOLOGY FOLLOWED FOR THE ASSESSMENT OF THE TELECOM INFRASTRUCTURE REQUIRED 10 CHAPTER- III: TELECOM PLAN FOR ANDAMAN & NICOBAR ISLANDS 36 CHAPTER- IV: COMPREHENSIVE TELECOM PLAN FOR LAKSHADWEEP 60 CHAPTER- V: SUPPORTING POLICY INITIATIVES 74 CHAPTER- VI: SUMMARY OF RECOMMENDATIONS 84 ANNEXURE 1.1 88 ANNEXURE 1.2 90 ANNEXURE 2.1 95 ANNEXURE 2.2 98 ANNEXURE 3.1 100 ANNEXURE 3.2 101 ANNEXURE 5.1 106 ANNEXURE 5.2 110 ANNEXURE 5.3 113 ABBREVIATIONS USED 115 i CHAPTER-I: INTRODUCTION Reference from Department of Telecommunication 1.1. Over the last decade, the growth of telecom infrastructure has become closely linked with the economic development of a country, especially the development of rural and remote areas. The challenge for developing countries is to ensure that telecommunication services, and the resulting benefits of economic, social and cultural development which these services promote, are extended effectively and efficiently throughout the rural and remote areas - those areas which in the past have often been disadvantaged, with few or no telecommunication services. 1.2. The Role of telecommunication connectivity is vital for delivery of e- Governance services at the doorstep of citizens, promotion of tourism in an area, educational development in terms of tele-education, in health care in terms of telemedicine facilities. In respect of safety and security too telecommunication connectivity plays a vital role. -

TERESSA ISLAND Sl.No
TERESSA ISLAND Sl.No. Particulars 31.12.2006 1. Area (Sq Km) 101.40 2. Census Villages (2001Census) 11 (i) Inhabited 11 1 Aloorang 2 Aloora 3 Enam 4Luxi 5 Kalara 6 Chuk Machi 7 Safed Balu 8 Minyuk 9 Kanahinot 10 Kalasi 11 Bengali (ii) Uninhabitted NIL 3. Revenue Villages NIL 4. Panchayat Bodies NIL 5. House Holds (2001 Census) 415 6. Population (2001 Census) 2026 Male 1081 Female 945 7. ST Population (2001 Census) 1826 Male 944 Female 882 8. Languages Spoken Nicobari & Hindi 9. Main Religion Hinduism, Christianity & Islam 10. Occupation – Main Workers (2001 Census) (i) Cultivators 4 (ii) Household Industries 443 (iii) Other Workers 184 11. Villages provided with piped water 5 supply 12. Health Service (a) Institutions (i) Primary Health Centre 1 (ii) Sub Centre 4 (b) Health Manpower (i) Doctors 1 (ii) Nurses/Midwives/LHVs 10 (iii) Para Medical Staff 29 (c) Bed Strength 10 13. Civil Supplies (i) Fair Price Shops 1 (ii) Ration Cards 947 (iii) Quantity Of Rice (Kg) 50000 14. Education (a) Institutions (i) Primary School 7 (ii) Middle School 1 (iii) Secondary School 1 59 ISLAND-WISE STATISTICAL OUTLINE - 2006 (b) Enrolment (i) Primary School 183 (ii) Middle School 82 (iii) Secondary School 193 (c) Teaching Staff (i) Primary School 10 (ii) Middle School 7 (iii) Secondary School 9 15. Social Welfare NIL 16. Electricity (i) Villages electrified 6 (ii) Electric Connections provided 4 17. Agriculture (i) Cultivable Area NE (ii) Main Crops Coconut & Arecanut (iii) Irrigation Sources NIL 18. Veterinary Service (i) Veterinary Sub Dispensary 1 (ii) Artificial insemination centre 1 (iii) Para Veterinary Staff 2 19. -

November 17-2
Tuesday 2 Daily Telegrams November 17, 2020 GOVT. PRIMARY SCHOOL No. TN/DB/PHED/2020/1277 27 SUBHASGRAM - 2 HALDER PARA, SARDAR TIKREY DO OFFICE OF THE EXECUTIVE ENGINEER NSV, SUBHASHGRAM GOVT. PRIMARY SCHOOL PUBLIC HEALTH ENGINEERING DIVISION 28 SUBHASGRAM - 3 DAS PARA, DAKHAIYA PARA DO A.P.W.D., PORT BLAIR NSV, SUBHASHGRAM th SCHOOL TIKREY, SUB CENTER Prothrapur, dated the 13 November 2020. COMMUNITY HALL, 29 KHUDIRAMPUR AREA, STEEL BRIDGE, AAGA DO KHUDIRAMPUR TENDER NOTICE NALLAH, DAM AREA (F) The Executive Engineer, PHED, APWD, Prothrapur invites on behalf of President of India, online Item Rate e- BANGLADESH QUARTER, MEDICAL RAMAKRISHNAG GOVT. PRIMARY SCHOOL tenders (in form of CPWD-8) from the vehicle owners / approved and eligible contractors of APWD and Non APWD 30 COLONY AREA, SAJJAL PARA, R K DO RAM - 1 RAMKRISHNAGRAM Contractors irrespective of their enlistment subject to the condition that they have experience of having successfully GRAM HOUSE SITE completed similar nature of work in terms of cost in any of the government department in A&N Islands and they should GOVT. PRIMARY SCHOOL RAMAKRISHNAG BAIRAGI PARA, MALO PARA, 31 VV PITH, DO not have any adverse remarks for following work RAM - 2 PAHAR KANDA NIT No. Earnest RAMKRISHNAGRAM Sl. Estimated cost Time of Name of work Money RAMAKRISHNAG COMMUNITY HALL, NEAR MAGAR NALLAH WATER TANK No. put to Tender Completion 32 DO Deposit RAM - 3 VKV, RAMKRISHNAGRAM AREA, POLICE TIKREY, DAS PARA VIDYASAGARPAL GOVT. PRIMARY SCHOOL SAITAN TIKRI, PANDEY BAZAAR, 1 NIT NO- R&M of different water pump sets under 33 DO 15/DB/ PHED/ E & M Sub Division attached with EE LI VS PALLY HELIPAD AREA GOVT. -

CAR NICOBAR ISLAND Sl.No
CAR NICOBAR ISLAND Sl.No. Particulars 31.12.2006 1. Area (Sq Km) 126.90 2. Census Villages (2001Census) 16 (i) Inhabited 16 1Mus 2 Teetop 3 Sawai 4 Arrong 5Kimois 6 Kakana 7IAF Camp 8 Malacca 9Perka 10 Tamaloo 11 Kinyuka 12 Chuckchucha 13 Tapoiming 14 Big Lapati (Jayanti) 15 Small Lapati 16 Kinmai (ii) Uninhabitted NIL 3. Revenue Villages NIL 4. Panchayat Bodies NIL 5. House Holds (2001 Census) 3296 6. Population (2001 Census) 20292 Male 10663 Female 9629 7. ST Population (2001 Census) 15899 Male 7914 Female 7985 8. Languages Spoken Nicobari & Hindi 9. Main Religion Hinduism, Christianity & Islam 10. Occupation – Main Workers (2001 Census) (i) Cultivators 24 (ii) Agricultural Labourers 9 (iii) Household Industries 2288 (iii) Other Workers 3671 11. Villages provided with piped water 16 supply 12. Health Service (a) Institutions (i) Hospital 1 (ii) Sub Centre 5 (iii) Dispensary 1 (b) Health Manpower (i) Doctors 10 (ii) Nurses/Midwives/LHVs 37 (iii) Para Medical Staff 60 (c) Bed Strength 113 13. Industries Industrial Centre 1 Industrial Estate Nil Industries Registered 13 54 ISLAND-WISE STATISTICAL OUTLINE - 2006 13. Civil Supplies (i) Fair Price Shops 13 (ii) Ration Cards Holder(APL+Temp) 4317 (iii) Quantity of Rice Allotted (MT) 283000 (iv) Quantity of Sugar Allotted (MT) 24000 (v) Quantity of Wheat Allotted (MT) -- 14. Education (a) Institutions (i) Primary School 6 (ii) Middle School 3 (iii) Secondary School 4 (iv) Senior Secondary School 4 (b) Enrollment (i) Primary School 183 (ii) Middle School 647 (iii) Secondary School 632 (iv) Senior Secondary School 1842 (c) Teaching staff (i) Primary School 23 (ii) Middle School 32 (iii) Secondary School 47 (iv) Senior Secondary School 49 15. -

International Union for Conservation of Nature and Natural Resources
INTERNATIONAL UNION FOR CONSERVATION OF NATURE AND NATURAL RESOURCES Report on Land Use in the ANDAMAN AND NICOBAR ISLANDS by D.N. McVean IUCN CONSULTANT Library CH - 1196 Gland With Financial Assistance from The Government of India and The United Nations Environmental Programme Morges, Switzerland Jwte, 1976 TABLE OF CONTENTS Introduction ••••••••••••••••••••••ct•••• .. •••••·••••••••••11:e•••••••••• 1 SuDID8.ry ••••••••••••••••••••••••••• 4 ••••••• ,. fl •• fl " M .............. 6 •• a • • 1 ENVIRONMENTAL Il!PACT ASSESSMENT ....... " .. " .......................... 2 Effect of de.forestation on climate • " • ll ............................ 2 Accelerated soil erosion ........... ....... ... .. .... ................ 3 Water supplies, perennial and seasonal ... " ....................... 5 Forestry ···•~41~••••11•••••···········••t-•••····················· 7 Agriculture and settlement ••••••••••....••••• , • • • • . • • • • • • • • • • • • • 9 Plantation agriculture ••••11•••·••!:ilf'• '!lr ••························· 11 Other development 12 ··············-~r.o••··················-····· CONSERVATION .......................... ., ...... ,_ ................... 14 Terrestrial habitats •••• S • e • I • IJ ... I ••• S e 4 I' ••• e ••• • ••••••••• I' ••••• 14 Marine habitats .............. ....... II. ....................... 17 Indigenous tribes • ' .. e • • llJo 1' • + "' • e .. + • • • • • • • • • ' ' • Ill- 4' .. t • • ... II 4 41 • •• • • 18 COMMEN'.i:S ON PREVIOUS REPORTS ...... ,.••••••••• ,.,. •••••••••••••••••••••• 41. 19 RECOMMENDATIONS -

Chapter 2 Introduction to the Geography and Geomorphology Of
Downloaded from http://mem.lyellcollection.org/ by guest on February 7, 2017 Chapter 2 Introduction to the geography and geomorphology of the Andaman–Nicobar Islands P. C. BANDOPADHYAY1* & A. CARTER2 1Department of Geology, University of Calcutta, 35 Ballygunge Circular Road, Kolkata-700019, India 2Department of Earth & Planetary Sciences, Birkbeck, University of London, London, UK *Correspondence: [email protected] Abstract: The geography and the geomorphology of the Andaman–Nicobar accretionary ridge (islands) is extremely varied, recording a complex interaction between tectonics, climate, eustacy and surface uplift and weathering processes. This chapter outlines the principal geographical features of this diverse group of islands. Gold Open Access: This article is published under the terms of the CC-BY 3.0 license The Andaman–Nicobar archipelago is the emergent part of a administrative headquarters of the Nicobar Group. Other long ridge which extends from the Arakan–Yoma ranges of islands of importance are Katchal, Camorta, Nancowry, Till- western Myanmar (Burma) in the north to Sumatra in the angchong, Chowra, Little Nicobar and Great Nicobar. The lat- south. To the east the archipelago is flanked by the Andaman ter is the largest covering 1045 km2. Indira Point on the south Sea and to the west by the Bay of Bengal (Fig. 1.1). A coast of Great Nicobar Island, named after the honorable Prime c. 160 km wide submarine channel running parallel to the Minister Smt Indira Gandhi of India, lies 147 km from the 108 N latitude between Car Nicobar and Little Andaman northern tip of Sumatra and is India’s southernmost point. -
Jandec2006.Pdf
Academy Journal VOLUME 58 NO 1 VICTIMS OF CRIME - NEED FOR PRO-ACTIVE ROLE BY THE 3 FUNCTIONARIES OF CRIMINAL JUSTICE SYSTEM Bag R K, Coordinator&Joint Director West Bengal Judicial Academy DOMESTIC VIOLENCE AND LAW 6 Bhawra V K, IPS, IGP Commando, Punjab FORENSIC HYPNOSIS 10 Chander Muktesh, IPS, Addl.Commissioner of Police Crime, Delhi TRAFFICKING IN PERSONS 14 Krishna Prasad K, IPS, IGP&Director, Addl. Director, APPA OUR BELOVED C.D.I. 20 Kumar Vijay, IPS (Retd.), Former DGP SCRB, West Bengal STRESS DIMENSIONS OF POLICE FIGHTING, TERRORISM, EXTREMISM 23 AND INSURGENCY Madana Mohan Madugula, & Dr. Raghunath Reddy, D. BETWEEN ART OF LIVING AND ART OF LEAVING 33 Mahesshwari A P, IPS, IGP, CRPF, Srinagar POLICE EXPECTATIONS AND FIELD REALITIES 37 Mohan Rao P (Dr.) POLICE REFORMS 40 Muhammad Bin Mahmood, IPS (Retd.),Former Ambassador to Saudi Arabia RECONCILING POLICE ORGANISATIONAL STRUCTURE AND WORK 42 CULTURE Patel Hasmukh, IPS, SP Bhavnagar, Gujarat A&N ISLANDS POLICE: THE FIRST RESPONDERS IN CAR NICOBAR 48 Porwal Vikram Kapali, Dy.SP/South Andaman Port Blair PLEA BARGAINING 53 Singh Pankaj Kumar, IPS, DIG, CBI CORRUPTION AND DEVELOPMENT 56 Sen Sankar, IPS (Retd.), Former Director NPA & Former DG, NHRC UNIFIED POLICE SERVICES CENTRE 61 Sharraf Umesh, IPS, CP, Vijayawada, Andhra Pradesh INNOVATIVE ORGANISATIONAL INITIATIVES IN PROMOTING 67 PEOPLE’S RESPECT FOR POLICE - A CHALLENGE BEFORE POLICE LEADERSHIP Thomas K V, Assistant Director, SIB Bhopal MP VICTIMS OF CRIME - NEED FOR PRO-ACTIVE ROLE BY THE FUNCTIONARIES OF CRIMINAL JUSTICE SYSTEM R K Bag INTRODUCTION victim of natural calamity and victim of state atrocity. -

Of Andaman and Nicobar Islands, Bay of Bengal
OCCASIONAL PAPER NO. 233 of Andaman and Nicobar Islands, Bay of Bengal D.R.K. SASTRY ZOOLOGICAL SURVEY OF INDIA OCCASIONAL PAPER NO. 233 RECORDS OF THE ZOOLOGICAL SURVEY OF INDIA Echinodermata of Andaman and Nicobar Islands, Bay of Bengal : An Annotated List D.R.K. SASTRY Zoo!ogicai Survey of India, Andaman and Nicobar Regional Station, Port Blair-744 102 Edited by the Director, Zoological Survey of India, Kolkata Zoological Survey of India Kolkata CITATION Sastry, D.R.K. 2005. Echinodermata of Andaman and Nicobar Islands, Bay of Bengal: An Annotated List, Rec. zoo/. Surv. India, Occ. Paper No. 233 : 1-207. (Published : Director, Zool. Surv. India, Kolkata) Published : March, 2005 ISBN 81-8171-063-0 © Govt. of India, 2005 ALL RIGHTS RESERVED • No part of this publication may be reproduced stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise without the prior permission of the publisher. • This book is sold subject to the condition that it shall not, by way of trade, be lent, resold hired out or otherwise disposed of without the publisher's consent, in an form of binding or cover other than that in which, it is published. • The correct price of this publication is the price printed on this page. Any revised price indicated by a rubber stamp or by a sticker or by any other means is incorrect and should be unacceptable. PRICE Indian : Rs. 350.00 Foreign : $ 25; £ 20 Published at the Publication Division by the Director Zoological Survey of India, 234/4, AJe Bose Road, 2nd MSO Building, 13th floor, Nizam Palace, Kolkata 700020 and Printed at Shiva Offset Press, Dehra Dun-248 001. -

October 2017 Smith's Giant Gecko (Gekko Smithii) from the Great
Project Update: October 2017 Smith's giant gecko (Gekko smithii) from the Great Nicobar Island Acknowledgements: I thank the Andaman and Nicobar Environmental Team (ANET) for facilitating field work for this project for a duration of 6 months, Department of Environment and Forests, Andaman and Nicobar Islands for providing permission to carry out this study and collect tissues for molecular laboratory work (Permit No.: CWLW/WL/134(A)/517), Andaman and Nicobar Administration for providing permission to carryout field work in Tribal Reserve Areas and the Police Department, A&N Islands for providing logistical support in remote locations. Objectives: 1. To identify diversity in gecko species and populations distributed on the Andaman and Nicobar islands 2. To recognise factors governing patterns of genetic diversity across space (dispersal ability, barriers of dispersal, isolation-by-distance, human mediated dispersal). 3. To assess evolutionary relationships of the endemic and human commensal lineages of geckos from the Andaman and Nicobar Islands and deduce bio- geographical affinities of these Islands. 4. To prioritise islands and species for conservation. Tasks, timeline and status: Task Timeline Status Permits for the study October 2016-January Complete Field data collection in the October2017 2016-May 2017 Complete A&N Islands Molecular laboratory work May 2017-August 2017 In progress Morphological data July-August 2017 In progress Preparinganalysis publications August- November 2017 In progress Designing and printing October 2017 Yet to begin education material Project final report November 2017 Yet to begin Summary of field data collection: We began field work on October 26th 2016 and completed this on May 3rd, 2017. -

Impact Assessment and Economic Benefits of Weather and Marine Services
Impact Assessment and Economic Benefits of Weather and Marine Services December 2010 National Council of Applied Economic Research (NCAER) Parisila Bhawan, 11, I.P. Estate New Delhi- 110 002, INDIA Tel: +91-11-2337 9861-63 Fax: +91-11-2337 0164 Website: www.ncaer.org copyright@2010 by the National Council of Applied Economic Research, New Delhi – 110 002. Preface The Ministry of Earth Sciences (MoES) was formed in 2006 from a merger of the India Meteorological Department (IMD), the National Centre for Medium Range Weather Forecasting (NCMRWF), the Indian Institute of Tropical Meteorology (IITM), Pune, Earth Risk Evaluation Centre (EREC), and the Department of Ocean Development. The Mission of the MoES is to provide the nation with forecasts of the monsoons and other weather/climate parameters, and information about ocean state, earthquakes, tsunamis and other phenomena related to earth systems through well-integrated programs. These services have significant economic and social benefits that are otherwise very difficult to quantify. The actual and potential benefits to the key stakeholders like individuals, firms, industry sectors and national bodies from state-of-the-art meteorological and related services are substantial and, till today, they are inadequately recognised and insufficiently exploited in India. NCAER was approached by the MoES to carry out a comprehensive study to understand the perspectives of the main stakeholders on the weather and marine services and estimate the economic and social benefits of these services provided by the MoES. However the MoES provides numerous services and the number of beneficiaries is large. This study has restricted to the main stakeholders, such as farmers and fishermen. -
Scanned Image
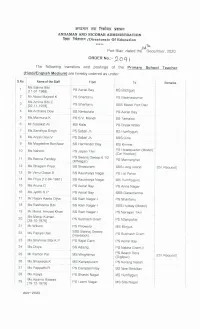
area war fala year ANDAMAN AND NICOBAR ADMINISTRATION fear Freee /Directorate Of Education kkk 24© lu Port Blair, dated the December, 2020 ORDER No.:- 2OQA i The following transfers and postings of the Primary School Teacher (Hindi/English Medium) are hereby ordered as under: S.No. Name ofthe Staff From | To Remarks Ms.Salma PS Aerial [11-01-1988]Bibi Bay MS Brichgunj Mr.Abdul Majeed K _ PS Shantanu PS Badmaspahar Ms.Amina Bibi.C | PS Shantanu [02-11-1978] SSS Model Port Blair _ | Ms.Archana Devi SS Nimbutala PS Aerial Bay Ms.Maimuna.K PS S.V. Mandir SS Tamaloo Mr.Sadakat Ali MS Kalsi PS Break Water Ms.Sandhya Singh PS Sabari Jn. MS Humfrygunj Ms. Anjali Devi.V PS Sabari Jn. SSS Girls | Ms.Magdeline Boniface SS Harminder Bay MS Kinmai PS Ms.Nahore PS Japan Tikri Headquarter (Model) (Car Nicobar) PS Swaraj Dweep 1/2 11 Ms.Beena Pandey PS (K/Nagar) 6 Mannarghat 12 Ms.Bhagam | Priya SS Sivapuram SSS Long Island [On Request] 13 Mr.Venu Gopal.B SS Kaushalya Nagar PS Lal Pahar 14 Ms.Priya [12-04-1981] SS Kaushalya Nagar MS Humfrygunj Ms.Aruna.G 15 PS Aerial Bay PS Anna Nagar | 16 Ms.Jyothi.S.P PS Aerial Bay SSS Garacharma “Mr 17 Rajoni Kanto Ojha SS Ram Nagar-| PS Shantanu Ms.Rasheena Bibi 18 SS Ram Nagar-| SSS Hutbay (Model) 19 Mr.Mohd. Amzad Khan SS Ram Nagar-| PS Narayan Tikri Ms.Manju Kumari 20 PS Subhash Gram PS [28-10-1976] Attampahar 21 Mr.Wilson PS Pillowolo MS Minyuk SSS Swaraj Dweep 22 Ms.Papiya Das PS Subhash (Havelock) Gram 23 Ms.Shahnaz Bibi.K.P PS Rajat Garh PS Aerial Bay | Ms. -

In Situ Studies of Astronomy of the Nicobarese Tribe of Nicobar Islands
In situ Studies of Astronomy of the Nicobarese Tribe of Nicobar Islands M. N. Vahia1, 2, Ganesh Halkare3, S. A. Awaradi4 and Kishore Menon2 1. Tata Institute of Fundamental Research, Dr Homi Bhabha Road, Navy Nagar, Colaba, Mumbai – 400 005, Maharashtra, India (Email: [email protected]) 2. Centre for Excellence in Basic Science, Vidya Nagari, Kalina, Santacruz (East), Mumbai – 400 098, Maharashtra, India 3. Indrayani Colony, Badnera Road, Amravati ‐ 444 607, Maharashtra, India 4. Andaman and Nicobar Tribal Research and Training Institute (ANTRI), Haddo – 744 102, Port Blair, Andaman and Nicobar Islands, India Received: 08 July 2018; Revised: 11 September 2018; Accepted: 25 October 2018 Heritage: Journal of Multidisciplinary Studies in Archaeology 6 (2018): 1013‐1038 Abstract: Sky is open for all to observe and it has fascinated humans from the time they first realised its existence. Humans have seen various objects in the patterns that the stars make. Most of the commonly held division of the sky has its roots in Babylonia about 3000 years before the Common Era. However, isolated tribal groups have not been a part of this narrative and they have interpreted the sky in different manner. Elsewhere (Vahia and Halkare 2017 and references therein) we have reported studies of the astronomy of various inland tribes in central India. Here we report the astronomical perspective of the tribes of the Nicobar Island. Isolated from the mainstream they have developed their own story about the astronomy and cosmogony of human race and the nature of Sun, Moon and stars. However, we find surprising lack of interest in using astronomy for navigational purposes.