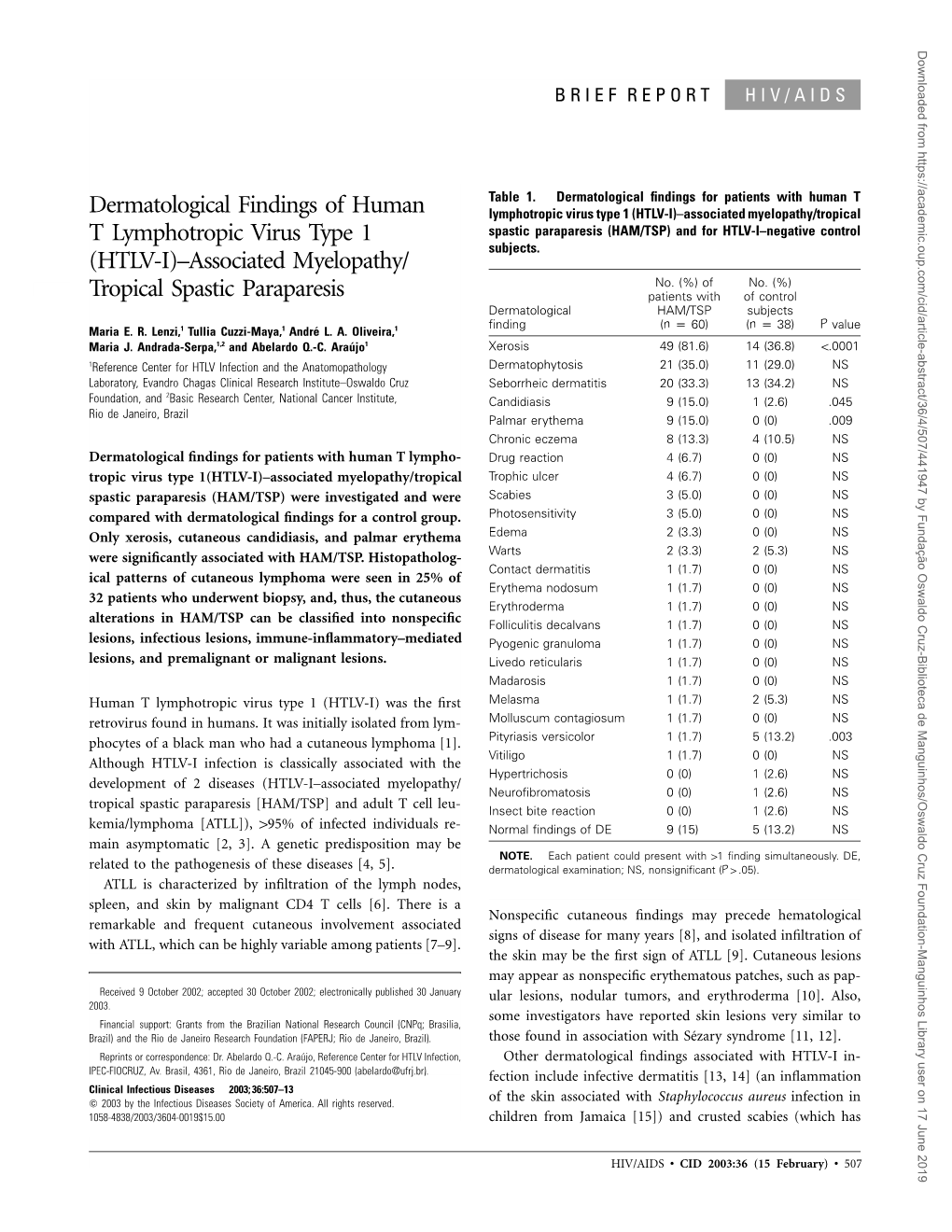
(HTLV-I)–Associated Myelopathy/ Tropical Spastic Paraparesis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dermatological Findings in Common Rheumatologic Diseases in Children
Available online at www.medicinescience.org Medicine Science ORIGINAL RESEARCH International Medical Journal Medicine Science 2019; ( ): Dermatological findings in common rheumatologic diseases in children 1Melike Kibar Ozturk ORCID:0000-0002-5757-8247 1Ilkin Zindanci ORCID:0000-0003-4354-9899 2Betul Sozeri ORCID:0000-0003-0358-6409 1Umraniye Training and Research Hospital, Department of Dermatology, Istanbul, Turkey. 2Umraniye Training and Research Hospital, Department of Child Rheumatology, Istanbul, Turkey Received 01 November 2018; Accepted 19 November 2018 Available online 21.01.2019 with doi:10.5455/medscience.2018.07.8966 Copyright © 2019 by authors and Medicine Science Publishing Inc. Abstract The aim of this study is to outline the common dermatological findings in pediatric rheumatologic diseases. A total of 45 patients, nineteen with juvenile idiopathic arthritis (JIA), eight with Familial Mediterranean Fever (FMF), six with scleroderma (SSc), seven with systemic lupus erythematosus (SLE), and five with dermatomyositis (DM) were included. Control group for JIA consisted of randomly chosen 19 healthy subjects of the same age and gender. The age, sex, duration of disease, site and type of lesions on skin, nails and scalp and systemic drug use were recorded. χ2 test was used. The most common skin findings in patients with psoriatic JIA were flexural psoriatic lesions, the most common nail findings were periungual desquamation and distal onycholysis, while the most common scalp findings were erythema and scaling. The most common skin finding in patients with oligoarthritis was photosensitivity, while the most common nail finding was periungual erythema, and the most common scalp findings were erythema and scaling. We saw urticarial rash, dermatographism, nail pitting and telogen effluvium in one patient with systemic arthritis; and photosensitivity, livedo reticularis and periungual erythema in another patient with RF-negative polyarthritis. -

Acroangiodermatitis (Pseudo-Kaposi's Sarcoma) in An
Revista5Vol89ingles_Layout 1 8/8/14 10:17 AM Página 792 792 DERMATOPATHOLOGY s Acroangiodermatitis (pseudo-Kaposi's sarcoma) in an HIV sero- positive patient with syphilis and hepatitis C virus coinfection: clinical and dermatopathological features* Fred Bernardes Filho1 Gustavo Martins2 José Augusto da Costa Nery1,3 Cecília Vianna de Andrade3,4 Bernard Kawa Kac1,5 DOI: http://dx.doi.org/10.1590/abd1806-4841.20143036 Abstract: Acroangiodermatitis is an angioproliferative disease usually related to chronic venous insufficiency, and it is considered a clinical and histological simulator of Kaposi's sarcoma (KS). Immunohistochemistry is the suit- able method to differentiate between these two entities. It reveals the following immunostaining profile: immunopositivity with anti-CD34 antibody is restricted to the vascular endothelium in acroangiodermatitis, and diffuse in the KS (endothelial cells and perivascular spindle cells); immunopositivity with anti-HHV-8 only in KS cases. We report the case of an HIV seropositive patient without apparent vascular disease, who presented viola- ceous and brownish erythematous lesions on the feet, and whose histopathology and immunohistochemistry indi- cated the diagnosis of acroangiodermatitis. Keywords: AIDS Serodiagnosis; Herpesvirus 8, human; Immunohistochemistry; Sarcoma, Kaposi; Syphilis, cutaneous INTRODUCTION Acroangiodermatitis is an unsual angioprolife- tantly with other manifestations or late in the course of rative disease related to chronic venous insufficiency, disease. The clinical presentation of KS is highly varia- arteriovenous malformations or fistulas, paralyzed ble, generally beginning with purplish or brownish, limbs, amputation stumps and thrombotic condi- erythematous, asymptomatic macules that later evolve tions.1,2 It is generally characterized by purpuric macu- into papules, plaques, nodules or tumor lesions.4,5 les, papules or plaques on the dorsum of the feet and Histopathologic distinction between acroangio- the malleolus. -

UC Davis Dermatology Online Journal
UC Davis Dermatology Online Journal Title Generalized linear IgA dermatosis with palmar involvement Permalink https://escholarship.org/uc/item/1s3402cj Journal Dermatology Online Journal, 21(9) Authors Norris, Ivy N Haeberle, M Tye Callen, Jeffrey P et al. Publication Date 2015 DOI 10.5070/D3219028674 License https://creativecommons.org/licenses/by-nc-nd/4.0/ 4.0 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Volume 21 Number September 2015 Case report Generalized linear IgA dermatosis with palmar involvement Ivy N Norris MD1, M Tye Haeberle MD2, Jeffrey P Callen MD2, Janine C Malone MD2 Dermatology Online Journal 21 (9): 1 1University of Louisville School of Medicine 2Division of Dermatology, Department of Medicine, University of Louisville School of Medicine, Louisville, Kentucky Correspondence: Dr. Tye Haeberle 3810 Springhurst Blvd Louisville, KY 40241 [email protected] Abstract Linear IgA bullous dermatosis (LABD) is a sub-epidermal blistering disorder characterized by deposition of IgA along the basement membrane zone (BMZ) as detected by immunofluorescence microscopy. The diagnosis is made by clinicopathologic correlation with immunofluorescence confirmation. Differentiation from other bullous dermatoses is important because therapeutic measures differ. Prompt initiation of the appropriate therapies can have a major impact on outcomes. We present three cases with prominent palmar involvement to alert the clinician of this potential physical exam finding and to consider LABD in the right context. Introduction Linear IgA bullous dermatosis (LABD) is a sub-epidermal blistering disorder characterized by deposition of IgA along the basement membrane zone (BMZ) as detected by immunofluorescence microscopy. Patients present most often with bullae mimicking bullous pemphigoid or with blisters that can have a herpetiform arrangement. -

Palmar Erythema and Hoarseness: an Unusual Clinical Presentation of Sarcoidosis
NOTABLE CASES NOTABLE CASES Palmar erythema and hoarseness: an unusual clinical presentation of sarcoidosis Ravinder P S Makkar, Surabhi Mukhopadhyay, Amitabh Monga, Anju Arora and Ajay K Gupta Palmar erythema is a very unusual manifestation of sarcoidosis. We report on a patient whose presenting features of sarcoidosis were palmar erythema and a hoarse voice. The diagnosis was confirmedThe Medical by palmar Journal of skin Australia biopsy ISSN: and 0025-729X the patient 20 Janu- responded well to treatment with prednisolone. (MJAary 2003; 2003 178178: 2 75-7675-76) ©The Medical Journal of Australia 2002 www.mja.com.au Notable Cases SARCOIDOSIS is a disease of unknown aetiology that can 1: Palmar erythema associated with sarcoidosis affect almost any organ of the body. Cutaneous involvement, occurring in up to 25% of cases of systemic sarcoidosis, is well recognised.1 However, palmar erythema is a very unusual skin manifestation of sarcoidosis — to our knowl- edge, it has been reported only once before in the literature.2 We describe a patient with palmar erythema and a hoarse voice who was subsequently shown to have sarcoidosis. Clinical record A 58-year-old man presented complaining of increasing hoarseness of voice of three weeks’ duration. The patient had also noticed increasing redness and a burning sensation over both palms. He had no history of any drug intake, fever, cough, breathlessness, chest pain, dysphagia, weight A: Diffuse erythematous macular rash seen on the palmar surface loss or anorexia. The patient was a non-smoker and did not (biopsy site arrowed). consume alcohol. On examination, he had a confluent, non-blanching, macular, erythematous rash on both palms (Box 1), but no other skin rash elsewhere on the body. -

40 Cutaneous Manifestations of Inflammatory Bowel Disease
40 Cutaneous manifestations of inflammatory bowel disease SCOTT W. BINDER Introduction Table 1. Cutaneous manifestations of Inflammatory bowel disease Cutaneous manifestations are common in inflamma Specific lesions tory bowel disease (IBD). In one study, the incidence Fissures and fistulas was reported to be as high as 34%. [1] However, some Oral manifestations (Crohn's disease) of the early studies included non-specific inflamma Metastatic Crohn's disease tory conditions such as urticaria, various maculo- papular eruptions, and pigmentary abnormalities, Reactive lesions Erythema nodosum some or all of which may be unrelated to the bowel Pyoderma gangrenosum disease. Other rigorous studies provide a more Aphthous ulcers reasonable estimate of cutaneous involvement in Vesiculopustular eruption patients with ulcerative colitis (UC) and Crohn's Pyoderma vegetans Necrotizing vasculitis disease (CD) (9-19%) [2]. Greenstein et aL, in an Cutaneous polyarteritis nodosa older study of 498 patients with CD, noted that cutaneous manifestations are more common when Miscellaneous associations the large intestine is involved [3]. Epidermolysis bullosa acquisita Mucocutaneous manifestations of IBD may be Clubbing Vitiligo classified as specific lesions, reactive lesions, and Acne fulminans miscellaneous associations (Table 1). For complete Psoriasis ness, cutaneous manifestations secondary to malab Vasculitis sorption [4, 5] or treatment may also be considered, Secondary amyloidosis but will not be treated in this text. Specific lesions refer to those lesions that are due to direct involve ment of the skin by the same disease process that aff'ects the gastrointestinal tract. This includes 8] for explication of the most current treatments of fissures, fistulas, and metastatic CD [2]. In contrast, the entities discussed herein. -

(12) United States Patent (10) Patent No.: US 7,359,748 B1 Drugge (45) Date of Patent: Apr
USOO7359748B1 (12) United States Patent (10) Patent No.: US 7,359,748 B1 Drugge (45) Date of Patent: Apr. 15, 2008 (54) APPARATUS FOR TOTAL IMMERSION 6,339,216 B1* 1/2002 Wake ..................... 250,214. A PHOTOGRAPHY 6,397,091 B2 * 5/2002 Diab et al. .................. 600,323 6,556,858 B1 * 4/2003 Zeman ............. ... 600,473 (76) Inventor: Rhett Drugge, 50 Glenbrook Rd., Suite 6,597,941 B2. T/2003 Fontenot et al. ............ 600/473 1C, Stamford, NH (US) 06902-2914 7,092,014 B1 8/2006 Li et al. .................. 348.218.1 (*) Notice: Subject to any disclaimer, the term of this k cited. by examiner patent is extended or adjusted under 35 Primary Examiner Daniel Robinson U.S.C. 154(b) by 802 days. (74) Attorney, Agent, or Firm—McCarter & English, LLP (21) Appl. No.: 09/625,712 (57) ABSTRACT (22) Filed: Jul. 26, 2000 Total Immersion Photography (TIP) is disclosed, preferably for the use of screening for various medical and cosmetic (51) Int. Cl. conditions. TIP, in a preferred embodiment, comprises an A6 IB 6/00 (2006.01) enclosed structure that may be sized in accordance with an (52) U.S. Cl. ....................................... 600/476; 600/477 entire person, or individual body parts. Disposed therein are (58) Field of Classification Search ................ 600/476, a plurality of imaging means which may gather a variety of 600/162,407, 477, 478,479, 480; A61 B 6/00 information, e.g., chemical, light, temperature, etc. In a See application file for complete search history. preferred embodiment, a computer and plurality of USB (56) References Cited hubs are used to remotely operate and control digital cam eras. -

Blanching Rashes
BLANCHING RASHES Facilitators Guide Author Aoife Fox (Edits by the DFTB Team) [email protected] Author Aoife Fox Duration 1-2h Facilitator level Senior trainee/ANP and above Learner level Junior trainee/Staff nurse and Senior trainee/ANP Equipment required None OUTLINE ● Pre-reading for learners ● Basics ● Case 1: Chicken Pox (15 min) ● Case 2: Roseola (15 min) ● Case 3: Scarlet fever (20 min) ● Case 4: Kawasaki disease (including advanced discussion) (25 min) ● Game ● Quiz ● 5 take home learning points PRE-READING FOR LEARNERS BMJ Best Practice - Evaluation of rash in children PEDS Cases - Viral Rashes in Children RCEM Learning - Common Childhood Exanthems American Academy of Dermatology - Viral exanthems 2 Infectious Non-infectious Blanching Blanching Staphylococcus scalded skin syndrome Sunburn Impetigo Eczema Bullous impetigo Urticaria Eczema hepeticum Atopic dermatitis Measles Acne vulgaris Glandular fever/infectious mononucleosis Ichthyosis vulgaris keratosis pilaris Hand foot and mouth disease Salmon patch Erythema infectiosum/Fifth disease Melasma Chickenpox (varicella zoster) Napkin rash Scabies Seborrhoea Tinea corporis Epidermolysis bullosa Tinea capitis Kawasaki disease Molluscum contagiosum Steven-Johnson syndrome Scarlet fever Steven-Johnson syndrome/toxic epi- Lyme disease dermal necrolysis Congenital syphilis Erythema multiforme Congenital rubella Erythema nodosum Herpes simplex Roseola (sixth disease) Non-blanching Epstein-Barr virus Port-wine stain Pityriasis rosea Henoch-Schoenlein purpura Idiopathic thrombocytopenia Acute leukaemia Haemolytic uremic syndrome Trauma Non-blanching Mechanical (e.g. coughing, vomiting – in Meningococcal rash distribution of superior vena cava) 3 BASE Key learning points Image: used with gratitude from Wikipedia.org Definitions/rash description: ● Macule: a flat area of colour change <1 cm in size (e.g., viral exanthem [such as measles and rubella], morbilliform drug eruption). -

Mallory Prelims 27/1/05 1:16 Pm Page I
Mallory Prelims 27/1/05 1:16 pm Page i Illustrated Manual of Pediatric Dermatology Mallory Prelims 27/1/05 1:16 pm Page ii Mallory Prelims 27/1/05 1:16 pm Page iii Illustrated Manual of Pediatric Dermatology Diagnosis and Management Susan Bayliss Mallory MD Professor of Internal Medicine/Division of Dermatology and Department of Pediatrics Washington University School of Medicine Director, Pediatric Dermatology St. Louis Children’s Hospital St. Louis, Missouri, USA Alanna Bree MD St. Louis University Director, Pediatric Dermatology Cardinal Glennon Children’s Hospital St. Louis, Missouri, USA Peggy Chern MD Department of Internal Medicine/Division of Dermatology and Department of Pediatrics Washington University School of Medicine St. Louis, Missouri, USA Mallory Prelims 27/1/05 1:16 pm Page iv © 2005 Taylor & Francis, an imprint of the Taylor & Francis Group First published in the United Kingdom in 2005 by Taylor & Francis, an imprint of the Taylor & Francis Group, 2 Park Square, Milton Park Abingdon, Oxon OX14 4RN, UK Tel: +44 (0) 20 7017 6000 Fax: +44 (0) 20 7017 6699 Website: www.tandf.co.uk All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior permission of the publisher or in accordance with the provisions of the Copyright, Designs and Patents Act 1988 or under the terms of any licence permitting limited copying issued by the Copyright Licensing Agency, 90 Tottenham Court Road, London W1P 0LP. Although every effort has been made to ensure that all owners of copyright material have been acknowledged in this publication, we would be glad to acknowledge in subsequent reprints or editions any omissions brought to our attention. -

Essential Clinical Skills in Pediatrics
Essential Clinical Skills in Pediatrics A Practical Guide to History Taking and Clinical Examination Anwar Qais Saadoon 123 Essential Clinical Skills in Pediatrics Anwar Qais Saadoon Essential Clinical Skills in Pediatrics A Practical Guide to History Taking and Clinical Examination Anwar Qais Saadoon Al-Sadr Teaching Hospital Basra Iraq ISBN 978-3-319-92425-0 ISBN 978-3-319-92426-7 (eBook) https://doi.org/10.1007/978-3-319-92426-7 Library of Congress Control Number: 2018947572 © Springer International Publishing AG, part of Springer Nature 2018 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. -

Clinical and Histopathological Spectrum of Toxic Erythema of Chemotherapy in Patients Who Have Undergone Allogeneic Hematopoietic Cell Transplantation
Hematol Oncol Stem Cell Ther (2019) 12, 19–25 Available at www.sciencedirect.com ScienceDirect journal homepage: www.elsevier.com/locate/hemonc ORIGINAL RESEARCH REPORT Clinical and histopathological spectrum of toxic erythema of chemotherapy in patients who have undergone allogeneic hematopoietic cell transplantation Manrup K. Hunjan a, Somaira Nowsheen b,c, Alvaro J. Ramos-Rodriguez d, Shahrukh K. Hashmi e, Alina G. Bridges f,g, Julia S. Lehman f,g, Rokea El-Azhary f,* a St Johns Institute of Dermatology, Guys and St Thomas’ Hospitals NHS Trust, UK b Mayo Clinic Medical Scientist Training Program, Mayo Clinic School of Medicine, Rochester, MN, USA c Mayo Clinic Graduate School of Biomedical Sciences, Mayo Clinic, Rochester, MN, USA d Department of Internal Medicine, Icahn School of Medicine at Mount Sinai West, New York, NY, USA e Department of Hematology and Oncology, Mayo Clinic, Rochester, MN, USA f Department of Dermatology, Mayo Clinic, Rochester, MN, USA g Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA Received 15 April 2018; received in revised form 17 August 2018; accepted 3 September 2018 Available online 20 September 2018 KEYWORDS Abstract Cancer; Objective/Background: Toxic erythema of chemotherapy (TEC) is a well-recognized adverse Capillary leak syndrome cutaneous reaction to chemotherapy. Similar to many skin diseases, the clinical presentations (CLS); may vary. Our objective is to expand on the typical and atypical clinical and histopathological Chemotherapy; Stem cell transplant; presentations of TEC. Toxic erythema of Methods: Forty patients with a diagnosis of TEC were included from 500 patients who had chemotherapy; undergone an allogeneic hematopoietic stem cell transplant. -

Vivian (Wai Chong) Wong, M.D., Ph.D., FAAD. Board Certified Dermatologist Curriculum Vitae
Vivian (Wai Chong) Wong, M.D., Ph.D., FAAD. Board Certified Dermatologist Curriculum Vitae Synopsis I have more than 10 years of experience in basic and clinical research in dermatology, pharmacology, and medical innovations. I am a board-certified dermatologist and I hold dual M.D. and Ph.D. degrees in Pharmacology. I joined Skin Wellness Physicians after a career as a faculty member at the Department of Dermatology at Harvard Medical School and the director of hair loss clinic. In addition to seeing patients at our Naples, East Naples and Marco Island locations, I serve as clinical instructor for the internal medicine and transitional residency programs at Naples Community Hospital. I also work as an independent consultant for medical diagnostic, therapeutic and technology companies. I have collaborated with researchers in North America, Europe and Asia and authored over 250 articles to date on important topics such as melanoma, zika virus, and cutaneous lymphoma. I am a renowned expert on hair loss and I have been interviewed by the Boston Magazine, Boston25 News and QuantiaMD. I have presented at more than 50 international and domestic conferences, and received more than 40 awards for my contributions. Positions 10/2020- Present Dermatologist, Skin Wellness Physicians Naples, Florida 9/2018 – 9/2020 Attending dermatologist, Harvard Medical Faculty Physicians Department of Dermatology, Beth Israel Deaconess Medical Center, Boston Academic appointment: 12/2020- Present Clinical Instructor, Dermatology Internal Medicine Residency Program, Naples Community Hospital Transitional Residency Program, Naples Community Hospital 9/2018 – 9/2020 Core teaching faculty Department of Dermatology, Harvard Medical School, Boston Industry experience: 2014 - present VisualDx®, New York. -

Vol-8 (2) 2007 BSM.Pmd
J MEDICINE 2007; 8 : 44-48 CUTANEOUS MANIFESTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS NAHID PARVEEN1, DIPAK KUMAR DAS2, F.R.M. MAHBUBUL HAQUE3, MAHAMUDUN NABI MOHAMMAD MOMTAZUL HAQUE4 Abstract: Systemic lupus erythematosus (LE) is a heterogeneous, multisystem, autoimmune disease characterized by the production of auto-antibodies against several cell constituents. The skin is one of the target organs most variably affected by the disease can be yield valuable diagnostic & prognostic information. The present study was conducted to evaluate cutaneous manifestations of SLE in Bangladeshi patients. 100 cases of SLE were collected from the Department of Dermatology, BSMMU, Dhaka. The diagnosis was based on American Rheumatism Association Criteria. Cutaneous changes were recorded on a predevised pro forma. LE specific cutaneous changes noted were: Malar rash or butterfly rash (70.0%), maculopapular rash (19.0%), discoid rash (10.0%), and bullous LE (10.0%). Non specific LE lesions noted were: Photosensitivity (75.0%), alopecia (47.0%), oral mucosal lesion (34.0%), hyperpigmentation (20.0%), nail change (15.0%), Raynauds phenomenon (12.0%), Palmar erythema, genital lesion, periungual talangiectesia, leg ulcers, livedo reticularis, erythema multiform were rare. Systemic lupus erythematosus is a multisystem disease that predominantly affects women. Cutaneous lesions are the most important diagnostic tools as reflected by the fact that they account for four of the 11 revised American Rheumatism Association criteria of SLE. The pattern of skin changes may vary from place to place. Key Words: SLE, LE specific and non specific cutaneous lesions Introduction: systemic lupus erythematosus.2,7 There is a tremendous Systemic lupus erythematosus (SLE) is a variability and diversity in the type of involvement heterogeneous, multisystem, autoimmune disease ranging from classical butterfly rash and atrophic characterized by the production of auto-antibodies hyperkeratotic lesions of discoid lupus to bullae, alopecia against several cell constituents.