Ttts/Taps/Tops
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Human Chimera: Legal Problems Arising from Individuals with Multiple Types of Dna
Seton Hall University eRepository @ Seton Hall Law School Student Scholarship Seton Hall Law 5-2-2014 The umH an Chimera: Legal Problems Arising From Individuals with Multiple Types of DNA Robert Russell Granzen Follow this and additional works at: https://scholarship.shu.edu/student_scholarship Recommended Citation Granzen, Robert Russell, "The umH an Chimera: Legal Problems Arising From Individuals with Multiple Types of DNA" (2014). Law School Student Scholarship. 485. https://scholarship.shu.edu/student_scholarship/485 THE HUMAN CHIMERA: LEGAL PROBLEMS ARISING FROM INDIVIDUALS WITH MULTIPLE TYPES OF DNA Robert Granzen INTRODUCTION Science continually changes, and with it our understanding of the human body. While some scientific developments are limited in scope, others have widespread effects. Scientists have just recently begun understanding the range of effects chimerism in humans can have. Chimerism, originally associated with hermaphrodites having both male and female sexual organs, is much more common than originally thought. As chimerism becomes more common, so do individuals with separate and distinct deoxyribonucleic acid (DNA) strands in their bodies. Most individuals are unaware of their chimeric genetic code and most will likely never know. Because of the inherent difficulty of testing for chimerism, many problems are presented to legal system. Part I of this article will begin with the history of human chimeras. The section will then describe the ways in which chimeras are formed. The section will discuss the most common form of chimerism in humans--fetal cell microchimerism (FMC). FMC occurs when cells are transferred from baby to mother or mother to baby via the umbilical cord.1 Studies have shown that mothers may keep cells from their children for years after giving birth.2 Moreover, cells can be exchanged between twins while inside the uterus.3 Secondly, the section will describe the process of embryo fusion, which can cause tetragametic chimerism. -

Meconium Peritonitis
ISSN: 2377-9004 Agrawal et al. Obstet Gynecol Cases Rev 2020, 7:180 DOI: 10.23937/2377-9004/1410180 Volume 6 | Issue 5 Obstetrics and Open Access Gynaecology Cases - Reviews CASE REPORT Meconium Peritonitis: In Utero Diagnosis of a Rare Clinical Entity and Postnatal Outcome Sarita Agrawal, MD, FICOG, FIAMS, FCGP1, Arpana Verma, MS2*, Sarita Rajbhar, MS3, Pushpawati Thakur, MD4, Loukya Kodumuri, MBBS5 and Swati Kumari, MS, FNB6 1Professor and Head of Department, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 2Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 3Assistant Professor, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 4 Check for Associate Professor, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, updates Raipur, Chhattisgarh, India 5Post Graduate Student, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 6Sonologist and Fetal Medicine Expert, Shivam Fetomed and Spine Centre, Raipur, Chhattisgarh, India *Corresponding author: Arpana Verma, MS, Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, V.V-18, Parthivi Province, Near Salasar Greens, Sarona, Raipur, Chhattisgarh - 492099, India, Tel: 9741412716; 6260334337 Abstract done for immune and non-immune hydrops and was found to be negative. One week later, a repeat ultrasound was done Objective: To present an unusual case of meconium peri- which showed moderate fetal ascites with few areas of calci- tonitis diagnosed during prenatal period and its postnatal fication in the bowel loops and prominent inferior vena cava, outcome. -

Association Between First-Trimester Intrauterine Hematoma and Twin Pregnancy Outcomes: a Retrospective Cohort Study
Association Between First-Trimester Intrauterine Hematoma and Twin Pregnancy Outcomes: A Retrospective Cohort Study Wanqing Ji Guangzhou Women and Children's Medical Center Jie Zheng Guangzhou Women and Children's Medical Center Weidong Li Guangzhou Women and Children's Medical Center Fang Guo Guangzhou Women and Children's Medical Center Bo Hou Third Aliated Hospital of Sun Yat-Sen University Ping He ( [email protected] ) Guangzhou Women and Children's Medical Center https://orcid.org/0000-0002-6551-8578 Research article Keywords: intrauterine hematoma, twin gestation, rst trimester, miscarriage, vanishing twin syndrome Posted Date: September 21st, 2020 DOI: https://doi.org/10.21203/rs.3.rs-75567/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Version of Record: A version of this preprint was published on January 11th, 2021. See the published version at https://doi.org/10.1186/s12884-020-03528-0. 1 Title page 2 Association between first-trimester intrauterine hematoma and twin pregnancy 3 outcomes: A retrospective cohort study 4 Wanqing Ji1,Ϯ , jie Zheng1,Ϯ, Weidong Li 2,Ϯ, Fang Guo1, , Ping He1,* Bo Hou3,* 5 1Department of Obstetrics, Guangzhou Women and Children’s Medical Center, Guangzhou Medical 6 University, Guangzhou, 510623,China. 7 2Department of Woman and Child Health Information Guangzhou Women and Children’s Medical 8 Center, Guangzhou Medical University, Guangzhou, 510623,China. 9 3Departments of Neurosurgery, The Third Affiliated Hospital, Sun Yat-sen University, Guangzhou, 10 Guangdong province, 510630, China.E-mail: [email protected] 11 *Correspondence address. Ping He, Guangzhou Women and Children’s Medical Center, Guangzhou 12 Medical University, Guangzhou, Guangdong province, 510623, China.Fax number: 86-20-8717 6790 13 E-mail: [email protected] 14 Bo Hou , Departments of Neurosurgery, The Third Affiliated Hospital, Sun Yat-sen University, 15 Guangzhou, Guangdong province, 510630, China. -

CDC Having Healthy Babies One at a Time
HAVING HEALTHY BABIES ONE AT A TIME Why are we worried about twin pregnancies? We know that you are ready to start or add to your family. You may be concerned about your chances of having a baby using in vitro fertilization (IVF) or how much cycles of IVF cost. These concerns are common and may lead you to think about transferring more than one embryo during your IVF procedure. However, transferring more than one embryo increases your chances of having twins or more. Twin pregnancy is risky for baby and mother, whether or not IVF is used. Some of these risks include: Almost 3 out of 5 Twin babies are more likely to be stillborn, twin babies are born preterm, or at less than experience neonatal death, have birth defects of 37 weeks of pregnancy. Twin babies are nearly the brain, heart, face, limbs, muscles, or digestive 6 times as likely to be born preterm as system, and have autism than single babies. single babies. Almost 1 out of 10 About 1 out of 4 women carrying twins gets pregnancy-related twin babies are admitted to the neonatal high blood pressure. Women carrying twins intensive care unit (NICU). Twin babies are are twice as likely to get pregnancy-related high more than 5 times as likely to be admitted to the blood pressure as women carrying single babies. NICU as single babies. Almost 1 out of 20 About 7 out of 1,000 women carrying twins gets gestational diabetes. twin babies have cerebral palsy. Twin babies are Women carrying twins are 1.5 times as likely to get more than 4 times as likely to have cerebral palsy gestational diabetes as women carrying as single babies. -

Subcutaneous Emphysema, Pneumomediastinum, Pneumoretroperitoneum, and Pneumoscrotum: Unusual Complications of Acute Perforated Diverticulitis
Hindawi Publishing Corporation Case Reports in Radiology Volume 2014, Article ID 431563, 5 pages http://dx.doi.org/10.1155/2014/431563 Case Report Subcutaneous Emphysema, Pneumomediastinum, Pneumoretroperitoneum, and Pneumoscrotum: Unusual Complications of Acute Perforated Diverticulitis S. Fosi, V. Giuricin, V. Girardi, E. Di Caprera, E. Costanzo, R. Di Trapano, and G. Simonetti Department of Diagnostic Imaging, Molecular Imaging, Interventional Radiology and Radiation Therapy, University Hospital Tor Vergata, Viale Oxford 81, 00133 Rome, Italy Correspondence should be addressed to E. Di Caprera; [email protected] Received 11 April 2014; Accepted 7 July 2014; Published 17 July 2014 Academic Editor: Salah D. Qanadli Copyright © 2014 S. Fosi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Pneumomediastinum, and subcutaneous emphysema usually result from spontaneous alveolar wall rupture and, far less commonly, from disruption of the upper airways or gastrointestinal tract. Subcutaneous neck emphysema, pneumomediastinum, and retropneumoperitoneum caused by nontraumatic perforations of the colon have been infrequently reported. The main symptoms of spontaneous subcutaneous emphysema are swelling and crepitus over the involved site; further clinical findings in case of subcutaneous cervical and mediastinal emphysema can be neck and chest pain and dyspnea. Radiological imaging plays an important role to achieve the correct diagnosis and extension of the disease. We present a quite rare case of spontaneous subcutaneous cervical emphysema, pneumomediastinum, and pneumoretroperitoneum due to perforation of an occult sigmoid diverticulum. Abdomen ultrasound, chest X-rays, and computer tomography (CT) were performed to evaluate the free gas extension and to identify potential sources of extravasating gas. -

Association Between Chorionicity and Preterm Birth in Twin Pregnancies: a Systematic Review Involving 29 864 Twin Pregnancies
DOI: 10.1111/1471-0528.16479 Systematic Review www.bjog.org Association between chorionicity and preterm birth in twin pregnancies: a systematic review involving 29 864 twin pregnancies S Marleen,a,b C Dias,b R Nandasena,b R MacGregor,c J Allotey,d J Aquilina,c A Khalil,e,f S Thangaratinamg a Barts Research Centre for Women’s Health (BARC), Barts and the London School of Medicine and Dentistry, Queen Mary University of London, London, UK b Sri Jayewardenepura Postgraduate Teaching Hospital, Nugegoda, Sri Lanka c Royal London Hospital, Barts Health NHS Trust, London, UK d Institute of Applied Health Research, University of Birmingham, Birmingham, UK e St George’s University Hospitals NHS Foundation Trust, London, UK f Molecular and Clinical Sciences Research Institute, St George’s Medical School, University of London, London, UK g World Health Organization (WHO) Collaborating Centre for Global Women’s Health, Institute of Metabolism and Systems Research, University of Birmingham, Birmingham, UK Correspondence: S Marleen, Barts Research Centre for Women’s Health (BARC), Barts and the London School of Medicine and Dentistry, Queen Mary University of London, Mile End Road, London E1 4NS, UK. Email: [email protected] Accepted 7 August 2020. Published Online 7 October 2020. Background The perinatal mortality and morbidity among twins I2 = 46%, OR 1.55, 95% CI 1.27–1.89 I2 = 68%, OR 1.47, 95% CI vary by chorionicity. Although it is considered that 1.27–1.69, I2 = 60%, OR 1.66, 95% CI 1.43–1.93, I2 = 65%, monochorionicity is associated with an increased risk of preterm respectively). -

Consensus Guidelines for Partial Exchange Transfusion for Polycythemia in Neonates UCSF (NC)2 (Northern California Neonatal Consortium)
Consensus Guidelines for Partial Exchange Transfusion for Polycythemia in Neonates UCSF (NC)2 (Northern California Neonatal Consortium) Executive summary Objectives • Standardize the approach to screening and management of polycythemia in infants ≥ 34 weeks gestation using current practice standards and best available evidence • Improve quality and safety of care for neonates ≥ 34 weeks GA with possible polycythemia; specifically: o Improve recognition of infants showing symptoms of polycythemia o Decrease unnecessary screening o Provide recommendations on how to perform partial exchange transfusion safely and effectively o Decrease morbidity associated with unnecessary partial exchange transfusions Recommendations • Who to Screen o Asymptomatic patients should not be routinely screened regardless of risk factors o Only screen symptomatic patients for polycythemia • Who Should Receive Partial Exchange Transfusion o Do NOT perform PET in asymptomatic infant with Hct <=75% o Consider PET in infants with Hct >65% who are demonstrating signs listed in Section A or B on page 3 o Consider PET in asymptomatic infants with Hct >75%, but note there is minimal data for benefit of PET in asymptomatic infants. • Timing of Partial Exchange Transfusion o PET should be performed as soon as possible in symptomatic infants Methods This guideline was developed through local consensus based on published evidence and expert opinion as part of the UCSF Northern California Neonatal Consortium. Metrics Plan UCSF NC2 (Northern California Neonatology Consortium). -

Pre-Eclampsia/Eclampsia in Twin Pregnancies A
J Med Genet: first published as 10.1136/jmg.13.3.208 on 1 June 1976. Downloaded from Journal of Medical Genetics (1976). 13, 208-211. Pre-eclampsia/eclampsia in twin pregnancies A. McFARLANE and J. S. SCOTT From the Department of Obstetrics and Gynaecology (Leeds Maternity Hospital), University of Leeds, 17 Springfield Mount, Leeds LS2 9NG Summary. A study of 1045 twin gestations with regard to known or likely zygosity and the incidence of pre-eclampsia/eclampsia failed to reveal differences between known dizygous twins and like-sex 'presumed' and 'estimated' monozygous twins except in the 'estimated' data for multigravidae. There was a threefold in- crease in the incidence for twins as opposed to singleton pregnancies. These results are discussed in relation to increased conceptus-mother antigenic differences. It is suggested that the risk of gestosis in twin pregnancy involves more than a summa- tion ofthat operating in two singleton pregnancies. It has been suggested that genetic incompatibility Pregnancies were classified according to definitions given between mother and fetus may be a factor in the below. aetiology of pre-eclampsia (Penrose, 1946; Kalmus, 1946; Platt, Stewart, and Emery, 1958). Epidemio- A. Hypertension status logical evidence has been provided by Stevenson et (1) Mildpre-eclampsia-a basal blood pressure of 120/ 80 mm Hg or less recorded before 24 weeks' gestation, al (1971) in a study of consanguineous marriages in followed by a rise to 140/90 mm Hg or more on at least the Middle East. They also recorded twin data two occasions recorded in the antenatal ward, clinic which pointed to a higher incidence of toxaemia in readings being discounted, together with oedema and unlike-sex as opposed to like-sex twin pregnancies. -

CDHO Advisory Polycythemia, 2018-11-09
CDHO Advisory | P olycythemia COLLEGE OF DENTAL HYGIENISTS OF ONTARIO ADVISORY ADVISORY TITLE Use of the dental hygiene interventions of scaling of teeth and root planing including curetting surrounding tissue, orthodontic and restorative practices, and other invasive interventions for persons1 with polycythemia. ADVISORY STATUS Cite as College of Dental Hygienists of Ontario, CDHO Advisory Polycythemia, 2018-11-09 INTERVENTIONS AND PRACTICES CONSIDERED Scaling of teeth and root planing including curetting surrounding tissue, orthodontic and restorative practices, and other invasive interventions (“the Procedures”). SCOPE DISEASE/CONDITION(S)/PROCEDURE(S) Polycythemia INTENDED USERS Advanced practice nurses Nurses Dental assistants Patients/clients Dental hygienists Pharmacists Dentists Physicians Denturists Public health departments Dieticians Regulatory bodies Health professional students ADVISORY OBJECTIVE(S) To guide dental hygienists at the point of care relative to the use of the Procedures for persons who have polycythemia, chiefly as follows. 1. Understanding the medical condition. 2. Sourcing medications information. 3. Taking the medical and medications history. 4. Identifying and contacting the most appropriate healthcare provider(s) for medical advice. 1 Persons includes young persons and children Page | 1 CDHO Advisory | P olycythemia 5. Understanding and taking appropriate precautions prior to and during the Procedures proposed. 6. Deciding when and when not to proceed with the Procedures proposed. 7. Dealing with adverse events arising during the Procedures. 8. Keeping records. 9. Advising the patient/client. TARGET POPULATION Child (2 to 12 years) Adolescent (13 to 18 years) Adult (19 to 44 years) Middle Age (45 to 64 years) Aged (65 to 79 years) Aged 80 and over Male Female Parents, guardians, and family caregivers of children, young persons and adults with polycythemia. -

CASE REPORT CASE CASE R Imaging Findings of Meconium
CASE REPORT CASE REPORT Imaging findings of meconium peritonitis Logeshini Naidoo, MB ChB, FCRad (Diag) SA Helen Joseph and Coronation Hospitals, Johannesburg Introduction Meconium peritonitis results from intrauterine gastrointestinal perfora- tion, and can occur as early as the second trimester.1 Meconium extrudes into the peritoneal cavity, inciting an intense fibroplastic reaction that results in intra-abdominal calcifications.2 It is a rare condition occurring in 1 in 35 000 pregnant women.3 The clinical and radiological manifestations depend on whether the bowel perforation seals off in utero in the neonatal period or remains patent.3 Accordingly, the radiological spectra range from the incidental demonstration of diffuse intra-abdominal calcifications to meconium ascites (free meconium in the peritoneal cavity), meconium pseudocysts (walled-off meconium concentrations), and meconium hydrocoeles. Meconium has also been reported in the thoracic cavity (via diaphrag- matic hernias) and in the pelvic soft tissues.4 Antenatal ultrasound allows early detection of the condition, demonstrating free fluid, hydrocoeles and echogenic foci representing intraperitoneal calcifications.5 In the newborn, plain abdominal radiographs demonstrating calcifications and/or ascites are sufficient for diagnosis.1 Postnatal ultrasound is reserved for atypical presentations and can exclude intra-abdominal masses.1 Although computed tomography (CT) was used as an ancillary tool in the case report described below, it is unnecessary, thus negating the need for radiation exposure and expenditure of time. Fig. 1. Supine abdominal X-ray revealing a massively distended abdomen with poor lung capacities. The bulging flanks and central The imaging findings in a newborn with an ongoing bowel perfora- floating bowel loops indicate ascites. -
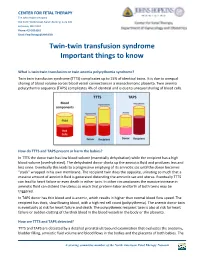
Twin to Twin Transfusion Syndrome (TTTS)
CENTER FOR FETAL THERAPY The Johns Hopkins Hospital 600 North Wolfe Street, Nelson Building, Suite 228 Baltimore, MD 21287 Phone: 410 502 6561 Email: [email protected] Twin-twin transfusion syndrome Important things to know What is twin-twin transfusion or twin anemia polycythemia syndrome? Twin twin transfusion syndrome (TTTS) complicates up to 15% of identical twins. It is due to unequal sharing of blood volume across blood vessel connections in a monochorionic placenta. Twin anemia polycythemia sequence (TAPS) complicates 4% of identical and is due to unequal sharing of blood cells. How do TTTS and TAPS present or harm the babies? In TTTS the donor twin has low blood volume (essentially dehydration) while the recipient has a high blood volume (overhydrated). The dehydrated donor drinks up the amniotic fluid and produces less and less urine. Eventually this leads to a progressive emptying of its amniotic sac until the donor becomes “stuck” wrapped in his own membrane. The recipient twin does the opposite, urinating so much that a massive amount of amniotic fluid is generated distending the amniotic sac and uterus. Eventually TTTS can lead to heart failure or even death in either twin. In other circumstances the massive increase in amniotic fluid can distend the uterus so much that preterm labor and birth of both twins may be triggered. In TAPS donor has thin blood and is anemic, which results in higher than normal blood flow speed. The recipient has thick, slow flowing blood, with a high red cell count (polycythemia). The anemic donor twin is eventually at risk for heart failure and death. -

Fetal Meconium Peritonitis Associated with Prenatal Methamphetamine Exposure
W.J. Yang, et al ■ SHORT COMMUNICATION ■ FETAL MECONIUM PERITONITIS ASSOCIATED WITH PRENATAL METHAMPHETAMINE EXPOSURE Wen-Jui Yang1, Chie-Pein Chen1,2*, Chen-Yu Chen1, Kuo-Gon Wang1, Tsung-Hsien Su1,2 1Department of Obstetrics and Gynecology, Mackay Memorial Hospital, and 2Mackay Medicine, Nursing and Management College, Taipei, Taiwan. SUMMARY Objective: In roughly 50% of all patients with meconium peritonitis, there is no evidence of primary obstruction of the bowel. We report a case of maternal methamphetamine and heroin abuse complicated by fetal meconium pseudocyst without a definite intestinal obstructive lesion. We discuss the correlation between the presence of meconium peritonitis and prenatal exposure to methamphetamine. Case Report: A 19-year-old, gravida 2, para 0, abortus 1, woman had abused illegal drugs, including methamphetamine and intravenous heroin. Suffering from withdrawal symptoms, she was taken to a shelter where she was diagnosed with a pregnancy of 26 weeks’ gestation. The patient underwent cesarean section at 34 weeks due to preterm labor and fetal malpresentation. A boy weighing 2,474 g was born, but had to be intubated and admitted to the intensive care unit because of a distended abdomen and respiratory distress. A laparotomy performed on the second day of life revealed a large calcified pseudocyst associated with two perforations of the distal jejunum. A segmental resection of the jejunum with primary anastomosis was performed. The infant recovered well after the operation and was discharged 65 days after birth. Conclusion: Since methamphetamine is a powerful _-adrenergic stimulant and induces the release of catecholamines from adrenergic synapses, it can cause powerful vessel constriction.