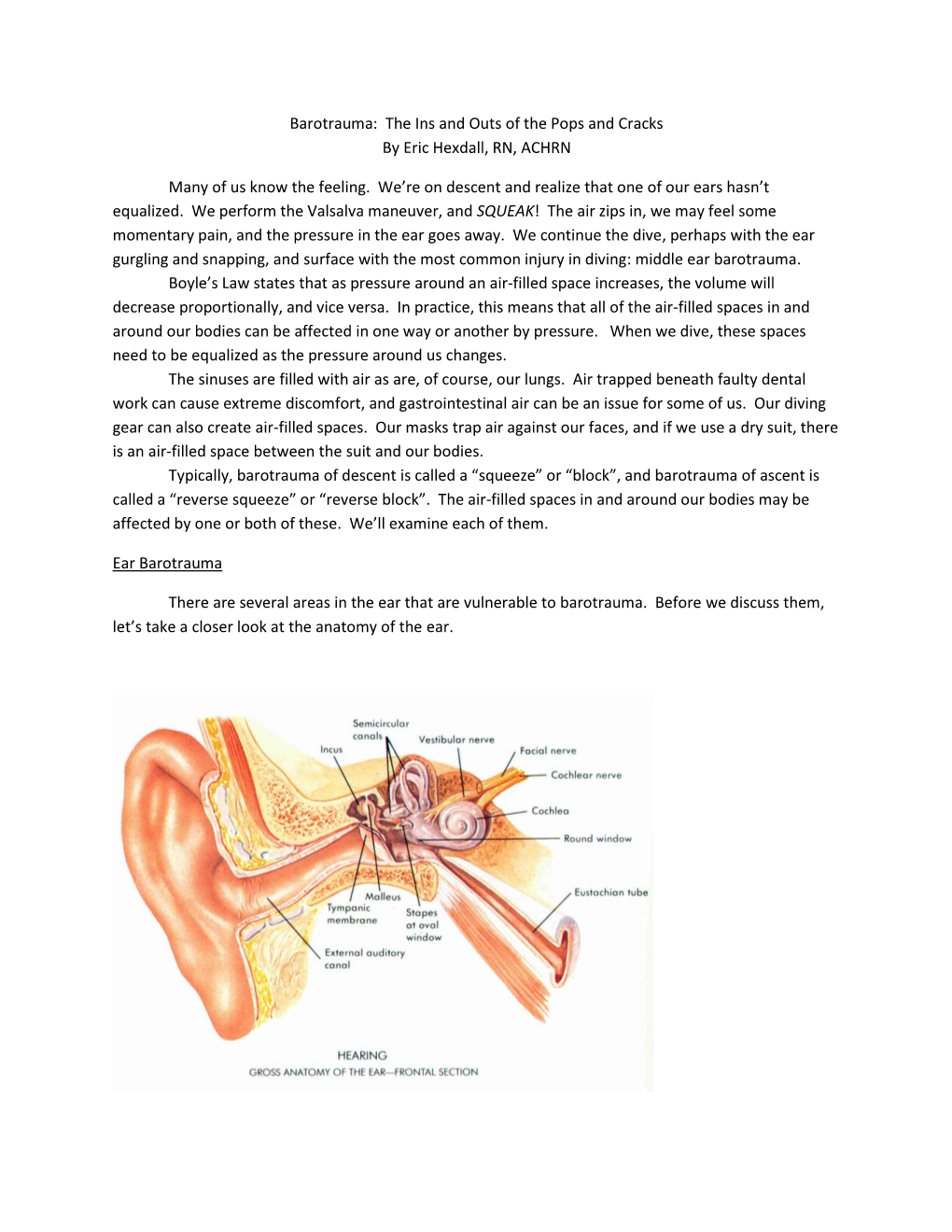
Barotrauma: the Ins and Outs of the Pops and Cracks by Eric Hexdall, RN, ACHRN
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Course Description
Instructor: Walter W Lancaster II Off Campus phone: 951-351-1445 x204 Dept phone: NA Cell phone: 951-312-2589 Department of Health and Exercise Science e-mail: [email protected] Spring Quarter, 2016 Alternate e-mail: [email protected] Off Campus Office: La Sierra Academy Office Hours: M-Th 8am – 4pm Consultations by appointment PEAC 106 Scuba Diving Walter Lancaster Location: Health and Exercise Science Classroom 1 (or other assigned instructional locaton) & Pool Tuesdays 6:30pm ~ 9:45pm I. COURSE DESCRIPTION: A. Bulletin Course Description: Course Description Basic SCUBA Diver is an entry-level course for people who have not been previously certified to SCUBA dive, and provides a comprehensive overview of basic concepts that are required to dive safely. Topics include diving equipment, diving physiology, dive planing, environmental considerations, and recognizing and managing risks associated with Open Water diving. Participants who successfully complete the classroom and pool work will qualify for an Open Water certification experience, which must be completed if the student wishes to become a certified diver. Successful completion of the Open Water experience will result in an industry recognized and accepted certification at the level of Basic SCUBA Diver through the National Assocaiton of Underwater Instructors (NAUI). All attendees must be age 16 or older. Students must be able to demonstrate a 10-minute swim/float in water too deep to stand in without the use of swim aids, complete a 200 meter/yard continuous surface swim and demonstrate an underwater (single breath) free dive for a horizontal minimum distance of 25 yards. B. Instructional Materials: Use of the recommended text and Comprehesive Resource Notebook is made available to all students as part of the comprehensive Lab Fee. -
Hyperbaric Oxygen Therapy in Dermatology
MILITARY DERMATOLOGY IN PARTNERSHIP WITH THE ASSOCIATION OF MILITARY DERMATOLOGISTS Hyperbaric Oxygen Therapy in Dermatology Jonathan P. Jeter, MD; Emily B. Wong, MD Overview of HOT PRACTICE POINTS Hyperbaric oxygen therapy involves sitting or lying in a • Hyperbaric oxygen therapy can be considered for special chamber that allows for controlled levels of oxygen the treatment of failing cutaneous grafts and flaps, (O2) at increased atmospheric pressure, which specifically chronic ulcerations caused by vasculitis or autoim- involves breathing near 100% O2 while inside a mono- mune disorders, and vascular compromise, including place or multiplace chamber5 that is pressurized to greater cutaneous ischemia caused by fillers. than sea level pressure (≥1.4 atmosphere absolute).2 • Hyperbaric oxygen therapy involves 1- to 2-hour treat- A monoplace chamber is designed to treat a single ments, 5 days a week, for as long as 1 month. person (Figure 1);copy a multiplace chamber (Figure 2) accom- 5,6 • Hyperbaric oxygen therapy is safe and well-tolerated, modates as many as 5 to 25 patients. The chambers with few contraindications. The sooner therapy is also accommodate hospital beds and medical attendants, started, the greater the potential for benefit. if needed. Hyperbaric O2 is inhaled through a mask, a tight-fitting hood, or an endotracheal tube, depending on notthe patient’s status.7 Treatment ranges from only 1 or Hyperbaric oxygen therapy (HOT) is a potentially useful technique for 2 iterations for acute conditions to 30 sessions or more for certain dermatologic conditions. We review its indications, dermato- chronic conditions. Individual sessions last 45 minutes to logic applications, and potential complications. -

Job Hazard Analysis
Identifying and Evaluating Hazards in Research Laboratories Guidelines developed by the Hazards Identification and Evaluation Task Force of the American Chemical Society’s Committee on Chemical Safety Copyright 2013 American Chemical Society Table of Contents FOREWORD ................................................................................................................................................... 3 ACKNOWLEDGEMENTS ................................................................................................................................. 5 Task Force Members ..................................................................................................................................... 6 1. SCOPE AND APPLICATION ..................................................................................................................... 7 2. DEFINITIONS .......................................................................................................................................... 7 3. HAZARDS IDENTIFICATION AND EVALUATION ................................................................................... 10 4. ESTABLISHING ROLES AND RESPONSIBILITIES .................................................................................... 14 5. CHOOSING AND USING A TECHNIQUE FROM THIS GUIDE ................................................................. 17 6. CHANGE CONTROL .............................................................................................................................. 19 7. ASSESSING -

Mansfield, NG18 2AD to the Editor: Dear Sir, VERTIGO in DIVERS Thank You for Asking for My Comments on Noel Roydhouse's Letter Which I Have Read with Interest
Br J Sports Med: first published as 10.1136/bjsm.17.3.210 on 1 September 1983. Downloaded from 210 CORRESPONDENCE 14 Woodhouse Road, Mansfield, NG18 2AD To the Editor: Dear Sir, VERTIGO IN DIVERS Thank you for asking for my comments on Noel Roydhouse's letter which I have read with interest. He is technically correct in stating that vertigo is not inevitable when the tympanic membrane ruptures. Vertigo is not dependent on the size of perforation that is sustained, but is dependent on the rate of ingress of cold water into the tympanic cavity. The caloric effect produced by rapid ingress of water is entirely dependent on the temperature difference between the water that has entered the tympanic cavity and body temperature. Once the water temperature reaches approximate body temperature then the caloric effect ceases as does the vertigo. As ENT surgeons we use this caloric phenomenon for testing labyrinthine function (vestibular function); and under test conditions we use water at 300C and 440C, in ears with intact tympanic membranes, in order to induce a vertigo. If an article were to be directed at "diving doctors" I think that it would be fair comment for it to be stated that a vertigo sustained on descent should be assumed to be due to a tympanic membrane rupture with rapid ingress of water, until proven otherwise, by inspection of the ear; if the tympanic membrane is found to be intact, then a diagnosis of perilymph fistula must be made, which will only be proved or disproved by performing an exploratory tympanotomy. -

Review of Diver Noise Exposure
doi:10.3723/ut.29.021 International Journal of the Society for Underwater Technology, Vol 29, No 1, pp 21–39, 2010 Review of diver noise exposure TG Anthony, NA Wright and MA Evans QinetiQ Ltd, Hampshire, UK Technical Paper Abstract • Assess the risk to all employees, including divers, Divers are exposed to high noise levels from a variety from noise at work of sources both above and below water. The noise • Take action to reduce the noise exposure that exposure should comply with `The Control of Noise produces these risks at Work Regulations 2005' (CoNaWR05, 2005). A • Provide hearing protection if the noise risk detailed review of diver noise exposure is presented, cannot be reduced sufficiently by other methods encompassing diver hearing, noise sources, exposure • Ensure legal limits on noise exposure are not levels and control measures. Divers are routinely exceeded exposed to a range of noise sources of sufficiently high • Provide employees with information, instruction intensity to cause auditory damage, and audiometric and training studies indicate that diver hearing is impaired by • Conduct health surveillance where there is a risk exposure to factors associated with diving. Human to health. hearing under water, in cases where the diver's ear is The CoNaWR05 requires employers to take wet, is less sensitive than in air and should be assessed specific action at certain noise action values. These using an underwater weighting scale. Manufacturers of relate to the levels of exposure to noise of divers diving equipment and employers of divers have a joint averaged over a working day or week and the responsibility to ensure compliance with the exposure maximum noise (peak sound pressure) to which values in the CoNaWR05, although noise is only one they may be exposed. -

Hyperbaric Physiology the Rouse Story Arrival at Recompression
Hyperbaric Physiology The Rouse Story • Oct 12, 1992, off the New Jersey coast • father/son team of experienced divers • explore submarine wreck in 230 ft (70 m) • breathing compressed air • trapped in wreck & escaped with no time for decompression Chris and Chrissy Rouse Arrival at recompression Recompression efforts facility • Both divers directly ascend to dive boat • Recompression starts about 3 hrs after • Helicopter arrives at boat in 1 hr 27 min ascent • Bronx Municipal Hospital recompression facility – put on pure O2 and compressed to 60 ft – Chris (39 yrs) pronounced dead • extreme pain as circulation returned – compressed to 165 ft, then over 5.5 hrs – Chrissy (22 yrs) gradually ascended back to 30 ft., lost • coherent and talking consciousness • paralysis from chest down • no pain – back to 60 ft. Heart failure and death • blood sample contained foam • autopsy revealed that the heart contained only foam Medical Debriefing Gas Laws • Boyle’s Law • Doctors conclusions regarding their – P1V1 = P2V2 treatment • Dalton’s Law – nothing short of recompression to extreme – total pressure is the sum of the partial pressures depths - 300 to 400 ft • Henry’s Law – saturation treatment lasting several days – the amt of gas dissolved in liquid at any temp is – complete blood transfusion proportional to it’s partial pressure and solubility – deep helium recompression 1 Scuba tank ~ 64 cf of air Gas problems during diving Henry, 1 ATM=33 ft gas (10 m) dissovled = gas Pp & tissue • Rapture of the deep (Nitrogen narcosis) solubility • Oxygen -

History of Scuba Diving About 500 BC: (Informa on Originally From
History of Scuba Diving nature", that would have taken advantage of this technique to sink ships and even commit murders. Some drawings, however, showed different kinds of snorkels and an air tank (to be carried on the breast) that presumably should have no external connecons. Other drawings showed a complete immersion kit, with a plunger suit which included a sort of About 500 BC: (Informaon originally from mask with a box for air. The project was so Herodotus): During a naval campaign the detailed that it included a urine collector, too. Greek Scyllis was taken aboard ship as prisoner by the Persian King Xerxes I. When Scyllis learned that Xerxes was to aack a Greek flolla, he seized a knife and jumped overboard. The Persians could not find him in the water and presumed he had drowned. Scyllis surfaced at night and made his way among all the ships in Xerxes's fleet, cung each ship loose from its moorings; he used a hollow reed as snorkel to remain unobserved. Then he swam nine miles (15 kilometers) to rejoin the Greeks off Cape Artemisium. 15th century: Leonardo da Vinci made the first known menon of air tanks in Italy: he 1772: Sieur Freminet tried to build a scuba wrote in his Atlanc Codex (Biblioteca device out of a barrel, but died from lack of Ambrosiana, Milan) that systems were used oxygen aer 20 minutes, as he merely at that me to arficially breathe under recycled the exhaled air untreated. water, but he did not explain them in detail due to what he described as "bad human 1776: David Brushnell invented the Turtle, first submarine to aack another ship. -

No Limits Freediving
1 No Limits Freediving "The challenges to the respiratory function of the breath-hold diver' are formidable. One has to marvel at the ability of the human body to cope with stresses that far exceed what normal terrestrial life requires." Claes Lundgren, Director, Center for Research and Education in Special Environments A woman in a deeply relaxed state floats in the water next to a diving buoy. She is clad in a figure-hugging wetsuit, a dive computer strapped to her right wrist, and another to her calf. She wears strange form-hugging silicone goggles that distort her eyes, giving her a strange bug-eyed appearance. A couple of meters away, five support divers tread water near a diving platform, watching her perform an elaborate breathing ritual while she hangs onto a metal tube fitted with two crossbars. A few meters below the buoy, we see that the metal tube is in fact a weighted sled attached to a cable descending into the dark-blue water. Her eyes are still closed as she begins performing a series of final inhalations, breathing faster and faster. Photographers on the media boats snap pictures as she performs her final few deep and long hyperventilations, eliminating carbon dioxide from her body. Then, a thumbs-up to her surface crew, a pinch of the nose clip, one final lungful of air, and the woman closes her eyes, wraps her knees around the bottom bar of the sled, releases a brake device, and disappears gracefully beneath the waves. The harsh sounds of the wind and waves suddenly cease and are replaced by the effervescent bubbling of air being released from the regulators of scuba-divers. -

Heat Stroke Heat Exhaustion
Environmental Injuries Co lin G. Ka ide, MD , FACEP, FAAEM, UHM Associate Professor of Emergency Medicine Board-Certified Specialist in Hyperbaric Medicine Specialist in Wound Care The Ohio State University Wexner Medical Center The Most Dangerous Drug Combination… Accidental Testosterone Hypothermia and Alcohol! The most likely victims… Photo: Ralf Roletschek 1 Definition of Blizzard Hypothermia of Subnormal T° when the body is unable to generate sufficient heat to sustain normal functions Core Temperature < 95°F 1979 (35°C) Most Important Temperatures Thermoregulation 95°F (35° C) Hyper/Goofy The body uses a Poikilothermic shell to maintain a Homeothermic core 90°F (32°C) Shivering Stops Maintains core T° w/in 1.8°F(1°C) 80°F (26. 5°C) Vfib, Coma Hypothalamus Skin 65°F (18°C) Asystole Constant T° 96.896.8-- 100.4° F 2 Thermoregulation The 2 most important factors Only 3 Causes! Shivering (10x increase) Decreased Heat Production Initiated by low skin temperature Increased Heat Loss Warming the skin can abolish Impaired Thermoregulation shivering! Peripheral vasoconstriction Sequesters heat Predisposing Predisposing Factors Factors Decreased Production Increased Loss –Endocrine problems Radiation Evaporation • Thyroid Conduction* • Adrenal Axis Convection** –Malnutrition *Depends on conducting material **Depends on wind velocity –Neuromuscular disease 3 Predisposing Systemic Responses CNS Factors T°< 90°F (34°C) Impaired Regulation Hyperactivity, excitability, recklessness CNS injury T°< 80°F (27°C) Hypothalamic injuries Loss of voluntary -

Miller Manual
MILLER DIVING EQUIPMENT INC. Miller 400 Diving Helmet Maintenance Manual © Miller Diving All Rights Reserved Document # 030715001 1 MILLER 400 DIVING HELMET OPERATIONS AND MAINTENANCE MANUAL Part # 100-900 TABLE OF CONTENTS WARRANTY ............................................................................................................................... 3 DEFINITIONS OF SIGNAL WORDS ........................................................................................ 4 IMPORTANT SAFETY INFORMATION .................................................................................. 5 SECTION 1: GENERAL INFORMATION 1-A INTRODUCTION ............................................................................................. 7 1-B GENERAL DESCRIPTION OF MILLER 400 ................................................ 7 SECTION 2: OPERATING INSTRUCTIONS AND PROCEDURES 2-A PRE-DIVE PROCEDURE .................................................................................8 2-B DRESSING INTO THE MILLER HELMET ....................................................8 2-C OPERATING INSTRUCTIONS .......................................................................9 2-D EMERGENCY PROCEDURES ........................................................................9 2-E RECOMMENDED MATERIALS FOR MAINTENANCE .............................10 SECTION 3: DESCRIPTIONS, MAINTENANCE AND REPLACEMENT 3-A HELMET SHELL ..............................................................................................12 3-B FACE PLATE AND FACE RING .....................................................................12 -

Ari D'agostino, Csilla
BIOGRAPHICAL SKETCH NAME Address: University of South Florida, 4202 E. Fowler Ave, PCD 3127, Tampa, FL, 33620 Csilla Ari D`Agostino, Ph.D. Phone: +1(813) 2409925 Email: [email protected], [email protected] INSTITUTION AND LOCATION DEGREE Completion Date FIELD OF STUDY (if applicable) MM/YYYY Szent Istvan University, HU M.S. 1997-2002 Zoology Semmelweis University, HU Ph.D. 2002-2008 Neurosciences University of South Florida, Postdoctoral scholar 06/2010-09/2012 Molecular Medicine Tampa, FL Molecular Pharmacology and University of South Florida, Postdoctoral scholar 09/2012-09/2013 Physiology Tampa, FL University of South Florida, Research Associate Molecular Pharmacology and 09/2013- 12/2016 Tampa, FL Physiology University of South Florida, Research Assistant 3/2017-1/2020 Psychology Tampa, FL Professor A. Personal Statement I have a broad background in comparative neuroanatomy, molecular biology, microscopy, physiology, with numerous peer reviewed publications- mostly as first author-, a book and a book chapter, 7 provisional patents, as well as many national and international conference presentations. I completed my PhD in 2008 on the cerebralization, astroglial architecture and blood-brain barrier composition of cartilaginous fishes using immunohistochemical markers on 12 shark and ray species. After completing my PhD I moved to the United States of America and on June 1st, 2010 I joined Dr. Huntington Potter`s laboratory at the Byrd Alzheimer`s Institute. My project focused on studying the mechanism of neurotransmitter and neurotrophin receptor mislocalization in Alzheimer`s disease and my work involved cell cultures, immunocytochemistry, flow cytometry, spectrophotometry, Atomic Force Microscopy (AFM), fluorescence and confocal microscopy, RT-PCR and recombinant DNA techniques. -

Dry Suit Diving Provides the Diver with a Layer of Air Around the Body
Dry suits come into play when preventing convection is no longer adequate in delaying the loss of body heat. A dry suit Dry Suit Diving provides the diver with a layer of air around the body. Air is a better thermal insulator than water. A diver will still get cold, but the additional delay in losing body heat will make it possibleto enjoya diveinthecoldest environments. The layer of air is an advantage for thermal insulation. The air in the suit also offers options for positioning in the water that would be difficult with a wetsuit. Unfortunately the added advantage is a trade-off with inconveniences. Diving in adrysuit is not without challenges. An additional airspace (next to lungs and BCD) makes buoyancy control more difficult. Dry suits require special maintenance. Dry suits also alter requirements for other equipment items and in most cases come with a need for additional weight. Dry suit training is needed in order to cope with the additional challenges. Dry suit training will also provide valuable information for selecting your own drysuit. Divers lose their body heat via direct contact with the colder water. The body heat is lost via conduction. Conduction means that the warmer substance (the skin) has direct contact with the colder substance (water). An unprotected swimmer loses body heat up to 25 times faster in water than in air. Convection refers to the fact that warmed-up water is lighter than colder water. The warmer water moves up and is replaced by colder water. Your body therefore is repeatedly heating up cold water.