Money and Morals
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
GERON CORPORATION (Exact Name of Registrant As Specified in Its Charter)
UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, D.C. 20549 FORM 10-K (Mark One) ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the Fiscal Year Ended December 31, 2019 or TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the transition period from to . Commission File Number: 0-20859 GERON CORPORATION (Exact name of registrant as specified in its charter) Delaware 75-2287752 (State or other jurisdiction of (I.R.S. Employer incorporation or organization) Identification No.) 149 Commonwealth Drive, Suite 2070, Menlo Park, CA 94025 (Address of principal executive offices) (Zip Code) Registrant’s telephone number, including area code: (650) 473-7700 Securities registered pursuant to Section 12(b) of the Act: Title of each class: Trading symbol(s): Name of each exchange on which registered: Common Stock, $0.001 par value GERN The Nasdaq Stock Market LLC Securities registered pursuant to Section 12(g) of the Act: None Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes No Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes No Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. -

Lengthened Telomeres Restore Immune System to a Younger State
Dear friend, you are presumably here to find out more information on TA-65 telomeres and telomerase. This page contains just a small amount of what I have written about the topics but, many times the questions I get are the same. Here you will find the answers to many of the more frequently asked questions that I could not cover on the TA-65 page. Please note: I kept many of them in “post format” as they were originally published on the internet. Lengthened telomeres restore immune system to a younger state New study is the first ever Peer-Reviewed Report of a Telomerase Activator taken by live humans. New York, NY (September 8, 2010) — A pioneering study published in the Rejuvenation Research Journal today shows that TA-65, a natural Telomerase Activator made and marketed by Telomerase Activation Sciences, Inc. (“T.A. Sciences”), reduces the percentage of short telomeres in immune cells and restores and remodels the aging human immune system to be more like that of a younger individual. The year-long study of the first 100 clients of T.A. Sciences found that TA-65, a nutritional supplement marketed only through specialized doctors, had been successful in lengthening shortened telomeres. Telomeres are sequences of DNA, located at the ends of all chromosomes, which serve as cellular clocks of aging. Every time a cell divides, telomeres shorten until they become critically short, and the cell either stops functioning properly or dies. By activating a gene that is normally turned off, TA-65 has been shown to activate the enzyme telomerase. -
![Michael D. West (1953- ) [1]](https://docslib.b-cdn.net/cover/2064/michael-d-west-1953-1-472064.webp)
Michael D. West (1953- ) [1]
Published on The Embryo Project Encyclopedia (https://embryo.asu.edu) Michael D. West (1953- ) [1] By: Jiang, Lijing Keywords: Biography [2] Stem cells [3] Regeneration [4] Michael D. West is a biomedical entrepreneur and investigator whose aim has been to extend human longevity with biomedical interventions. His focus has ranged from the development of telomerase-based therapeutics to the application of human embryonic stem cells [5] in regenerative medicine [6]. Throughout his eventful career, West has pursued novel and sometimes provocative ideas in a fervent, self-publicizing manner. As of 2009, West advocated using human somatic cell nuclear transfer [7] techniques to derive human embryonic stem cells [5] for therapeutic practice. Through his testimonies before the US Senate, articles, and even controversies generated by his own research and claims, West has played an important role in shaping the public debate over human cloning [8] and embryonic stem cell research [9]. Born in Niles, Michigan, on 28 April 1953, West grew up in a wealthy family that ran a profitable automotive leasing business. West’s scientific predilection was discovered and cultivated early in his childhood, when he could enjoy a laboratory-like set-up in a storage area above the family’s garage. After entering Niles Senior High School, West became interested in a broad range of philosophical questions such as the meaning of life. These interests led him into an amateur but persistent study of philosophy, theology, mythology, and folklore for about ten years, during which he also managed to teach himself Greek and Hebrew. The intellectual development of West, although initiated somewhat precociously, took a most circuitous path. -

Geron Initiates Randomized Phase 2 Clinical Trial of Imetelstat in Breast Cancer
Geron Initiates Randomized Phase 2 Clinical Trial of Imetelstat in Breast Cancer December 2, 2010 10:52 AM ET Telomerase Inhibitor in Combination with Chemotherapy Targets Cancer Stem Cells MENLO PARK, Calif., December 2, 2010 - Geron Corporation (Nasdaq: GERN) today announced enrollment of the first patient in a randomized Phase 2 clinical trial of its telomerase inhibitor drug, imetelstat (GRN163L), in combination with paclitaxel (with or without bevacizumab) in patients with locally recurrent or metastatic breast cancer. "We are pleased to initiate our second randomized Phase 2 clinical trial of imetelstat," said Stephen M. Kelsey, M.D., Geron's executive vice president and chief medical officer, oncology. "We are applying what we learned in our Phase 1 program and leveraging our preclinical data that showed imetelstat's activity against cancer stem cells from a broad range of tumor types, including breast cancer." "We look forward to assessing imetelstat in this Phase 2 clinical trial in breast cancer," said Kathy D. Miller, M.D., Associate Professor and Sheila D. Ward Scholar at the Indiana University Melvin and Bren Simon Cancer Center and lead investigator of the trial. "The Phase 1 trial of imetelstat combined with paclitaxel and bevacizumab in locally recurrent or metastatic breast cancer showed an encouraging preliminary response rate, particularly in context of the reduced doses of chemotherapy that were administered during treatment cycles." Phase 2 Trial Design The clinical trial is an open label, multi-center, randomized Phase 2 study of the efficacy and safety of treatment with imetelstat plus paclitaxel (with or without bevacizumab) versus paclitaxel (with or without bevacizumab) for patients with locally recurrent or metastatic breast cancer (MBC) who have not received chemotherapy or have received one non-taxane based chemotherapy for MBC. -

Michael West CV
MICHAEL DAVID WEST, B.S., M.S., Ph.D. CURRICULUM VITAE November, 2016 Summary: Dr. West is Co-Chief Executive Officer of BioTime, Inc. (NYSE MKT: BTX). BioTime and its subsidiaries are focused on developing an array of research and therapeutic products using pluripotent stem cell technology. He received his Ph.D. from Baylor College of Medicine in 1989 concentrating on the biology of cellular aging. He has focused his academic and business career on the application of developmental biology to the age-related degenerative disease. He was the founder and first CEO of Geron Corporation of Menlo Park, California (Nasdaq: GERN) and from 1992 to 1998 he was a Director, and Vice President, where he initiated and managed programs in telomerase diagnostics, oligonucleotide-based telomerase inhibition as anti-tumor therapy, and the cloning and use of telomerase in telomerase-mediated therapy wherein telomerase is utilized to immortalize human cells. From 1995 to 1998 he organized and managed the research collaboration between Geron and its academic collaborators James Thomson and John Gearhart that led to the first isolation of human embryonic stem and human embryonic germ cells. In 2013 he led BioTime’s efforts to acquire Geron’s stem cell assets now residing in the BioTime subsidiary Asterias Biotherapeutics (NYSE MKT: AST). From 1998 to 2007 he held positions as CEO, President, and Chief Scientific Officer at Advanced Cell Technology, Inc., which was acquired by Astellas Pharma, Inc., where he managed programs in nuclear transfer, retinal differentiation, and PureStemTM, a technology for the multiplex derivation and characterization of diverse clonal human embryonic progenitor cell lines. -

Geron Corporation
GERON CORPORATION FORM 10-K (Annual Report) Filed 2/27/2004 For Period Ending 12/31/2003 Address 230 CONSTITUTION DRIVE MENLO PARK, California 94025 Telephone 650-473-7700 CIK 0000886744 Industry Biotechnology & Drugs Sector Healthcare Fiscal Year 12/31 UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, D.C. 20549 FORM 10-K [X] ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the Fiscal Year Ended December 31, 2003 or [ ] TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the Transition Period From to ____________ to __________. Commission File Number: 0-20859 GERON CORPORATION (Exact name of registrant as specified in its charter) Delaware 75 -2287752 (State or other jurisdiction of (I.R.S. Employer incorporation or organization) Identification No.) 230 Constitution Drive, Menlo Park, CA 94025 (Address, including zip code, of principal executive offices) Registrant’s telephone number, including area code: (650) 473-7700 Securities registered pursuant to Section 12(b) of the Act: None Securities registered pursuant to Section 12(g) of the Act: Common Stock $0.001 par value Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes [X] No [ ] Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. -
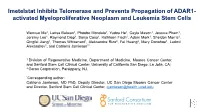
Activated Myeloproliferative Neoplasm and Leukemia Stem Cells
Imetelstat Inhibits Telomerase and Prevents Propagation of ADAR1- activated Myeloproliferative Neoplasm and Leukemia Stem Cells Wenxue Ma1, Larisa Balaian1, Phoebe Mondala1, Yudou He1, Cayla Mason1, Jessica Pham1, Jeremy Lee1, Raymond Diep1, Sanja Coso1, Kathleen Fisch1, Adam Mark1, Sheldon Morris1, Qingfei Jiang1, Thomas Whisenant1, Aleksandra Rizo2, Fei Huang2, Mary Donohoe1, Ludmil Alexandrov1, and Catriona Jamieson1* 1 Division of Regenerative Medicine, Department of Medicine, Moores Cancer Center, and Sanford Stem Cell Clinical Center, University of California San Diego, La Jolla, CA; 2 Geron Corporation, Parsippany, NJ. *Corresponding author: Catriona Jamieson, MD PhD, Deputy Director, UC San Diego Moores Cancer Center and Director, Sanford Stem Cell Clinical Center, [email protected] Fig. 1 Telomere Shortening Characterizes Pre-LSC and LSC A B ●● ●● 100 R = - 0.46 , p = 0.003 100 R = - 0.47 , p = 0.0023 Wilcoxon, p = 0.041 Wilcoxon, p = 0.14 y = 97 - 0.092 x y = 98 - 0.11 x n n i i ● ● t t n n ● e e t ● ● t 15 n ● ● ● ● ● n s o ● ● o 80 ● ● 80 ● ● l l c c 10 ● ● ● e e e ● c s r ● ● ● ● r l ● ● l ● ● ● ● e ● ● e Sex ● Sex e ● ● ● ● m c m m ● ● e ● ● ● ● t o ● ● ●● o ● ● ● ● a l l ● ● ● s ● ● Female Female e e v e e g g i ● t t l ● ● + 10 A A ● ● ● ● ● ● a 4 Male Male d 60 60 d ● ● ● s 3 ● e e ● t ● ● t ● ● ● ● D ● c ● ● ● ● c ● ● C e e ● ● ● ● ● r r ● ● ● ● ● r ● ● r ● ● ● ● o ● ● o ● 5 ● ● c ● ● ● ● c ● ●● ● e ● ● e ● ● ● ● g g ● ● 40 40 ● ● ● ● 5 ● ● ● ●● ● ● ● A ● ● A ● ● ● ●● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● Female -

Geron Corporation 2000 Annual Report
ANNUAL REPORT 2000 Sometimes the body heals itself. Sometimes it does not. UNLIKE BONE, NEURONS DO NOT REGENERATE AFTER INJURY. IF A NERVE CELL IS DAMAGED DUE TO DISEASE OR INJURY, THERE IS NO TREATMENT AT PRESENT TO RESTORE LOST FUNCTION. GERON / 2000 Sometimes our cells fight disease. GERON / 2000 . Sometimes our cells are the disease. CANCER OCCURS WHEN CELLS BEGIN TO MULTIPLY EXCESSIVELY AS THE RESULT OF GENETIC MUTATIONS, CAUSING A TUMOR TO GROW UNCONTROLLABLY. TUMORS TURN ESPECIALLY DEADLY WHEN CANCER CELLS SPREAD THROUGHOUT THE BODY. GERON / 2000 How When Why Where Oncology FINDING AND FIGHTING CANCER Geron is leveraging the power of telomerase to develop novel ways of diagnosing and treating a broad range of cancers. An enzyme that confers replicative immortality to cells, telomerase is present in all cancer types studied to date, making it a universal and specific target for the development of a new class of cancer diagnostics and therapeutics. Regenerative Medicine REPAIRING DAMAGE, RESTORING FUNCTION Through the integration of its powerful and proprietary technology platforms, Geron intends to become the leader in the emerging field of regenerative medicine. The company’s goal is to produce tissue-matched, healthy and youthful replacement cells to restore organ function lost to disease. In this way, Geron expects to establish living cells as tomorrow’s pharmaceuticals. GERON / 2000 . GERON’S THREE TECHNOLOGY PLATFORMS SUPPORT MULTIPLE PRODUCT OPPORTUNITIES THAT ARE GROUPED BY TARGET MARKET INTO FOUR BUSINESS UNITS TO ACCELERATE PRODUCT DEVELOPMENT, PARTNERING AND COMMERCIALIZATION. Oncology Regenerative Medicine • Telomerase • Human Embryonic Stem Cells • Nuclear Transfer Predictive Nuclear Transfer: Toxicology and Screening Ag / Xeno / Biologics . -

Geron Annual Report 2008
GERON ANNUAL REPORT 2008 Dear Stockholders, The two principal goals for Geron Corporation in 2008 were to initiate the world’s first clinical trial of a human embryonic stem cell (hESC)-based therapy and to demonstrate utility of GRN163L, our telomerase inhibitor drug, in cancer patients. In last year’s annual report, we stated that accomplishing these two goals would complete our transition into a fully integrated clinical development company. I am pleased to report success on both fronts as detailed in the enclosed letters. Each product in clinical development is a proprietary, first-in-class therapy with substantial economic potential. We expect a very exciting 2009 as we advance our programs toward the demonstration of safety and clinical utility in patients. As always, we are grateful for your support. REGENERATIVE MEDICINE “ FDA clearance of our GRNOPC1 Investigational New Drug (IND) application is one of Geron’s most significant accomplishments to date. This marks the beginning of what is potentially a new chapter in medical therapeutics — one that reaches beyond pills to a new level of healing: the restoration of organ and tissue function achieved by the injection of healthy replacement cells.” REGENERATIVE MEDICINE GRNOPC1 – Glial Cells fOR SPINAL CORD INJURY Geron Receives FDA Clearance to Begin World’s First Human Clinical Trial of Embryonic Stem Cell-Based Therapy In January of 2009, we received clearance from the U.S. Food and Drug Administration (FDA) to begin a clinical trial of GRNOCP1, our hESC-derived cell therapy for acute spinal cord injury. GRNOPC1 contains hESC-derived oligodendrocyte progenitor cells that have demonstrated remyelinating and nerve growth stimulating properties leading to restoration of function in animal models of acute spinal cord injury (Journal of Neuroscience, Vol. -

US Treats First Patient with Human Embryonic Stem Cells (Update 2) 11 October 2010, by Karin Zeitvogel
US treats first patient with human embryonic stem cells (Update 2) 11 October 2010, by Karin Zeitvogel US doctors have begun the first tests of human Geron began working with human embryonic stem embryonic stem cells in patients, treating a man cells in 1999. with spinal cord injuries in a landmark trial of the controversial process, the Geron Corporation said Back then, "many predicted that it would be a Monday. number of decades before a cell therapy would be approved for human clinical trials," Geron's The patient began the pioneering treatment Friday president and chief executive Thomas Okarma said with an injection of the biotech company's human in a statement. embryonic stem cells, as part of a clinical trial that aims to test safety and efficacy toward regaining Okarma described Monday's start of the clinical trial sensation and movement. as "a milestone for the field of human embryonic stem cell-based therapies." The treatment took place at the Shepherd Center in Atlanta, Georgia, a spokeswoman for the GRNOPC1 is made up of cells containing hospital told AFP, declining to give further details precursors to oligodendrocytes -- multi-tasking cells due to patient privacy concerns. that occur in the nervous system. The Phase I trial is expected to involve around 10 Oligodendrocytes are lost in spinal cord injury, patients. Participants in the human trials must be resulting in myelin and neuronal loss which cause severely injured and start treatment with Geron's paralysis in many patients. product, GRNOPC1, seven to 14 days after sustaining their injury. Preclinical studies of GRNOPC1 found that when it was injected into the injury site of animals with Patients will be given a single injection of two spinal cord injuries, it migrated throughout the million of Geron's GRNOPC1 cells in the trial. -

Geron Corporation 919 E
GERON CORPORATION 919 E. Hillsdale Blvd., Suite 250 Foster City, CA 94404 April 14, 2020 Dear Fellow Geron Stockholder: You are cordially invited to attend the 2020 Annual Meeting of Stockholders (the “Annual Meeting”) of Geron Corporation to be held on Friday, June 5, 2020, at 8:00 a.m., Pacific Daylight Time. In light of the COVID-19 pandemic, for the safety of all our stockholders and personnel, and taking into account recent federal, state and local guidance that has been issued, we have determined that the Annual Meeting will be held in a virtual meeting format only, via the Internet, with no physical in-person meeting. You will be able to attend and participate in the virtual Annual Meeting online by visiting www.virtualshareholdermeeting.com/GERN2020, where you will be able to listen to the meeting live, submit questions, and vote. Instructions on how to participate in the virtual Annual Meeting and demonstrate proof of stock ownership are posted at www.virtualshareholdermeeting.com/GERN2020. The webcast of the virtual Annual Meeting will be archived for one year after the date of the virtual Annual Meeting at www.virtualshareholdermeeting.com/GERN2020. As permitted by the rules of the Securities and Exchange Commission, we are pleased to furnish our proxy materials to stockholders primarily over the Internet. Consequently, most stockholders will receive a notice with instructions for accessing proxy materials and voting via the Internet, instead of paper copies of proxy materials. However, this notice will provide information on how stockholders may obtain paper copies of proxy materials if they choose. -

Geron Announces Presentation at ECTRIMS/ACTRIMS October 25, 2011 3:38 PM ET Non-Clinical Data Supports Use of GRNOPC1 in Multipl
Geron Announces Presentation at ECTRIMS/ACTRIMS October 25, 2011 3:38 PM ET Non-Clinical Data Supports Use of GRNOPC1 in Multiple Sclerosis MENLO PARK, Calif., October 25, 2011 - Geron Corporation (Nasdaq: GERN) today announced data on the use of GRNOPC1, oligodendrocyte progenitors derived from human embryonic stem cells, for myelin repair in a non-human primate model. The data supports further investigation of the potential therapeutic use of GRNOPC1 in central nervous system (CNS) disorders where the central or contributing pathology is destructive removal of myelin from nerve axons, such as observed in multiple sclerosis (MS), myelitis and spinal cord injury. GRNOPC1 is currently in a Phase 1 clinical trial in patients with spinal cord injury. The new data were presented at the 5th Joint Triennial Congress of the European and Americas Committees for Treatment and Research in Multiple Sclerosis, in Amsterdam, by Prof. Jeffery D. Kocsis, Ph.D., from Yale University School of Medicine. The work was performed in collaboration with scientists at Geron. The studies utilized a non-human primate model where demyelinated lesions, such as seen in multiple sclerosis, were induced chemically in the spinal cord. GRNOPC1 was injected into the demyelinated spinal cord lesions one week after chemical induction. The lesion sites from six monkeys were analyzed using light and electron microscopy at various timepoints up to one year after injection of GRNOPC1 to look for evidence of cell survival and remyelination of nerve axons. In the first few weeks after implantation, the injection sites contained maturing transplanted cells indicative of a premyelinating phenotype with evidence of variable numbers and degrees of remyelinated axons.