The Effects of Surfactants on the Solubility and Dissolution Profiles of a Poorly Water-Soluble Basic Drug, Carvedilol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
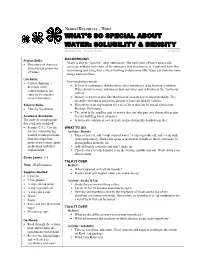
Effects of Surfactants on the Toxicitiy of Glyphosate, with Specific Reference to RODEO
SERA TR 97-206-1b Effects of Surfactants on the Toxicitiy of Glyphosate, with Specific Reference to RODEO Submitted to: Leslie Rubin, COTR Animal and Plant Health Inspection Service (APHIS) Biotechnology, Biologics and Environmental Protection Environmental Analysis and Documentation United States Department of Agriculture Suite 5A44, Unit 149 4700 River Road Riverdale, MD 20737 Task No. 5 USDA Contract No. 53-3187-5-12 USDA Order No. 43-3187-7-0028 Prepared by: Gary L. Diamond Syracuse Research Corporation Merrill Lane Syracuse, NY 13210 and Patrick R. Durkin Syracuse Environmental Research Associates, Inc. 5100 Highbridge St., 42C Fayetteville, New York 13066-0950 Telephone: (315) 637-9560 Fax: (315) 637-0445 CompuServe: 71151,64 Internet: [email protected] February 6, 1997 TABLE OF CONTENTS EXECUTIVE SUMMARY ......................................... iii 1. INTRODUCTION .............................................1 2. CONSTITUENTS OF SURFACTANT FORMULATIONS USED WITH RODE0 ....4 2.1. AGRI-DEX ..........................................4 2.2. LI-700 .............................................4 2.3. R-11 ...............................................6 2.4. LATRON AG-98 ......................................6 2.5. LATRON AG-98 AG ....................................7 3. INFORMATION ON EFFECTS OF SURFACTANT FORMULATIONS ON THE TOXICITY OF RODEO ................................8 3.1. HUMAN HEALTH ......................................8 3.1.1. LI 700 ........................................8 3.1.2. Phosphatidylcholine ................................8 -

Pulmonary Surfactant: the Key to the Evolution of Air Breathing Christopher B
Pulmonary Surfactant: The Key to the Evolution of Air Breathing Christopher B. Daniels and Sandra Orgeig Department of Environmental Biology, University of Adelaide, Adelaide, South Australia 5005, Australia Pulmonary surfactant controls the surface tension at the air-liquid interface within the lung. This sys- tem had a single evolutionary origin that predates the evolution of the vertebrates and lungs. The lipid composition of surfactant has been subjected to evolutionary selection pressures, partic- ularly temperature, throughout the evolution of the vertebrates. ungs have evolved independently on several occasions pendent units, do not necessarily stretch upon inflation but Lover the past 300 million years in association with the radi- unpleat or unfold in a complex manner. Moreover, the many ation and diversification of the vertebrates, such that all major fluid-filled corners and crevices in the alveoli open and close vertebrate groups have members with lungs. However, lungs as the lung inflates and deflates. differ considerably in structure, embryological origin, and Surfactant in nonmammals exhibits an antiadhesive func- function between vertebrate groups. The bronchoalveolar lung tion, lining the interface between apposed epithelial surfaces of mammals is a branching “tree” of tubes leading to millions within regions of a collapsed lung. As the two apposing sur- of tiny respiratory exchange units, termed alveoli. In humans faces peel apart, the lipids rise to the surface of the hypophase there are ~25 branches and 300 million alveoli. This structure fluid at the expanding gas-liquid interface and lower the sur- allows for the generation of an enormous respiratory surface face tension of this fluid, thereby decreasing the work required area (up to 70 m2 in adult humans). -

Solubility and Aggregation of Selected Proteins Interpreted on the Basis of Hydrophobicity Distribution
International Journal of Molecular Sciences Article Solubility and Aggregation of Selected Proteins Interpreted on the Basis of Hydrophobicity Distribution Magdalena Ptak-Kaczor 1,2, Mateusz Banach 1 , Katarzyna Stapor 3 , Piotr Fabian 3 , Leszek Konieczny 4 and Irena Roterman 1,2,* 1 Department of Bioinformatics and Telemedicine, Jagiellonian University—Medical College, Medyczna 7, 30-688 Kraków, Poland; [email protected] (M.P.-K.); [email protected] (M.B.) 2 Faculty of Physics, Astronomy and Applied Computer Science, Jagiellonian University, Łojasiewicza 11, 30-348 Kraków, Poland 3 Institute of Computer Science, Silesian University of Technology, Akademicka 16, 44-100 Gliwice, Poland; [email protected] (K.S.); [email protected] (P.F.) 4 Chair of Medical Biochemistry—Jagiellonian University—Medical College, Kopernika 7, 31-034 Kraków, Poland; [email protected] * Correspondence: [email protected] Abstract: Protein solubility is based on the compatibility of the specific protein surface with the polar aquatic environment. The exposure of polar residues to the protein surface promotes the protein’s solubility in the polar environment. The aquatic environment also influences the folding process by favoring the centralization of hydrophobic residues with the simultaneous exposure to polar residues. The degree of compatibility of the residue distribution, with the model of the concentration of hydrophobic residues in the center of the molecule, with the simultaneous exposure of polar residues is determined by the sequence of amino acids in the chain. The fuzzy oil drop model enables the quantification of the degree of compatibility of the hydrophobicity distribution Citation: Ptak-Kaczor, M.; Banach, M.; Stapor, K.; Fabian, P.; Konieczny, observed in the protein to a form fully consistent with the Gaussian 3D function, which expresses L.; Roterman, I. -
Solubility & Density
Natural Resources - Water WHAT’S SO SPECIAL ABOUT WATER: SOLUBILITY & DENSITY Activity Plan – Science Series ACTpa025 BACKGROUND Project Skills: Water is able to “dissolve” other substances. The molecules of water attract and • Discovery of chemical associate with the molecules of the substance that dissolves in it. Youth will have fun and physical properties discovering and using their critical thinking to determine why water can dissolve some of water. things and not others. Life Skills: • Critical thinking – Key vocabulary words: develops wider • Solvent is a substance that dissolves other substances, thus forming a solution. comprehension, has Water dissolves more substances than any other and is known as the “universal capacity to consider solvent.” more information • Density is a term to describe thickness of consistency or impenetrability. The scientific formula to determine density is mass divided by volume. Science Skills: • Hypothesis is an explanation for a set of facts that can be tested. (American • Making hypotheses Heritage Dictionary) • The atom is the smallest unit of matter that can take part in a chemical reaction. Academic Standards: It is the building block of matter. The activity complements • A molecule consists of two or more atoms chemically bonded together. this academic standard: • Science C.4.2. Use the WHAT TO DO science content being Activity: Density learned to ask questions, 1. Take a clear jar, add ¼ cup colored water, ¼ cup vegetable oil, and ¼ cup dark plan investigations, corn syrup slowly. Dark corn syrup is preferable to light so that it can easily be make observations, make distinguished from the oil. predictions and offer 2. -

THE SOLUBILITY of GASES in LIQUIDS Introductory Information C
THE SOLUBILITY OF GASES IN LIQUIDS Introductory Information C. L. Young, R. Battino, and H. L. Clever INTRODUCTION The Solubility Data Project aims to make a comprehensive search of the literature for data on the solubility of gases, liquids and solids in liquids. Data of suitable accuracy are compiled into data sheets set out in a uniform format. The data for each system are evaluated and where data of sufficient accuracy are available values are recommended and in some cases a smoothing equation is given to represent the variation of solubility with pressure and/or temperature. A text giving an evaluation and recommended values and the compiled data sheets are published on consecutive pages. The following paper by E. Wilhelm gives a rigorous thermodynamic treatment on the solubility of gases in liquids. DEFINITION OF GAS SOLUBILITY The distinction between vapor-liquid equilibria and the solubility of gases in liquids is arbitrary. It is generally accepted that the equilibrium set up at 300K between a typical gas such as argon and a liquid such as water is gas-liquid solubility whereas the equilibrium set up between hexane and cyclohexane at 350K is an example of vapor-liquid equilibrium. However, the distinction between gas-liquid solubility and vapor-liquid equilibrium is often not so clear. The equilibria set up between methane and propane above the critical temperature of methane and below the criti cal temperature of propane may be classed as vapor-liquid equilibrium or as gas-liquid solubility depending on the particular range of pressure considered and the particular worker concerned. -

Henry's Law Constants and Micellar Partitioning of Volatile Organic
38 J. Chem. Eng. Data 2000, 45, 38-47 Henry’s Law Constants and Micellar Partitioning of Volatile Organic Compounds in Surfactant Solutions Leland M. Vane* and Eugene L. Giroux United States Environmental Protection Agency, National Risk Management Research Laboratory, 26 West Martin Luther King Drive, Cincinnati, Ohio 45268 Partitioning of volatile organic compounds (VOCs) into surfactant micelles affects the apparent vapor- liquid equilibrium of VOCs in surfactant solutions. This partitioning will complicate removal of VOCs from surfactant solutions by standard separation processes. Headspace experiments were performed to quantify the effect of four anionic surfactants and one nonionic surfactant on the Henry’s law constants of 1,1,1-trichloroethane, trichloroethylene, toluene, and tetrachloroethylene at temperatures ranging from 30 to 60 °C. Although the Henry’s law constant increased markedly with temperature for all solutions, the amount of VOC in micelles relative to that in the extramicellar region was comparatively insensitive to temperature. The effect of adding sodium chloride and isopropyl alcohol as cosolutes also was evaluated. Significant partitioning of VOCs into micelles was observed, with the micellar partitioning coefficient (tendency to partition from water into micelle) increasing according to the following series: trichloroethane < trichloroethylene < toluene < tetrachloroethylene. The addition of surfactant was capable of reversing the normal sequence observed in Henry’s law constants for these four VOCs. Introduction have long taken advantage of the high Hc values for these compounds. In the engineering field, the most common Vast quantities of organic solvents have been disposed method of dealing with chlorinated solvents dissolved in of in a manner which impacts human health and the groundwater is “pump & treat”swithdrawal of ground- environment. -

Dive Theory Guide
DIVE THEORY STUDY GUIDE by Rod Abbotson CD69259 © 2010 Dive Aqaba Guidelines for studying: Study each area in order as the theory from one subject is used to build upon the theory in the next subject. When you have completed a subject, take tests and exams in that subject to make sure you understand everything before moving on. If you try to jump around or don’t completely understand something; this can lead to gaps in your knowledge. You need to apply the knowledge in earlier sections to understand the concepts in later sections... If you study this way you will retain all of the information and you will have no problems with any PADI dive theory exams you may take in the future. Before completing the section on decompression theory and the RDP make sure you are thoroughly familiar with the RDP, both Wheel and table versions. Use the appropriate instructions for use guides which come with the product. Contents Section One PHYSICS ………………………………………………page 2 Section Two PHYSIOLOGY………………………………………….page 11 Section Three DECOMPRESSION THEORY & THE RDP….……..page 21 Section Four EQUIPMENT……………………………………………page 27 Section Five SKILLS & ENVIRONMENT…………………………...page 36 PHYSICS SECTION ONE Light: The speed of light changes as it passes through different things such as air, glass and water. This affects the way we see things underwater with a diving mask. As the light passes through the glass of the mask and the air space, the difference in speed causes the light rays to bend; this is called refraction. To the diver wearing a normal diving mask objects appear to be larger and closer than they actually are. -

Biomechanics of Safe Ascents Workshop
PROCEEDINGS OF BIOMECHANICS OF SAFE ASCENTS WORKSHOP — 10 ft E 30 ft TIME AMERICAN ACADEMY OF UNDERWATER SCIENCES September 25 - 27, 1989 Woods Hole, Massachusetts Proceedings of the AAUS Biomechanics of Safe Ascents Workshop Michael A. Lang and Glen H. Egstrom, (Editors) Copyright © 1990 by AMERICAN ACADEMY OF UNDERWATER SCIENCES 947 Newhall Street Costa Mesa, CA 92627 All Rights Reserved No part of this book may be reproduced in any form by photostat, microfilm, or any other means, without written permission from the publishers Copies of these Proceedings can be purchased from AAUS at the above address This workshop was sponsored in part by the National Oceanic and Atmospheric Administration (NOAA), Department of Commerce, under grant number 40AANR902932, through the Office of Undersea Research, and in part by the Diving Equipment Manufacturers Association (DEMA), and in part by the American Academy of Underwater Sciences (AAUS). The U.S. Government is authorized to produce and distribute reprints for governmental purposes notwithstanding the copyright notation that appears above. Opinions presented at the Workshop and in the Proceedings are those of the contributors, and do not necessarily reflect those of the American Academy of Underwater Sciences PROCEEDINGS OF THE AMERICAN ACADEMY OF UNDERWATER SCIENCES BIOMECHANICS OF SAFE ASCENTS WORKSHOP WHOI/MBL Woods Hole, Massachusetts September 25 - 27, 1989 MICHAEL A. LANG GLEN H. EGSTROM Editors American Academy of Underwater Sciences 947 Newhall Street, Costa Mesa, California 92627 U.S.A. An American Academy of Underwater Sciences Diving Safety Publication AAUSDSP-BSA-01-90 CONTENTS Preface i About AAUS ii Executive Summary iii Acknowledgments v Session 1: Introductory Session Welcoming address - Michael A. -
Carbon Dioxide Capture by Chemical Absorption: a Solvent Comparison Study
Carbon Dioxide Capture by Chemical Absorption: A Solvent Comparison Study by Anusha Kothandaraman B. Chem. Eng. Institute of Chemical Technology, University of Mumbai, 2005 M.S. Chemical Engineering Practice Massachusetts Institute of Technology, 2006 SUBMITTED TO THE DEPARTMENT OF CHEMICAL ENGINEERING IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN CHEMICAL ENGINEERING PRACTICE AT THE MASSACHUSETTS INSTITUTE OF TECHNOLOGY JUNE 2010 © 2010 Massachusetts Institute of Technology All rights reserved. Signature of Author……………………………………………………………………………………… Department of Chemical Engineering May 20, 2010 Certified by……………………………………………………….………………………………… Gregory J. McRae Hoyt C. Hottel Professor of Chemical Engineering Thesis Supervisor Accepted by……………………………………………………………………………….................... William M. Deen Carbon P. Dubbs Professor of Chemical Engineering Chairman, Committee for Graduate Students 1 2 Carbon Dioxide Capture by Chemical Absorption: A Solvent Comparison Study by Anusha Kothandaraman Submitted to the Department of Chemical Engineering on May 20, 2010 in partial fulfillment of the requirements of the Degree of Doctor of Philosophy in Chemical Engineering Practice Abstract In the light of increasing fears about climate change, greenhouse gas mitigation technologies have assumed growing importance. In the United States, energy related CO2 emissions accounted for 98% of the total emissions in 2007 with electricity generation accounting for 40% of the total1. Carbon capture and sequestration (CCS) is one of the options that can enable the utilization of fossil fuels with lower CO2 emissions. Of the different technologies for CO2 capture, capture of CO2 by chemical absorption is the technology that is closest to commercialization. While a number of different solvents for use in chemical absorption of CO2 have been proposed, a systematic comparison of performance of different solvents has not been performed and claims on the performance of different solvents vary widely. -

THE SOLUBILITY of GASES in LIQUIDS INTRODUCTION the Solubility Data Project Aims to Make a Comprehensive Search of the Lit- Erat
THE SOLUBILITY OF GASES IN LIQUIDS R. Battino, H. L. Clever and C. L. Young INTRODUCTION The Solubility Data Project aims to make a comprehensive search of the lit erature for data on the solubility of gases, liquids and solids in liquids. Data of suitable accuracy are compiled into data sheets set out in a uni form format. The data for each system are evaluated and where data of suf ficient accuracy are available values recommended and in some cases a smoothing equation suggested to represent the variation of solubility with pressure and/or temperature. A text giving an evaluation and recommended values and the compiled data sheets are pUblished on consecutive pages. DEFINITION OF GAS SOLUBILITY The distinction between vapor-liquid equilibria and the solUbility of gases in liquids is arbitrary. It is generally accepted that the equilibrium set up at 300K between a typical gas such as argon and a liquid such as water is gas liquid solubility whereas the equilibrium set up between hexane and cyclohexane at 350K is an example of vapor-liquid equilibrium. However, the distinction between gas-liquid solUbility and vapor-liquid equilibrium is often not so clear. The equilibria set up between methane and propane above the critical temperature of methane and below the critical temperature of propane may be classed as vapor-liquid equilibrium or as gas-liquid solu bility depending on the particular range of pressure considered and the par ticular worker concerned. The difficulty partly stems from our inability to rigorously distinguish between a gas, a vapor, and a liquid, which has been discussed in numerous textbooks. -

Effect of Surfactant on Interfacial Gas Transfer Studied by Axisymmetric Drop Shape Analysis-Captive Bubble (ADSA-CB)
5446 Langmuir 2005, 21, 5446-5452 Effect of Surfactant on Interfacial Gas Transfer Studied by Axisymmetric Drop Shape Analysis-Captive Bubble (ADSA-CB) Yi Y. Zuo,† Dongqing Li,† Edgar Acosta,‡ Peter N. Cox,§ and A. Wilhelm Neumann*,† Department of Mechanical and Industrial Engineering, University of Toronto, 5 King’s College Road, Toronto, ON, M5S 3G8, Canada, Department of Chemical Engineering and Applied Chemistry, University of Toronto, 200 College Street, Toronto, ON, M5S 3E5, Canada, and Department of Critical Care Medicine, The Hospital for Sick Children, 555 University Avenue, Toronto, ON, M5G 1X8, Canada Received January 31, 2005. In Final Form: April 3, 2005 A new method combining axisymmetric drop shape analysis (ADSA) and a captive bubble (CB) is proposed to study the effect of surfactant on interfacial gas transfer. In this method, gas transfer from a static CB to the surrounding quiescent liquid is continuously recorded for a short period (i.e., 5 min). By photographical analysis, ADSA-CB is capable of yielding detailed information pertinent to the surface tension and geometry of the CB, e.g., bubble area, volume, curvature at the apex, and the contact radius and height of the bubble. A steady-state mass transfer model is established to evaluate the mass transfer coefficient on the basis of the output of ADSA-CB. In this way, we are able to develop a working prototype capable of simultaneously measuring dynamic surface tension and interfacial gas transfer. Other advantages of this method are that it allows for the study of very low surface tensions (<5 mJ/m2) and does not require equilibrium of gas transfer. -
Biotransformation: Basic Concepts (1)
Chapter 5 Absorption, Distribution, Metabolism, and Elimination of Toxics Biotransformation: Basic Concepts (1) • Renal excretion of chemicals Biotransformation: Basic Concepts (2) • Biological basis for xenobiotic metabolism: – To convert lipid-soluble, non-polar, non-excretable forms of chemicals to water-soluble, polar forms that are excretable in bile and urine. – The transformation process may take place as a result of the interaction of the toxic substance with enzymes found primarily in the cell endoplasmic reticulum, cytoplasm, and mitochondria. – The liver is the primary organ where biotransformation occurs. Biotransformation: Basic Concepts (3) Biotransformation: Basic Concepts (4) • Interaction with these enzymes may change the toxicant to either a less or a more toxic form. • Generally, biotransformation occurs in two phases. – Phase I involves catabolic reactions that break down the toxicant into various components. • Catabolic reactions include oxidation, reduction, and hydrolysis. – Oxidation occurs when a molecule combines with oxygen, loses hydrogen, or loses one or more electrons. – Reduction occurs when a molecule combines with hydrogen, loses oxygen, or gains one or more electrons. – Hydrolysis is the process in which a chemical compound is split into smaller molecules by reacting with water. • In most cases these reactions make the chemical less toxic, more water soluble, and easier to excrete. Biotransformation: Basic Concepts (5) – Phase II reactions involves the binding of molecules to either the original toxic molecule or the toxic molecule metabolite derived from the Phase I reactions. The final product is usually water soluble and, therefore, easier to excrete from the body. • Phase II reactions include glucuronidation, sulfation, acetylation, methylation, conjugation with glutathione, and conjugation with amino acids (such as glycine, taurine, and glutamic acid).