Towards a Detailed Understanding of the Red Blood Cell Storage Lesion
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
IFM Innate Immunity Infographic
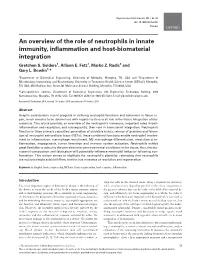
UNDERSTANDING INNATE IMMUNITY INTRODUCTION The immune system is comprised of two arms that work together to protect the body – the innate and adaptive immune systems. INNATE ADAPTIVE γδ T Cell Dendritic B Cell Cell Macrophage Antibodies Natural Killer Lymphocites Neutrophil T Cell CD4+ CD8+ T Cell T Cell TIME 6 hours 12 hours 1 week INNATE IMMUNITY ADAPTIVE IMMUNITY Innate immunity is the body’s first The adaptive, or acquired, immune line of immunological response system is activated when the innate and reacts quickly to anything that immune system is not able to fully should not be present. address a threat, but responses are slow, taking up to a week to fully respond. Pathogen evades the innate Dendritic immune system T Cell Cell Through antigen Pathogen presentation, the dendritic cell informs T cells of the pathogen, which informs Macrophage B cells B Cell B cells create antibodies against the pathogen Macrophages engulf and destroy Antibodies label invading pathogens pathogens for destruction Scientists estimate innate immunity comprises approximately: The adaptive immune system develops of the immune memory of pathogen exposures, so that 80% system B and T cells can respond quickly to eliminate repeat invaders. IMMUNE SYSTEM AND DISEASE If the immune system consistently under-responds or over-responds, serious diseases can result. CANCER INFLAMMATION Innate system is TOO ACTIVE Innate system NOT ACTIVE ENOUGH Cancers grow and spread when tumor Certain diseases trigger the innate cells evade detection by the immune immune system to unnecessarily system. The innate immune system is respond and cause excessive inflammation. responsible for detecting cancer cells and This type of chronic inflammation is signaling to the adaptive immune system associated with autoimmune and for the destruction of the cancer cells. -

In Vitro Induction of Erythrocyte Phosphatidylserine Translocation by the Natural Naphthoquinone Shikonin
Toxins 2014, 6, 1559-1574; doi:10.3390/toxins6051559 OPEN ACCESS toxins ISSN 2072-6651 www.mdpi.com/journal/toxins Article In Vitro Induction of Erythrocyte Phosphatidylserine Translocation by the Natural Naphthoquinone Shikonin Adrian Lupescu, Rosi Bissinger, Kashif Jilani and Florian Lang * Department of Physiology, University of Tuebingen, Gmelinstreet 5, Tuebingen 72076, Germany; E-Mails: [email protected] (A.L.); [email protected] (R.B.); [email protected] (K.J.) * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +49-7071-297-2194; Fax: +49-7071-29-5618. Received: 4 March 2014; in revised form: 5 May 2014 / Accepted: 5 May 2014 / Published: 13 May 2014 Abstract: Shikonin, the most important component of Lithospermum erythrorhizon, has previously been shown to exert antioxidant, anti-inflammatory, antithrombotic, antiviral, antimicrobial and anticancer effects. The anticancer effect has been attributed to the stimulation of suicidal cell death or apoptosis. Similar to the apoptosis of nucleated cells, erythrocytes may experience eryptosis, the suicidal erythrocyte death characterized by cell shrinkage and by phosphatidylserine translocation to the erythrocyte surface. Triggers of 2+ 2+ eryptosis include the increase of cytosolic Ca -activity ([Ca ]i) and ceramide formation. The present study explored whether Shikonin stimulates eryptosis. To this end, Fluo 3 2+ fluorescence was measured to quantify [Ca ]i, forward scatter to estimate cell volume, annexin V binding to identify phosphatidylserine-exposing erythrocytes, hemoglobin release to determine hemolysis and antibodies to quantify ceramide abundance. As a result, 2+ a 48 h exposure of human erythrocytes to Shikonin (1 µM) significantly increased [Ca ]i, increased ceramide abundance, decreased forward scatter and increased annexin V binding. -

1 Induction of Eryptosis in Red Blood Cells Using a Calcium Ionophore 2
1 TITLE: 2 Induction of Eryptosis in Red Blood Cells Using a Calcium Ionophore 3 4 AUTHORS AND AFFILIATIONS: 5 Parnian Bigdelou1, Amir M. Farnoud1 6 1Department of Chemical and Biomolecular Engineering, Ohio University, Athens, OH, USA 7 8 Corresponding Author: 9 Amir M. Farnoud ([email protected]) 10 11 Email Address of Co-author: 12 Parnian Bigdelou ([email protected]) 13 14 KEYWORDS: 15 erythrocyte, eryptosis, phosphatidylserine, annexin V, ionomycin, cell membrane 16 17 SUMMARY: 18 A protocol for the induction of eryptosis, programmed cell death in erythrocytes, using the 19 calcium ionophore, ionomycin, is provided. Successful eryptosis is evaluated by monitoring the 20 localization phosphatidylserine in the membrane outer leaflet. Factors affecting the success of 21 the protocol have been examined and optimal conditions provided. 22 23 ABSTRACT: 24 Eryptosis, erythrocyte programmed cell death, occurs in a number of hematological diseases 25 and during injury to erythrocytes. A hallmark of eryptotic cells is the loss of compositional 26 asymmetry of the cell membrane, leading to the translocation of phosphatidylserine to the 27 membrane outer leaflet. This process is triggered by increased intracellular concentration of 28 Ca2+, which activates scramblase, an enzyme that facilitates bidirectional movement of 29 phospholipids between membrane leaflets. Given the importance of eryptosis in various 30 diseased conditions, there have been efforts to induce eryptosis in vitro. Such efforts have 31 generally relied on the calcium ionophore, ionomycin, to enhance intracellular Ca2+ 32 concentration and induce eryptosis. However, many discrepancies have been reported in the 33 literature regarding the procedure for inducing eryptosis using ionomycin. -

Influence of Oxidative Stress on Erythrocyte's Formation And
IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-ISSN: 2320–1959.p- ISSN: 2320–1940 Volume 9, Issue 4 Ser. I (Jul. – Aug. 2020), PP 37-43 www.iosrjournals.org Influence Of Oxidative Stress On Erythrocyte’s Formation And Function Resulting In Anemia Irha Basit1, Ayesha Aziz2, Rabia Azam1*, Humera Aziz3, Safoora Shabbir2, Noor Fatima4 , Kiran Liaqat4, Raheela Fatima4 1 Department of Biochemistry, University of Agriculture, Faisalabad, Pakistan 2 Department of Biochemistry, Government College University, Faisalabad, Pakistan 3 Department of Environmental Sciences and Engineering, Government College University, Faisalabad, Pakistan 4 Faculty of Pharmaceutical Sciences, Government College University, Faisalabad, Pakistan *Corresponding author: (Rabia Azam,) Abstract Anemia is a condition with a reduced amount of total blood cell (RBC) or blood hemoglobin or reduced blood oxygen-carrying capacity. Blood loss, decreased production of red blood cells and increased breakdown of red blood cells can cause anemia. Trauma and gastrointestinal bleeding are a source of blood loss, but certain factors, including iron deficiency, vitamin B12 deficiency, lower erythropoietin level, slight bone marrow neoplasm thalassemia, genetic disorders such as sickle cell, parasitic infection including malariaand other autoimmune diseases are the causes of lower erythrocytes. Anemia is also associated with oxidative stress owing to two processes. Oxidative stress affects the function of the kidney resulting in lower erythropoietin production, which ultimately affects erythropoiesis and therefore reduces erythrocyte production. In other way, oxidative stress also reduces the amount of erythrocyte by increasing the rate of programmed cell death of erythrocytes (eryptosis) by activating the calcium channels and cell loss of KCl. This review provides insight into the mechanism followed by oxidative stress to reduce the amounts of erythrocytes in the body resulting in the development of anemia. -

Balance Between Innate Versus Adaptive Immune System and the Risk of Dementia: a Population-Based Cohort Study Kimberly D
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Erasmus University Digital Repository Willik et al. Journal of Neuroinflammation (2019) 16:68 https://doi.org/10.1186/s12974-019-1454-z RESEARCH Open Access Balance between innate versus adaptive immune system and the risk of dementia: a population-based cohort study Kimberly D. van der Willik1,2†, Lana Fani1†, Dimitris Rizopoulos3, Silvan Licher1, Jesse Fest4, Sanne B. Schagen2,5, M. Kamran Ikram1,6† and M. Arfan Ikram1*† Abstract Background: Immunity has been suggested to be important in the pathogenesis of dementia. However, the contribution of innate versus adaptive immunity in the development of dementia is not clear. In this study, we aimed to investigate (1) the association between components of innate immunity (granulocytes and platelets) and adaptive immunity (lymphocytes) with risk of dementia and (2) the association between their derived ratios (granulocyte-to-lymphocyte ratio [GLR], platelet-to-lymphocyte ratio [PLR], and systemic immune-inflammation index [SII]), reflecting the balance between innate and adaptive immunity, with risk of dementia. Methods: Blood cell counts were measured repeatedly between 2002 and 2015 in dementia-free participants of the prospective population-based Rotterdam Study. Participants were followed-up for dementia until 1 January 2016. Joint models were used to determine the association between granulocyte, platelets, and lymphocyte counts, and their derived ratios with risk of dementia. Results: Of the 8313 participants (mean [standard deviation] age 61.1 [7.4] years, 56.9% women), 664 (8.0%) developed dementia during a median follow-up of 8.6 years. -
An Overview of the Role of Neutrophils in Innate Immunity, Inflammation and Host-Biomaterial Integration Gretchen S
Regenerative Biomaterials, 2017, 55–68 doi: 10.1093/rb/rbw041 Review An overview of the role of neutrophils in innate immunity, inflammation and host-biomaterial integration Gretchen S. Selders1, Allison E. Fetz1, Marko Z. Radic2 and Gary L. Bowlin1,* 1Department of Biomedical Engineering, University of Memphis, Memphis, TN, USA and 2Department of Microbiology, Immunology and Biochemistry, University of Tennessee Health Science Center (UTHSC), Memphis, TN, USA, 858 Madison Ave, Room 201 Molecular Science Building, Memphis, TN 38163, USA *Correspondence address. Department of Biomedical Engineering, 330 Engineering Technology Building, 3806 Norriswood Ave. Memphis, TN 38152, USA. Tel: (901)678-2670; Fax: (901) 678-5281; E-mail:[email protected] Received 26 September 2016; revised 14 October 2016; accepted on 19 October 2016 Abstract Despite considerable recent progress in defining neutrophil functions and behaviors in tissue re- pair, much remains to be determined with regards to its overall role in the tissue integration of bio- materials. This article provides an overview of the neutrophil’s numerous, important roles in both inflammation and resolution, and subsequently, their role in biomaterial integration. Neutrophils function in three primary capacities: generation of oxidative bursts, release of granules and forma- tion of neutrophil extracellular traps (NETs); these combined functions enable neutrophil involve- ment in inflammation, macrophage recruitment, M2 macrophage differentiation, resolution of in- flammation, angiogenesis, tumor formation and immune system activation. Neutrophils exhibit great flexibility to adjust to the prevalent microenvironmental conditions in the tissue; thus, the bio- material composition and fabrication will potentially influence neutrophil behavior following con- frontation. This review serves to highlight the neutrophil’s plasticity, reiterating that neutrophils are not just simple suicidal killers, but the true maestros of resolution and regeneration. -

Inborn Defects in the Antioxidant Systems of Human Red Blood Cells
Free Radical Biology and Medicine 67 (2014) 377–386 Contents lists available at ScienceDirect Free Radical Biology and Medicine journal homepage: www.elsevier.com/locate/freeradbiomed Review Article Inborn defects in the antioxidant systems of human red blood cells Rob van Zwieten a,n, Arthur J. Verhoeven b, Dirk Roos a a Laboratory of Red Blood Cell Diagnostics, Department of Blood Cell Research, Sanquin Blood Supply Organization, 1066 CX Amsterdam, The Netherlands b Department of Medical Biochemistry, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands article info abstract Article history: Red blood cells (RBCs) contain large amounts of iron and operate in highly oxygenated tissues. As a result, Received 16 January 2013 these cells encounter a continuous oxidative stress. Protective mechanisms against oxidation include Received in revised form prevention of formation of reactive oxygen species (ROS), scavenging of various forms of ROS, and repair 20 November 2013 of oxidized cellular contents. In general, a partial defect in any of these systems can harm RBCs and Accepted 22 November 2013 promote senescence, but is without chronic hemolytic complaints. In this review we summarize the Available online 6 December 2013 often rare inborn defects that interfere with the various protective mechanisms present in RBCs. NADPH Keywords: is the main source of reduction equivalents in RBCs, used by most of the protective systems. When Red blood cells NADPH becomes limiting, red cells are prone to being damaged. In many of the severe RBC enzyme Erythrocytes deficiencies, a lack of protective enzyme activity is frustrating erythropoiesis or is not restricted to RBCs. Hemolytic anemia Common hereditary RBC disorders, such as thalassemia, sickle-cell trait, and unstable hemoglobins, give G6PD deficiency Favism rise to increased oxidative stress caused by free heme and iron generated from hemoglobin. -

Extracellular Vesicles in Innate Immune Cell Programming
biomedicines Review Extracellular Vesicles in Innate Immune Cell Programming Naveed Akbar 1,* , Daan Paget 1,2 and Robin P. Choudhury 1 1 Radcliffe Department of Medicine, University of Oxford, Oxford OX3 9DU, UK; [email protected] (D.P.); [email protected] (R.P.C.) 2 Department of Pharmacology, University of Oxford, Oxford OX1 3QT, UK * Correspondence: [email protected] Abstract: Extracellular vesicles (EV) are a heterogeneous group of bilipid-enclosed envelopes that carry proteins, metabolites, RNA, DNA and lipids from their parent cell of origin. They mediate cellular communication to other cells in local tissue microenvironments and across organ systems. EV size, number and their biologically active cargo are often altered in response to pathological processes, including infection, cancer, cardiovascular diseases and in response to metabolic pertur- bations such as obesity and diabetes, which also have a strong inflammatory component. Here, we discuss the broad repertoire of EV produced by neutrophils, monocytes, macrophages, their pre- cursor hematopoietic stem cells and discuss their effects on the innate immune system. We seek to understand the immunomodulatory properties of EV in cellular programming, which impacts innate immune cell differentiation and function. We further explore the possibilities of using EV as immune targeting vectors, for the modulation of the innate immune response, e.g., for tissue preservation during sterile injury such as myocardial infarction or to promote tissue resolution of inflammation and potentially tissue regeneration and repair. Keywords: exosomes; transcription; neutrophil; monocyte; hematopoietic stem cell Citation: Akbar, N.; Paget, D.; Choudhury, R.P. Extracellular Vesicles in Innate Immune Cell Programming. -

Mast Cells in Infection and Immunity†
INFECTION AND IMMUNITY, Sept. 1997, p. 3501–3508 Vol. 65, No. 9 0019-9567/97/$04.0010 Copyright © 1997, American Society for Microbiology MINIREVIEW Mast Cells in Infection and Immunity† 1,2 2 SOMAN N. ABRAHAM * AND RAVI MALAVIYA Departments of Pathology and Molecular Microbiology, Washington University School of Medicine,1 and Department of Pathology, Barnes-Jewish Hospital of St. Louis,2 St. Louis, Missouri 63110 Mast cells remain one of the most enigmatic cells in the mediates binding of mast cells to parasitic helminths (46). body. These cells secrete significant amounts of numerous Parasitic helminths evoke a specific humoral immune response proinflammatory mediators which contribute to a number of in the host which involves, at least in part, the secretion of a chronic inflammatory conditions, including stress-induced in- large number of IgE antibodies (46). These antibodies become testinal ulceration, rheumatoid arthritis, interstitial cystitis, attached to mast cell surfaces because of the numerous IgE scleroderma, and Crohn’s disease (6, 14, 24, 76). Mast cells are receptors (FcεR) present on mast cell plasma membranes. also prominent in the development of anaphylaxis (14, 24, 76). Those IgE molecules that are specific for helminths then pro- Yet despite the negative effects of their secretions, mast cells mote mast cell binding to the parasite (56). Although IgE is not or mast cell-like cells have been described even among the commonly generated against bacteria, IgE specific to Helico- lowest order of animals (31). The phylogenic persistence of bacter pylori and Staphylococcus aureus has been reported in these cells through evolution strongly suggests that they are patients with peptic ulcers and atopic dermatitis, respectively beneficial in some fashion to the host. -

The Relationship Between COVID-19 and Innate Immunity in Children: a Review
children Review The Relationship between COVID-19 and Innate Immunity in Children: A Review Piero Valentini 1,2,3, Giorgio Sodero 1 and Danilo Buonsenso 2,3,4,*,† 1 Istituto di Pediatria, Università Cattolica del Sacro Cuore, 00168 Rome, Italy; [email protected] (P.V.); [email protected] (G.S.) 2 Department of Woman and Child Health and Public Health, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Rome, Italy 3 Global Health Research Institute, Istituto di Igiene, Università Cattolica del Sacro Cuore, 00168 Rome, Italy 4 Dipartimento di Scienze Biotecnologiche di Base, Cliniche Intensivologiche e Perioperatorie, Università Cattolica del Sacro Cuore, 00168 Rome, Italy * Correspondence: [email protected]; Tel.: +39-063-015-4390 † Current address: Danilo Buonsenso, Largo A. Gemelli 8, 00168 Rome, Italy. Abstract: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the virus responsible for the pandemic viral pneumonia that was first identified in Wuhan, China, in December 2019, and has since rapidly spread around the world. The number of COVID-19 cases recorded in pediatric age is around 1% of the total. The immunological mechanisms that lead to a lower susceptibility or severity of pediatric patients are not entirely clear. At the same time, the immune dysregulation found in those children who developed the multisystem inflammatory syndrome (MIC-S) is not yet fully understood. The aim of this review is to analyze the possible influence of children’s innate immune systems, considering the risk of contracting the virus, spreading it, and developing symptomatic disease or complications related to infection. Citation: Valentini, P.; Sodero, G.; Keywords: COVID-19; children; coronavirus; innate immunity; SARS-CoV-2; pandemic; MIC-S Buonsenso, D. -
The Innate Immune Response FUNCTIONS of the IMMUNE SYSTEM
The Innate Immune Response FUNCTIONS OF THE IMMUNE SYSTEM: • Recognize, destroy and clear a diversity of pathogens. • Initiate tissue and wound healing processes. • Recognize and clear damaged self components. Exhibit “tolerance” to innocuous material including self The Normal Immune Response The normal immune response is best understood in the context of defense against infectious pathogens, the classical definition of immunity. Innate immunity refers to defense mechanisms that have evolved to specifically recognize microbes and protect individuals against infections. Adaptive immunity consists of mechanisms that are stimulated and are capable of recognizing microbial and nonmicrobial substances. Innate immunity The first line of defense always ready to prevent and eradicate infections. Adaptive immunity Develops later, after exposure to microbes, and is even more powerful than innate immunity in combating infections. By convention, the term “immune response” refers to adaptive immunity. Innate and Adaptive immunity represent two different arms of the immune system that work together in host defense. Innate Immunity (natural/native): • Provides immediate protection from infection. • Is broadly specific to microbes and tissue damage products. • Does not change in response to reinfection (non-adaptive) • Initiates processes that lead to activation of adaptive immune responses. Adaptive Immunity (specific/acquired): • Appears to adapt to a variety of non-self components (acquired) • Is highly specific to a particular molecule “antigen” • Responses upon reinfection are faster, better and stronger (memory) • Generates proteins and cells that enhance innate immune function. http://classconnection.s3.amazonaws.com/536/flashcards/1317536/jpg/paneth_cell1332475911026.jpg INNATE IMMUNITY A major components of innate immunity are epithelial barriers that block entry of microbes. -

Ch33 WO Pt1.Pdf
33 Innate Host Resistance 1 33.1 Innate Resistance Overview 1. Identify the major components of the mammalian host immune system 2. Integrate the major immune components and their functions to explain in general terms how the immune system protects the host 2 Host Resistance Overview • Most pathogens (disease causing microbes) – must overcome surface barriers and reach underlying – overcome resistance by host • nonspecific resistance • specific immune response 3 Host Resistance Overview… • Immune system – composed of widely distributed cells, tissues, and organs – recognizes foreign substances or microbes and acts to neutralize or destroy them • Immunity – ability of host to resist a particular disease or infection • Immunology – science concerned with immune responses 4 Immunity • Nonspecific immune response – Aka nonspecific resistance, innate, or natural immunity – acts as a first line of defense – offers resistance to any microbe or foreign material – lacks immunological memory • Specific immune response – Aka acquired, adaptive, or specific immunity – resistance to a particular foreign agent – has “memory” • effectiveness increases on repeated exposure to agent 5 6 Antigens • Recognized as foreign • Invoke immune responses – presence of antigen in body ultimately results in B cell activation production of antibodies • antibodies bind to specific antigens, inactivating or eliminating them • other immune cells also become activated • Name comes from antibody generators 7 White Blood Cells of Innate and Adaptive Immunity • White blood