A Guide to Presenting Clinical Prediction Models for Use in the Clinical Setting Laura J Bonnett, Kym IE Snell, Gary S Collins, Richard D Riley
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Transforming Summary Statistics from Logistic Regression to the Liability Scale: Application To
bioRxiv preprint doi: https://doi.org/10.1101/385740; this version posted August 6, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Transforming summary statistics from logistic regression to the liability scale: application to genetic and environmental risk scores Alexandra C. Gilletta, Evangelos Vassosa, Cathryn M. Lewisa, b* a. Social, Genetic & Developmental Psychiatry Centre, Institute of Psychiatry, Psychology & Neuroscience, King’s College London, London, UK b. Department of Medical and Molecular Genetics, Faculty of Life Sciences and Medicine, King’s College London, London, UK Short Title: Transforming the odds ratio to the liability scale *Corresponding Author Cathryn M. Lewis Institute of Psychiatry, Psychology & Neuroscience Social, Genetic & Developmental Psychiatry Centre King’s College London 16 De Crespigny Park Denmark Hill, London, SE5 8AF, UK Tel: +44(0)20 7848 0873 Fax: +44(0)20 7848 0866 E-mail: [email protected] Keywords Statistical genetics, risk, logistic regression, liability threshold model, schizophrenia Page 1 bioRxiv preprint doi: https://doi.org/10.1101/385740; this version posted August 6, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1. Abstract 1.1. Objective Stratified medicine requires models of disease risk incorporating genetic and environmental factors. -
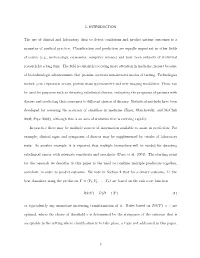
1. INTRODUCTION the Use of Clinical and Laboratory Data to Detect
1. INTRODUCTION The use of clinical and laboratory data to detect conditions and predict patient outcomes is a mainstay of medical practice. Classification and prediction are equally important in other fields of course (e.g., meteorology, economics, computer science) and have been subjects of statistical research for a long time. The field is currently receiving more attention in medicine, in part because of biotechnologic advancements that promise accurate non-invasive modes of testing. Technologies include gene expression arrays, protein mass spectrometry and new imaging modalities. These can be used for purposes such as detecting subclinical disease, evaluating the prognosis of patients with disease and predicting their responses to different choices of therapy. Statistical methods have been developed for assessing the accuracy of classifiers in medicine (Zhou, Obuchowski, and McClish 2002; Pepe 2003), although this is an area of statistics that is evolving rapidly. In practice there may be multiple sources of information available to assist in prediction. For example, clinical signs and symptoms of disease may be supplemented by results of laboratory tests. As another example, it is expected that multiple biomarkers will be needed for detecting subclinical cancer with adequate sensitivity and specificity (Pepe et al. 2001). The starting point for the research we describe in this paper is the need to combine multiple predictors together, somehow, in order to predict outcome. We note in Section 2 that for a binary outcome, D, the best classifiers using the predictors Y =(Y1,Y2,...,YP ) are based on the risk score function RS(Y )=P (D =1|Y ) (1) or equivalently any monotone increasing transformation of it. -

Support Vector Hazards Machine: a Counting Process Framework for Learning Risk Scores for Censored Outcomes
Journal of Machine Learning Research 17 (2016) 1-37 Submitted 1/16; Revised 7/16; Published 8/16 Support Vector Hazards Machine: A Counting Process Framework for Learning Risk Scores for Censored Outcomes Yuanjia Wang [email protected] Department of Biostatistics Mailman School of Public Health Columbia University New York, NY 10032, USA Tianle Chen [email protected] Biogen 300 Binney Street Cambridge, MA 02142, USA Donglin Zeng [email protected] Department of Biostatistics University of North Carolina at Chapel Hill Chapel Hill, NC 27599, USA Editor: Karsten Borgwardt Abstract Learning risk scores to predict dichotomous or continuous outcomes using machine learning approaches has been studied extensively. However, how to learn risk scores for time-to-event outcomes subject to right censoring has received little attention until recently. Existing approaches rely on inverse probability weighting or rank-based regression, which may be inefficient. In this paper, we develop a new support vector hazards machine (SVHM) approach to predict censored outcomes. Our method is based on predicting the counting process associated with the time-to-event outcomes among subjects at risk via a series of support vector machines. Introducing counting processes to represent time-to-event data leads to a connection between support vector machines in supervised learning and hazards regression in standard survival analysis. To account for different at risk populations at observed event times, a time-varying offset is used in estimating risk scores. The resulting optimization is a convex quadratic programming problem that can easily incorporate non- linearity using kernel trick. We demonstrate an interesting link from the profiled empirical risk function of SVHM to the Cox partial likelihood. -

Developing a Credit Risk Model Using SAS® Amos Taiwo Odeleye, TD Bank
Paper 3554-2019 Developing a Credit Risk Model Using SAS® Amos Taiwo Odeleye, TD Bank ABSTRACT A credit risk score is an analytical method of modeling the credit riskiness of individual borrowers (prospects and customers). While there are several generic, one-size-might-fit-all risk scores developed by vendors, there are numerous factors increasingly driving the development of in-house risk scores. This presentation introduces the audience to how to develop an in-house risk score using SAS®, reject inference methodology, and machine learning and data science methods. INTRODUCTION According to Frank H. Knight (1921), University of Chicago professor, risk can be thought of as any variability that can be quantified. Generally speaking, there are 4 steps in risk management, namely: Assess: Identify risk Quantify: Measure and estimate risk Manage: Avoid, transfer, mitigate, or eliminate Monitor: Evaluate the process and make necessary adjustment In the financial environment, risk can be classified in several ways. In 2017, I coined what I termed the C-L-O-M-O risk acronym: Credit Risk, e.g., default, recovery, collections, fraud Liquidity Risk, e.g., funding, refinancing, trading Operational Risk, e.g., bad actor, system or process interruption, natural disaster Market Risk, e.g., interest rate, foreign exchange, equity, commodity price Other Risk not already classified above e.g., Model risk, Reputational risk, Legal risk In the pursuit of international financial stability and cooperation, there are financial regulators at the global -

A Better Coefficient of Determination for Genetic Profile Analysis
A better coefficient of determination for genetic profile analysis Sang Hong Lee,1,* Michael E Goddard,2,3 Naomi R Wray,1,4 Peter M Visscher1,4,5 This is the peer reviewed version of the following article: Lee, S. H., M. E. Goddard, N. R. Wray and P. M. Visscher (2012). "A better coefficient of determination for genetic profile analysis." Genetic Epidemiology 36(3): 214-224, which has been published in final form at 10.1002/gepi.21614. This article may be used for non-commercial purposes in accordance with Wiley Terms and Conditions for self-archiving. 1Queensland Institute of Medical Research, 300 Herston Rd, Herston, QLD 4006, Australia; 2Biosciences Research Division, Department of Primary Industries, Victoria, Australia; 3Department of Agriculture and Food Systems, University of Melbourne, Melbourne, Australia; 4Queensland Brain Institute, University of Queensland, Brisbane, QLD 4072, Australia; 5Diamantina Institute, University of Queensland, Brisbane, QLD 4072, Australia Running head: A better coefficient of determination *Correspondence: Sang Hong Lee, 1Queensland Institute of Medical Research, 300 Herston Rd, Herston, QLD 4006, Australia. Tel: 61 7 3362 0168, [email protected] ABSTRACT Genome-wide association studies have facilitated the construction of risk predictors for disease from multiple SNP markers. The ability of such ‘genetic profiles’ to predict outcome is usually quantified in an independent data set. Coefficients of determination (R2) have been a useful measure to quantify the goodness-of-fit of the genetic profile. Various pseudo R2 measures for binary responses have been proposed. However, there is no standard or consensus measure because the concept of residual variance is not easily defined on the observed probability scale. -
Lecture 7 Risk Profile Scores Naomi Wray 2017 SISG Brisbane Module 10
2017 SISG Brisbane Module 10: Statistical & Quantitative Genetics of Disease Lecture 7 Risk profile scores Naomi Wray 1 Aims of Lecture 7 1. Statistics to evaluate risk profile scores a. Nagelkerke’s R2 b. AUC c. Decile Odds Ratio d. Variance explained on liability scale e. Risk stratification 2. Examples of Use of Risk Profile Scores 2 SNP profiling schematic Common pitfalls Discovery Target Variance of target Genome- GWAS sample phenotype Wide association explained by genotypes results predictor Select Apply Genomic profiles Evaluate top SNPs weighted sum of and risk alleles identify risk alleles Methods Methods to identify risk loci and estimate SNP effects Applications Visualising variation between individuals for common complex genetic diseases 15 12 17 12 19 16 12 7 12 8 12 11 4 SNP profiling schematic Common pitfalls Discovery Target Variance of target Genome- GWAS sample phenotype Wide association explained by genotypes results predictor Select Apply Genomic profiles Evaluate top SNPs weighted sum of and risk alleles identify risk alleles Methods Methods to identify risk loci and estimate SNP effects Applications Evaluate efficacy of score predictor Regression analysis: – y= phenotype, x = profile score. – Compare variance explained from the full model (with x) compared to a reduced model (covariates only). – Check the sign of the regression coefficient to determine if the relationship between y and x is in the expected direction. – BINARY TRAIT 6 First Application of Risk Profile Scoring 7 Purcell / ISC et al. Common polygenic variation contributes to risk of schizophrenia and bipolar disorder Nature 2009 Statistics to evaluate polygenic risk scoring 1. 1. Nagelkerke’s R2 – Pseudo-R2 statistic for logistic regression http://www.ats.ucla.edu/stat/mult_pkg/faq/general/Psuedo_RSquareds.htm Cox & Snell R2 Full model: y ~ covariates + score Logistic, y= case/control = 1/0 Reduced model: y ~ covariates N: sample size This definition gives R2 for a quantitative trait. -

Assessing Risk Score Calculation in the Presence of Uncollected Risk Factors
Assessing Risk Score Calculation in the Presence of Uncollected Risk Factors By Alice Toll Thesis Submitted to the Faculty of the Graduate School of Vanderbilt University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE in Biostatistics January 31, 2019 Nashville, Tennessee Approved: Dandan Liu, Ph.D. Qingxia Chen, Ph.D. TABLE OF CONTENTS Page LIST OF TABLES................................. iv LIST OF FIGURES ................................ v LIST OF ABBREVIATIONS........................... vi Chapter 1 Introduction................................... 1 2 Motivating Example .............................. 3 2.1 Framingham Stroke Risk Profile ..................... 3 2.2 Using Stroke Risk Scores in the Presence of Uncollected Risk Factors. 4 3 Methods..................................... 5 3.1 Cox Regression Models for Risk Prediction................ 5 3.2 Calculating Risk Scores .......................... 6 3.3 Performance Measures........................... 6 3.3.1 Correlation.............................. 6 3.3.2 C-Index................................ 6 3.3.3 IDI .................................. 7 3.3.4 Calibration.............................. 8 3.3.5 Differences in Predicted Risk.................... 9 4 Simulation Analysis............................... 10 4.1 Simulation Results for Performance Measures.............. 12 4.1.1 Correlation.............................. 12 4.1.2 C-Index................................ 12 4.1.3 IDI .................................. 12 4.1.4 Calibration............................. -

The Liability Threshold Model for Predicting the Risk of Cardiovascular Disease in Patients with Type 2 Diabetes: a Multi-Cohort Study of Korean Adults
H OH metabolites OH Article The Liability Threshold Model for Predicting the Risk of Cardiovascular Disease in Patients with Type 2 Diabetes: A Multi-Cohort Study of Korean Adults Eun Pyo Hong 1,2,3 , Seong Gu Heo 4 and Ji Wan Park 5,* 1 Molecular Neurogenetics Unit, Center for Genomic Medicine, Massachusetts General Hospital, Boston, MA 02114, USA; [email protected] 2 Department of Neurology, Harvard Medical School, Boston, MA 02115, USA 3 Medical and Population Genetics Program, the Broad Institute of M.I.T. and Harvard, Cambridge, MA 02142, USA 4 Yonsei Cancer Institute, College of Medicine, Yonsei University, Seoul 03722, Korea; [email protected] 5 Department of Medical Genetics, College of Medicine, Hallym University, Chuncheon, Gangwon-do 24252, Korea * Correspondence: [email protected] Abstract: Personalized risk prediction for diabetic cardiovascular disease (DCVD) is at the core of precision medicine in type 2 diabetes (T2D). We first identified three marker sets consisting of 15, 47, and 231 tagging single nucleotide polymorphisms (tSNPs) associated with DCVD using a linear mixed model in 2378 T2D patients obtained from four population-based Korean cohorts. Using the genetic variants with even modest effects on phenotypic variance, we observed improved risk stratification accuracy beyond traditional risk factors (AUC, 0.63 to 0.97). With a cutoff point of 0.21, the discrete genetic liability threshold model consisting of 231 SNPs (GLT231) correctly classified 87.7% of 2378 T2D patients as high or low risk of DCVD. For the same set of SNP markers, the GLT and polygenic risk score (PRS) models showed similar predictive performance, and we observed consistency between the GLT and PRS models in that the model based on a larger number Citation: Hong, E.P.; Heo, S.G.; Park, of SNP markers showed much-improved predictability. -

Developing Credit Risk Score Using Sas Programming 1
(c)2018 Amos OdeleyeAmos (c)2018 DEVELOPING CREDIT RISK SCORE USING SAS PROGRAMMING 1 Presenter: Amos Odeleye DISCLAIMER Opinions expressed are strictly and wholly of the presenter and not of SAS, FICO, Credit Bureau, past employers, current employer or any of their affiliates OdeleyeAmos (c)2018 SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc. in the USA and other countries Other brand and product names are trademarks of their respective companies 2 Credit Bureau or Credit Reporting Agency (CRA): Experian, Equifax or Transunion ABOUT THIS PRESENTATION Presented at Philadelphia-area SAS User Group (PhilaSUG) Fall 2018 meeting: OdeleyeAmos (c)2018 Date: TUESDAY, October 30th, 2018 Venue: Janssen (Pharmaceutical Companies of Johnson & Johnson) This presentation is an introductory guide on how to develop an in- house Credit Risk Score using SAS programming Your comment and question are welcomed, you can reach me via email: [email protected] 3 ABSTRACT Credit Risk Score is an analytical method of modeling the credit riskiness of individual borrowers – prospects and existing customers. OdeleyeAmos (c)2018 While there are numerous generic, one-size-fit-all Credit Risk scores developed by vendors, there are several factors increasingly driving the development of in-house Credit Risk Score. This presentation will introduce the audience on how to develop an in-house Credit Risk Score using SAS programming, Reject inference methodology, and Logistic Regression. -

Research Methods & Reporting
RESEARCH METHODS & REPORTING Prognosis and prognostic research: Developing a prognostic model Patrick Royston, 1 Karel G M Moons, 2 Douglas G Altman, 3 Yvonne Vergouwe 2 In the second article in their series, Patrick Royston and colleagues describe different approaches to building clinical prognostic models 1MRC Clinical Trials Unit, London The first article in this series reviewed why prognosis is Box 2 | Modelling continuous predictors NW1 2DA important and how it is practised in different medical Simple predictor transformations intended to detect and 2Julius Centre for Health Sciences settings. 1 We also highlighted the difference between model non-linearity can be systematically identified using, and Primary Care, University multivariable models used in aetiological research and Medical Centre Utrecht, Utrecht, for example, fractional polynomials, a generalisation of Netherlands those used in prognostic research and outlined the conventional polynomials (linear, quadratic, etc). 6 27 Power 3Centre for Statistics in Medicine, design characteristics for studies developing a prognostic transformations of a predictor beyond squares and cubes, University of Oxford, Oxford model. In this article we focus on developing a multi- including reciprocals, logarithms, and square roots are OX2 6UD variable prognostic model. We illustrate the statistical Correspondence to: P Royston allowed. These transformations contain a single term, [email protected] issues using a logistic regression model to predict the but to enhance flexibility can be extended to two term 2 Accepted: 6 October 2008 risk of a specific event. The principles largely apply to all models (eg, terms in log x and x ). Fractional polynomial multivariable regression methods, including models for functions can successfully model non-linear relationships Cite this as: BMJ 2009;338:b604 continuous outcomes and for time to event outcomes. -

Chapter 10. Considerations for Statistical Analysis
Chapter 10. Considerations for Statistical Analysis Patrick G. Arbogast, Ph.D. (deceased) Kaiser Permanente Northwest, Portland, OR Tyler J. VanderWeele, Ph.D. Harvard School of Public Health, Boston, MA Abstract This chapter provides a high-level overview of statistical analysis considerations for observational comparative effectiveness research (CER). Descriptive and univariate analyses can be used to assess imbalances between treatment groups and to identify covariates associated with exposure and/or the study outcome. Traditional strategies to adjust for confounding during the analysis include linear and logistic multivariable regression models. The appropriate analytic technique is dictated by the characteristics of the study outcome, exposure of interest, study covariates, and the underlying assumptions underlying the statistical model. Increasingly common in CER is the use of propensity scores, which assign a probability of receiving treatment, conditional on observed covariates. Propensity scores are appropriate when adjusting for large numbers of covariates and are particularly favorable in studies having a common exposure and rare outcome(s). Disease risk scores estimate the probability or rate of disease occurrence as a function of the covariates and are preferred in studies with a common outcome and rare exposure(s). Instrumental variables, which are measures that are causally related to exposure but only affect the outcome through the treatment, offer an alternative to analytic strategies that have incomplete information on potential unmeasured confounders. Missing data in CER studies is not uncommon, and it is important 135 to characterize the patterns of missingness in order to account for the missing data in the analysis. In addition, time-varying exposures and covariates should be accounted for to avoid bias. -
Credit Risk Evaluation Modeling – Analysis – Management
Credit Risk Evaluation Modeling – Analysis – Management INAUGURAL-DISSERTATION ZUR ERLANGUNG DER WÜRDE EINES DOKTORS DER WIRTSCHAFTSWISSENSCHAFTEN DER WIRTSCHAFTSWISSENSCHAFTLICHEN FAKULTÄT DER RUPRECHT-KARLS-UNIVERSITÄT HEIDELBERG VORGELEGT VON UWE WEHRSPOHN AUS EPPINGEN HEIDELBERG, JULI 2002 This monography is available in e-book-format at http://www.risk-and-evaluation.com. This monography was accepted as a doctoral thesis at the faculty of economics at Heidelberg University, Ger- many. © 2002 Center for Risk & Evaluation GmbH & Co. KG Berwanger Straße 4 D-75031 Eppingen www.risk-and-evaluation.com 2 Acknowledgements My thanks are due to Prof. Dr. Hans Gersbach for lively discussions and many ideas that con- tributed essentially to the success of this thesis. Among the many people who provided valuable feedback I would particularly like to thank Prof. Dr. Eva Terberger, Dr. Jürgen Prahl, Philipp Schenk, Stefan Lange, Bernard de Wit, Jean-Michel Bouhours, Frank Romeike, Jörg Düsterhaus and many colleagues at banks and consulting companies for countless suggestions and remarks. They assisted me in creating the awareness of technical, mathematical and economical problems which helped me to formulate and realize the standards that render credit risk models valuable and efficient in banks and financial institutions. Further, I gratefully acknowledge the profound support from Gertrud Lieblein and Computer Sciences Corporation – CSC Ploenzke AG that made this research project possible. My heartfelt thank also goes to my wife Petra for her steady encouragement to pursue this extensive scientific work. Uwe Wehrspohn 3 Introduction In the 1990ies, credit risk has become the major concern of risk managers in financial institu- tions and of regulators.