Leadership Named for 128Th Ohio General Assembly
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OMA Government Affairs Committee Meeting Materials
Table of Contents Page # Government Affairs Agenda 3 Manufacturers’ Evening Invitation 4 Committee Guest Bios 5 March 14, 2012 OMA Counsel Report Tort Reform Case Decision: Havel v. Villa St. 8 Joseph Marijuana Ballot Initiatives and Potential 10 Concerns for Ohio Manufacturers Ohio Supreme Court Contest 2012 13 Election Results List by Hannah News 14 Public Policy Report 19 Leadership News Articles 21 Legislative Update 32 Announcing the Ohio Steel Council 40 Ohio Prosperity Project 2012 Participant Engagement 41 Summit NAM Public Affairs Conference 2012 43 Energy 48 Environment 80 Tax 100 Workers’ Compensation 115 Human Resources 124 2012 Government Affairs OMA Government Affairs Committee Meeting Sponsor: Committee Calendar Wednesday, March 14, 2012 Wednesday, June 6, 2012 Thursday, September 20, 2012 Wednesday, November 14, 2012 Additional committee meetings or teleconferences, if needed, will be scheduled at the call of the Chair. Page 1 of 133 Page 2 of 133 OMA Government Affairs Committee March 14, 2012 AGENDA Welcome & Self-Introductions Jeff Fritz DuPont Committee Chair Ohio Primary Election Review Federal Highlights Barry Doggett Boiler & Utility MACT / NAM Conference Eaton Corporation NAM Regional Vice Chair OMA Counsel’s Report Kurt Tunnell Civil Justice / Ballot Issues / Supreme Court Bricker & Eckler, LLP Extended Producer Responsibility (EPR) Luke Harms New State Level Trend Whirlpool Manufacturing Advocacy Robert Lapp Ohio Steel Council Formed, Vertical Groups & OMA, The Timken Company Ohio Prosperity Project Food Manufacturing Dialogue Lee Anderson General Mills Staff Reports Ryan Augsburger Tax, Workers’ Comp, Energy, Environment The Ohio Manufacturers’ Association Kevin Schmidt The Ohio Manufacturers’ Association Honorable Ross McGregor Special Guests Ohio House of Representatives Honorable Kristina Roegner Ohio House of Representatives Workplace Freedom Polling Presentation Jeff Longstreth Ohio 2.0 Hans Kaiser Moore Information Committee Meetings begin at 10:00 a.m. -

Bulletin Ohio Oil and Gas Association Visit Us Online At
Volume 63, Number 1, January/February 2013 Bulletin Ohio Oil and Gas Association Visit us online at www.ooga.org State Budget Debate Governor Presses Severance Tax Increase in Upcoming State Budget Debate By: Brian Hickman hio Governor John Kasich (R) has been you know what they say? We should take this and run. But then they get Opressing his desire to increase the severance their lobbyists and all these other people and they obscure the issue.” tax on Ohio oil and gas production in recent media interviews ahead of the upcoming state budget debate. In these interviews, Kasich has mentioned A key focus of the Governor’s plan has been a reduction that accepting a proposal might be a better option of the state’s 5.9% income tax. than facing a potential ballot initiative that would create a higher increase in taxes. To achieve this goal, the Governor continues to push an increase in severance taxes levied on oil and gas In recent year-end interviews with the media, production from horizontal wells. Kasich has been setting the tone for the upcoming budget debate. He made it clear that the upcoming budget covering fiscal years 2014-2015 Kasich then went on to mention that the industry might want to consider will deal with a new formula along with a system the fact that, if a severance tax increase is not agreed to, a ballot initiative of comprehensive tax reforms for the state of may be started to achieve this goal. “Nobody’s talking about an 8 percent Ohio. -

April 2021 Monthly Legislative Update
Mid-Ohio Regional Planning Commission Monthly Legislative Update April 2021 Joseph Garrity Director of Government Affairs + Strategic Initiatives (614) 233-4127 [email protected] What’s Happening Governor Signs Transportation Budget Gov. Mike DeWine signed the more than $8 billion transportation budget bill last week. The governor highlighted $318 million included for highway safety projects, $2.4 billion for local roadway improvements and $8 million for electric vehicle charging station grants. Speaker Bob Cupp (R-Lima) called passage of the bill “a good day for the state of Ohio and people of Ohio,” adding that it was passed on time, within the available revenue, “and without a contentious conference committee.” The House action came one day after the Ohio Senate adopted an omnibus amendment to the bill and passed it on the floor in a 32-0 vote. The bill funds construction and maintenance of the state’s roadways and bridges, in addition to appropriating $70 million per year for public transit through a combination of General Revenue Fund and federal flex funds. However, Governor DeWine’s “Hands-Free Ohio” proposal to increase penalties for distracted driving was removed by the General Assembly upon final passage of the bill. This proposal may be brought forward as a standalone bill later this session. Transportation budgets generally must be passed by the end of March so the non-appropriations sections can become effective 90 days later, by July 1, the start of the new fiscal year. Biden Announces American Jobs Plan Last week, President Biden introduced his American Jobs Plan in Pittsburgh. -

Ohio Senate Journal
JOURNALS OF THE SENATE AND HOUSE OF REPRESENTATIVES OHIO SENATE JOURNAL WEDNESDAY, OCTOBER 9, 2019 SENATE JOURNAL, WEDNESDAY, OCTOBER 9, 2019 1261 ONE HUNDRED TWELFTH DAY Senate Chamber, Columbus, Ohio Wednesday, October 9, 2019, 1:30 p.m. The Senate met pursuant to adjournment. Prayer was offered by Pastor Brian Hanson, Grace Baptist Church in Cedarville, Ohio, followed by the Pledge of Allegiance to the Flag. The journal of the last legislative day was read and approved. The following guests were recognized by the Senate prior to the commencement of business: Senator Craig honored Franklin County Public Health on its 100th Anniversary. Senator Antonio recognized Mike and Jaret Gold on their visit to the Statehouse. Senator Craig recognized Hailey Kaye as a new staff member in his office. Senator Hottinger recognized Annie Bowen on her visit to the Statehouse. Senator Peterson requested a moment of silence in memory of Bret Wiseman. On the motion of Senator Peterson, the Senate advanced to the ninth order of business. OFFERING OF RESOLUTIONS Senators Obhof and Peterson offered the following resolution: S. R. No. 382-Senators Obhof, Peterson. Relative to the election of Louis W. Blessing III, to fill the vacancy in the membership of the Senate created by the resignation of Lou Terhar of the 8th Senatorial District. WHEREAS, Section 11 of Article II of the Ohio Constitution, provides for the filling of a vacancy in the Senate by election by the members of the Senate who are affiliated with the same political party as the person last elected to the seat which has become vacant; and WHEREAS, Lou Terhar of the 8th Senatorial District has resigned as a member of the Senate effective September 30, 2019, thus creating a vacancy in the Senate; now therefore be it 1262 SENATE JOURNAL, WEDNESDAY, OCTOBER 9, 2019 RESOLVED, By the members of the Senate who are affiliated with the Republican party, that Louis W. -

Most Lawmakers Running in Local Races Fare Well
November 10, 2016 Most lawmakers running in local races fare well State lawmakers running for local posts nearly ran the table on Tuesday, with just one going down in defeat. The lone loss came in Stark County, where Canton Township Trustee Bill Smith secured an unofficial 57.5-42.5% victory over Rep. Stephen Slesnick (D-Canton) in the race for a seat on the Stark County Board of Commissioners. The House's second highest-ranking Republican, Rep. Ron Amstutz (R-Wooster), secured a seat on the Wayne County Board of Commissioners after defeating David Keifer by a preliminary margin of about 70-30%. Mr. Keifer sought Rep. Amstutz's House seat in the March primary election but was defeated by Scott Wiggam, who went on to win the general election race. In Huron County, Rep. Terry Boose (R-Norwalk) bested Democrat Howard Smith in the race for a seat on the Huron County Board of Commissioners by about a margin of 64-36%, preliminary results show. Democratic lawmaker, Denise Driehaus (D-Cincinnati), is ahead of Hamilton County Commissioner Dennis Deters by a margin of 50.2 - 49.8% in the unofficial results. Term-limited Rep. Bill Hayes (R-Harrison Twp.) defeated his Democratic opponent, attorney Chris Shook, by a margin of 63.6-36.4% for the Licking County prosecutor's office. Sen. Shannon Jones (R-Springboro) was uncontested for a seat on the Warren County Board of Commissioners. 1 Republican majority increases in Ohio Senate Republican Presidential candidate Donald Trump's surprisingly strong win in Ohio was mirrored down ticket in legislative races, as the GOP was able to add to historically large majorities in both the House and Senate. -

November 17-18, 2012 Member's
O OUR E T AU T T U H B O I R R T S N 2 E 1 X 0 T 2 M , E 8 1 E - T 7 I 1 N . G V S O OC N T. 27-28 & Page 1 Page 2 OFFICERS PRESIDENT Cecil Parker KEEP the U.S.A. the American Way FIRST VICE PRESIDENT Motto of OGCA since 1937 Jim Tekavec Overheard at a recent OGCA meeting: an IDEAL: … I know not what course SECOND VICE PRESIDENT “Grandpa, what IS the ‘American Way?” others may take; but as for me, Give Robert Ray Preston me Liberty or Give me Death! Figuring a similar question could come my P. Henry, Virginia Convention SECRETARY way soon, I sat down to articulate an answer. Frank S. Hodges, Jr. But nothing would flow -- all the words seemed an AFFIRMATION: … our Fathers brought TREASURER small and forgettable. So I turned to echoes forth on this Continent a New Nation, con- from our past. ceived in Liberty and dedicated to the proposi- Thomas L. Kyser tion that all men are created equal. First “Branded” almost two and a half centu- A. Lincoln, The Gettysburg Address DIRECTORS ries ago, but enduring since the beginning of 2012-2013-2014 time, The American Way is -- a PROMISE: … Congress shall make no law Frank Becker, Jr. ... prohibiting the free exercise [of Religion]; Thomas E. Bowersox a BELIEF: We hold these truths to be self- or abridging the freedom of speech, or of the Joe Criniti evident, that all men are created equal, that press; or the right of the people peaceably to 2011-2012-2013 they are endowed by their Creator with certain assemble … Terrie L. -

Health Education Standards the Ohio Legislature Is
Support Senate Bill 121: Health Education Standards The Ohio legislature is currently considering Senate Bill 121, which would benefit students in Ohio. Specifically, the bill would allow the Ohio Department of Education to adopt health education standards. Local Matters strongly supports the implementation of health education standards in Ohio, as it lays an important foundation for nutrition education, among other health topics. The bill has bipartisan support and a diverse group of cosponsors. Notably, Senator Peggy Lehner, Chair of the Education Committee, where the bill is currently being heard, is a cosponsor of this important legislation. If you would like to show your support for Senate Bill 121, please contact the elected officials who sit on the Senate Education Committee (see below). If you have any questions about health education standards or the bill, please contact Noreen Warnock, Local Matters Co-founder and Director of Advocacy and Community: [email protected] or 614-263-5662. Key Talking Points: 1) Ohio is the only state in the country without health education standards for K-12 students. 2) Ohio currently faces a public health crisis. Over 33% of children in Ohio have enough excess weight to put them at risk of developing early onset diet-related diseases like diabetes and heart disease.1 3) Senate Bill 121 will help ensure students learn necessary skills to make healthy life choices, such as selecting healthy foods and engaging in physical activity. 4) The cost of healthcare in Ohio required to treat diet-related disease is estimated at $6.36 billion dollars.2 Children’s health complications will only increase economic and workforce burden as the generation ages. -

2018 Post-General Election Update
2018 post-general election update November 7, 2018 On Tuesday, November 6, 2018, Ohioans cast ballots in the 2018 general election. For the first time since 2006, five statewide elected offices were up for election without an incumbent running in the 2018 general election. Federal offices, including all Ohio U.S. Representatives seats and one U.S. Senate seat, two Ohio Supreme Court seats, all seats in the Ohio House of Representatives and 17 Ohio Senate seats were on the ballot. Many counties in Ohio and around the country reported record- breaking early voter turnout. Nearly 1.5 million ballots were requested by mail and in person, and an estimated 1.3 million had been cast as of the close of early voting on November 5, 2018. Here is Bricker & Eckler’s overview of the 2018 general election results and details on races of particular interest. STATEWIDE BALLOT ISSUES Issue 1: This proposed constitutional amendment was filed as the “Neighborhood Safety, Drug Treatment, and Rehabilitation Amendment.” If adopted, the amendment would have, among other things, required reductions in sentencing in certain situations, mandated that certain criminal offenses or uses of any drugs, such as fentanyl and heroin, can only be classified as a misdemeanor, and prohibited jail time as a sentence for obtaining, possessing or using such drugs until an individual’s third offense within 24 months. Issue 1 was defeated by 63.41 percent. The Ohio Safe and Healthy Communities Campaign led the way in support of the proposed constitutional amendment. Supporters of Issue 1 were financially supported by Open Society Policy Center, the Chan Zuckerberg Initiative and the Open Philanthropy Project Action Fund. -

December 12, 2016 131ST GENERAL ASSEMBLY ENDS LAME DUCK
December 12, 2016 131ST GENERAL ASSEMBLY ENDS LAME DUCK SESSION WITH SEVERAL MUNICIPAL ISSUES ADDRESSED The lame duck session ended Friday morning at about 3:30 am and as the dust settled, we’re proud to report that Ohio municipalities were able to claim a number of victories, a few draws, and only a limited number of losses. Now, we immediately turn our agenda to the next General Assembly, with the release of our first broad based policy report tomorrow. We would like to express our gratitude toward the many members of the General Assembly who worked with us on these many issues. Many members worked with us late into the night many times and worked hard to consider our concerns. Below, we review the legislation that effected municipalities in the final days of the session. Each of the following bills has been sent to Governor Kasich for his consideration. First, is Senate Bill 331, introduced by Senator Bob Peterson (R-Washington Court House). The original bill would regulate the sale of dogs from pet stores and dog retailers and to require the Director of Agriculture to license pet stores. This bill was introduced to create a statewide regulatory framework for pet breeding. The OML opposed this portion of the bill as an infringement on Home Rule and “single issue rule” problems which is the part of the Ohio Constitution that prohibits the legislature from passing bills with multiple subjects. This bill became a “Christmas tree bill” where numerous amendments were added, including language from AT&T on the 5G roll out Amendment 1: As mentioned above and as many of our members are aware, the House Finance committee amended the bill to create new regulations concerning micro wireless facility operators for their use of municipally owned land. -
Newsletter Nov. 10Final2.Indd
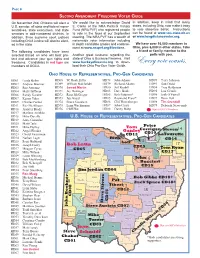
PAGE 8 SECOND AMENDMENT FREEDOMS VOTER GUIDE On November 2nd, Ohioans will elect a We would like to acknowledge David In addition, keep in mind that many U.S. senator, all state and federal repre- E. Conte of the NRA Political Victory states, including Ohio, now make it easy sentatives, state executives, and state Fund (NRA PVF) who registered people to vote absentee ballot. Instructions senators in odd-numbered districts. In to vote in the foyer at our September can be found at www.sos.state.oh.us addition, three supreme court justices meeting. The NRA PVF has a wealth of or www.longdistancevoter.org. including Chief Justice will also be elect- nationwide voter information including ed in the state. in depth candidate grades and endorse- We have over 10,000 members in ment at www.nrapvf.org/Elections. Ohio, plus 6,000 in other states. Take The following candidates have been a friend or family member to the selected based on who will best pro- Another great resource regarding the polls with you. tect and advance your gun rights and state of Ohio is Buckeye Firearms. Visit freedoms. Candidates in red type are www.buckeyefi rearms.org to down- Every vote counts. members of OGCA. load their Ohio Pro-Gun Voter Guide. OHIO HOUSE OF REPRESENTATIVES, PRO-GUN CANDIDATES HD01 Linda Bolon HD68 W. Roak Zeller HD78 John Adams HD89 Terry Johnson HD02 Andrew Brenner HD69 William Batchelder HD79 Richard Adams HD91 Dan Dodd HD03 Ron Amstutz HD70 Jarrod Martin HD80 Jeff Krabill HD94 Troy Balderson HD04 Matt Huffman HD71 Jay Hottinger HD83 Dave Burke HD95 Lou Gentile HD06 Randy Gardner HD72 Ross McGregor HD85 Bob Peterson* HD96 Josh O’Farrell HD07 Kenny Yuko HD73 Jay Goyal HD85 Raymond Pryor* HD97 Dave Hall HD09 Charles Perkel HD74 Bruce Goodwin HD86 Cliff Rosenberger HD98 Tim Grendell HD11 Roz McAllister HD75 Lynn Wachtmann HD87 John Carey HD99 Deborah Newcomb HD16 Jennifer Brady HD76 Cliff Hite HD88 Danny Bubp Depicts OGCA Members HD17 Marlene Anielski HD18 Mike Dovilla U.S. -

Standing Committees 133Rd General Assembly
STANDING COMMITTEES 133RD GENERAL ASSEMBLY AGRICULTURE & NATURAL RESOURCES Senator Frank Hoagland, Chair Senator Brian Hill, Vice Chair Senator Sean O’Brien, Ranking Minority Senator Bob Hackett Senator Teresa Fedor Senator Steve Huffman Senator Tina Maharath Senator Stephanie Kunze Senator Rob McColley Senator Bob Peterson Senator Joe Uecker EDUCATION Senator Peggy Lehner, Chair Senator Lou Terhar, Vice Chair Senator Teresa Fedor, Ranking Minority Senator Andrew Brenner Senator Tina Maharath Senator Bill Coley Senator Vernon Sykes Senator Theresa Gavarone Senator Matt Huffman Senator Steve Huffman Senator Nathan Manning ENERGY & PUBLIC UTILITIES Senator Steve Wilson, Chair Senator Rob McColley, Vice Chair Senator Sandra Williams, Ranking Minority Senator Andrew Brenner Senator Hearcel Craig Senator Dave Burke Senator Sean O’Brien Senator Matt Dolan Senator John Eklund Senator Frank Hoagland Senator Matt Huffman Senator Bob Peterson Senator Michael Rulli 1 FINANCE Senator Matt Dolan, Chair Senator Dave Burke, Vice Chair Senator Vernon Sykes, Ranking Minority Senator John Eklund Senator Nickie Antonio Senator Jay Hottinger Senator Sean O’Brien Senator Stephanie Kunze Senator Peggy Lehner Senator Rob McColley Senator Kirk Schuring Senator Lou Terhar Senator Steve Wilson Finance – General Government & Agency Review Subcommittee Senator Kirk Schuring, Chair Senator Michael Rulli, Vice Chair Senator Kenny Yuko, Ranking Minority Senator John Eklund Senator Hearcel Craig Senator Frank Hoagland Senator Sean O’Brien Senator Brian Hill Senator -

To Download Your Pro Gun Voter Guide
Pro Gun Voter Guide OHIO GENERAL ELECTION VOTE Tuesday, November 6, 2012 www.BuckeyeFirearms.org This list of candidates shows the district, name, party affi liation, and grade of candidates running for offi ce in the general election. See the FREE Pro-Gun Newsletter back of this sheet for an explanation of our grades. The “” indicates a Stay up-to-date on gun laws, politics, and candidate who is offi cially endorsed by Buckeye Firearms Association. events. Plus get the Grassroots Action Guide Create a CUSTOM VOTER GUIDE at BuckeyeFirearms.org. Free! Sign up at BuckeyeFirearms.org. U.S. Senate HD02 Mark Romanchuk (R) C HD29 Louis Blessing III (R) A Ohio Josh Mandel (R) A HD03 Tim Brown (R) B HD29 Hubert Brown (D) ?? HD03 Kelly Wicks (D) ?? HD30 Steven Newson (D) ?? U.S. House HD04 Robert Huenke (D) ?? HD30 Louis Terhar (R) A CD04 Jim Jordan (R) A+ HD04 Matt Huffman (R) A HD31 Denise Driehaus (D) D CD05 Bob Latta (R) A+ HD05 Nick Barborak (D) Aq HD31 Michael Gabbard (R) ?? CD07 Bob Gibbs (R) A+ HD05 Craig Newbold (R) A HD32 Dale Mallory (D) D HD06 Marlene Anielski (R) A HD32 Ron Mosby (R) ?? Justice of the Supreme Court HD06 Anthony Fossaceca (D) ?? HD33 Tom Bryan (R) Aq Ohio Robert Cupp (R) HD07 Mike Dovilla (R) A HD33 Alicia Reece (D) D Ohio Sharon Kennedy (R) HD07 Matt Patten (D) A HD34 Ronya Jeannette Habash (R) ?? Ohio Terrence O’Donnell (R) HD08 Armond Budish (D) D HD34 Vernon Sykes (D) D HD08 Tony Hocevar (R) ?? HD35 Zack Milkovich (D) D Ohio Senate HD09 Barbara Boyd (D) D HD35 Kevin Mitchell (R) Aq SD01 Cliff Hite