Tobacco Control Policy Making: United States
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SUGGESTED 2017-18 LEGISLATIVE INTERIM COMMITTEES with LEGISLATOR PREFERENCES COMMITTEE WORKING DOCUMENT All Choices
June 13, 2017 11:00 a.m. SUGGESTED 2017-18 LEGISLATIVE INTERIM COMMITTEES WITH LEGISLATOR PREFERENCES COMMITTEE WORKING DOCUMENT All Choices Administrative Rules R Representative Greg Westlind 4 (1 From Each House or Senate Standing Committee) R Representative Randy Boehning 1 Budget Section R Representative Bill Devlin 1 Membership consists of leadership R Representative Kim Koppelman 1 R Representative Larry Bellew R Representative Scott Louser 1 R Representative Randy Boehning R Representative Jay Seibel 1 R Representative Roger Brabandt D Senator Joan Heckaman 1 R Representative Mike Brandenburg R Representative Nathan Toman 2 R Representative Al Carlson R Representative Robin Weisz 2 R Representative Jeff Delzer R Representative Brandy Pyle 3 R Representative Tom Kading D Representative Joshua Boschee 3 R Representative Keith Kempenich R Senator Kelly Armstrong 3 R Senator Jerry Klein 3 R Representative Gary Kreidt R Senator Nicole Poolman 4 R Representative Bob Martinson D Representative Mary Schneider R Representative Lisa Meier R Senator Howard Anderson R Representative David Monson R Senator Ralph Kilzer R Representative Mike Nathe R Senator Scott Meyer R Representative Jon Nelson R Senator David Rust R Representative Chet Pollert 18 Members R Representative Mark Sanford 15 Republicans 3 Democrats R Representative Mike Schatz R Representative Ben Koppelman 2 R Representative Jim Schmidt R Representative Karen Rohr 4 R Representative Roscoe Streyle R Representative Gary Sukut 4 R Representative Donald Vigesaa D Representative -

House of Rep Daily Journal
Page 1 1st DAY MONDAY, DECEMBER 3, 2018 1 Organizational and Orientation Session December 3, 4, 5, 2018 JOURNAL OF THE HOUSE Sixty-sixth Legislative Assembly * * * * * Bismarck, December 3, 2018 The House convened at 1:00 p.m., with Speaker Bellew presiding. The prayer was offered by Rev. Rich Wyatt, Living Hope Church of the Nazarene, Bismarck. COMMUNICATION FROM SECRETARY OF STATE ALVIN A. JAEGER December 3, 2018 In accordance with Section 54-03-03 of the North Dakota Century Code, I certify the enclosed list is a true and correct record of members of the House of Representatives elected in the General Election held on November 6, 2018. The State Canvassing Board certified the results of the election on November 16, 2018. As specified in Section 16.1-15-45 of the North Dakota Century Code, Certificates of Election were then prepared by the Secretary of State and signed by the Governor, the Clerk of the Supreme Court (as the designated representative of the State Canvassing Board), and the Secretary of State. Each newly elected member of the Legislative Assembly was then issued their Certificate of Election (copies enclosed), as specified in Section 16.1-15-46 of the North Dakota Century Code. In addition, in accordance with Section 4, Article XI, of the North Dakota Constitution, an Oath of Office (or affirmation) form was provided to each Representative, with instructions to execute the Oath before a Notary Public and file it with the Secretary of State before he or she assumes the duties of their office. IN TESTIMONY WHEREOF, I have set my hand and affixed the Great Seal of the State of North Dakota at the Capitol in the City of Bismarck on this date. -
The Ranch Hand
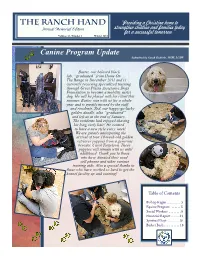
The Ranch Hand “Providing a Christian home to Annual Memorial Edition strengthen children and families today for a successful tomorrow.” Volume 31, Number 1 Winter 2012 Canine Program Update Submitted by Sarah Gubbels, MSW, LCSW Buster, our beloved black lab, “graduated” from Home On The Range in December 2011 and is currently receiving specialized training through Great Plains Assistance Dogs Foundation to become a mobility assist dog. He will be placed with his client this summer. Buster was with us for a whole year and is greatly missed by the staff and residents. Zed, our happy-go-lucky golden doodle, also “graduated” and left us at the end of January. The residents had enjoyed shaving his long curly hair! He seemed to have a new style every week! We are greatly anticipating the arrival of four 10-week-old golden retriever puppies from a generous breeder, Carol Torgelson. These puppies will remain with us until adulthood. Thank you to those who have donated their used cell phones and other various training aids. Also a special thanks to those who have worked so hard to get the kennel facility up and running! Table of Contents Bishop Kagan . 5 Equine Program . 5 Social Workers . 8 Financial Report . .14 Spiritual Dept . 16 Basket Bash . 18 Commemorative Gifts Contributions to Home On The Range (HOTR) in honor or in memory of an individual help ensure that the facility can continue to provide the very best care possible. We notify the honoree, or next of kin, regarding the gift with an appropriate card, as well as sending the donor a receipt or card. -

Budget Section
15.5082.03000 NORTH DAKOTA LEGISLATIVE MANAGEMENT Minutes of the BUDGET SECTION Wednesday, March 12, 2014 Senate Chamber, State Capitol Bismarck, North Dakota Representative Chet Pollert, Chairman, called the meeting to order at 10:00 a.m. Members present: Representatives Chet Pollert, Larry Bellew, Tracy Boe, Mike D. Brandenburg, Al Carlson, Jeff Delzer, Bill Devlin, Mark A. Dosch, Bette Grande, Ron Guggisberg, Rick Holman, Keith Kempenich, Gary Kreidt, Bob Martinson, Corey Mock, David Monson, Jon Nelson, Kenton Onstad, Blair Thoreson, Don Vigesaa, Alon Wieland; Senators Bill L. Bowman, Ron Carlisle, Robert Erbele, Joan Heckaman, Ray Holmberg, Ralph Kilzer, Jerry Klein, Karen K. Krebsbach, Gary A. Lee, Tim Mathern, David O'Connell, Larry J. Robinson, Mac Schneider, Terry M. Wanzek, Rich Wardner, John M. Warner Members absent: Representatives Eliot Glassheim, Kathy Hawken, Mark Sanford, Bob J. Skarphol, Roscoe Streyle, Clark Williams; Senator Tony Grindberg Others present: Donald Schaible, State Senator, Mott Representative Jim Schmidt, member of the Legislative Management, was also in attendance. See Appendix A for additional persons present. It was moved by Senator Robinson, seconded by Senator O'Connell, and carried on a voice vote that the minutes of the December 11, 2013, meeting be approved as distributed. STATUS OF THE GENERAL FUND Ms. Pam Sharp, Director, Office of Management and Budget, presented a report (Appendix B) on the status of the general fund. Ms. Sharp presented the following information on the status of the general -

2021 State Legislator Pledge Signers
I pledge that, as a member of the state legislature, I will cosponsor, vote for, and defend the resolution applying for an Article V convention for the sole purpose of enacting term limits on Congress. The U.S. Term Limits Article V Pledge Signers 2021 State Legislators 1250 Connecticut Ave NW Suite 200 ALABAMA S022 David Livingston H073 Karen Mathiak Washington, D.C. 20036 Successfully passed a term S028 Kate Brophy McGee H097 Bonnie Rich (202) 261-3532 limits only resolution. H098 David Clark termlimits.org CALIFORNIA H103 Timothy Barr ALASKA H048 Blanca Rubio H104 Chuck Efstration H030 Ron Gillham H105 Donna McLeod COLORADO H110 Clint Crowe ARKANSAS H016 Andres Pico H119 Marcus Wiedower H024 Bruce Cozart H022 Margo Herzl H131 Beth Camp H042 Mark Perry H039 Mark Baisley H141 Dale Washburn H071 Joe Cloud H048 Tonya Van Beber H147 Heath Clark H049 Michael Lynch H151 Gerald Greene ARIZONA H060 Ron Hanks H157 Bill Werkheiser H001 Noel Campbell H062 Donald Valdez H161 Bill Hitchens H001 Judy Burges H063 Dan Woog H162 Carl Gilliard H001 Quang Nguyen H064 Richard Holtorf H164 Ron Stephens H002 Andrea Dalessandro S001 Jerry Sonnenberg H166 Jesse Petrea H002 Daniel Hernandez S010 Larry Liston H176 James Burchett H003 Alma Hernandez S023 Barbara Kirkmeyer H177 Dexter Sharper H005 Leo Biasiucci H179 Don Hogan H006 Walter Blackman CONNECTICUT S008 Russ Goodman H007 Arlando Teller H132 Brian Farnen S013 Carden Summers H008 David Cook H149 Kimberly Fiorello S017 Brian Strickland H011 Mark Finchem S021 Brandon Beach H012 Travis Grantham FLORIDA S027 Greg Dolezal H014 Gail Griffin Successfully passed a term S030 Mike Dugan H015 Steve Kaiser limits only resolution. -

Lr101601 Minutes
NORTH DAKOTA LEGISLATIVE COUNCIL Minutes of the LEGISLATIVE REDISTRICTING COMMITTEE Tuesday and Wednesday, October 16-17, 2001 Harvest Room, State Capitol Bismarck, North Dakota Representative Mike Timm, Chairman, called the with which the committee will begin to further modify a meeting to order at 9:00 a.m. plan. Members present: Representatives Mike Timm, In response to a question from Senator Mathern, Ole Aarsvold, Al Carlson, William R. Devlin, Glen Chairman Timm said the vote is not to approve a Froseth, Pam Gulleson, Lyle Hanson, David Monson; particular plan but to select a plan with which the Senators Bill Bowman, Randel Christmann, Layton committee can make modifications. Freborg, Ray Holmberg, Ed Kringstad, Tim Mathern, It was moved by Senator Tomac, seconded by Steven W. Tomac Representative Gulleson, and failed on a roll call Others present: Bob Stenehjem, State Senator, vote that Senator Tomac’s 45-district plan be Bismarck approved for further consideration by the commit- Wesley R. Belter, State Representative, Leonard tee. Representative Gulleson and Senators Mathern Lois Delmore, State Representative, Grand Forks and Tomac voted “aye.” Representatives Timm, Jay Johnson, Minot Daily News, Minot Aarsvold, Carlson, Devlin, Froseth, Hanson, and Harlan Fuglesten, North Dakota Association of Monson and Senators Bowman, Christmann, Freborg, Rural Electric Cooperatives, Fargo and Mandan Holmberg, and Kringstad voted “nay.” Jon Lindgren, American Civil Liberties Union, It was moved by Representative Carlson, Fargo seconded by Senator Holmberg, and carried on a Tim Flakoll, State Senator, Fargo roll call vote that Representative Devlin’s Tom Disselhorst, Three Affiliated Tribes, Bismarck 47-district plan be approved for further considera- Carol Two Eagle, Grassroots American Indians, tion by the committee. -

MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2016 Name State Candidate Amount U.S
MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2016 Name State Candidate Amount U.S. House Robert Aderholt for Congress AL Rep. Robert Aderholt $2,000 ALABAMA TOTAL U.S. House Crawford for Congress AR Rep. Rick Crawford $1,500 Womack for Cogress Committee AR Rep. Stephen Womack $500 ARKANSAS TOTAL U.S. House Kyrsten Sinema for Congress AZ Rep. Kyrtsen Sinema $500 ARIZONA TOTAL U.S. House Denham for Congress CA Rep. Jeff Denham $1,500 Garamendi for Congress CA Rep. John Garamendi $500 Kevin McCarthy for Congress CA Rep. Kevin McCarthy $1,000 Valadao for Congress CA Rep. David Valadao $1,500 U.S. House Leadership Majority Committee PAC--Mc PAC CA Rep. Kevin McCarthy $5,000 State Assembly Adam Gray for Assembly 2016 CA Assm. Adam Gray $1,500 Catharine Baker for Assembly 2016 CA Assm. Catharine Baker $2,500 Cecilia Aguiar-Curry for Assembly 2016 CA Assm. Cecilia Aguiar-Curry $2,000 Chad Mayes for Assembly 2016 CA Assm. Chad Mayes $2,000 James Gallagher for Assembly 2016 CA Assm. James Gallagher $1,500 Patterson for Assembly 2016 CA Assm. James Patterson $2,000 Jay Obernolte for Assembly 2016 CA Assm. Jay Obernolte $1,500 Jim Cooper for Assembly 2016 CA Assm. Jim Cooper $1,500 Jimmy Gomez for Assembly 2016 CA Assm. Jimmy Gomez $1,500 Dr. Joaquin Arambola for Assembly 2016 CA Assm. Joaquin Arambula $1,500 Ken Cooley for Assembly 2016 CA Assm. Ken Cooley $1,500 Miguel Santiago for Assembly 2016 CA Assm. Miguel Santiago $1,500 Rudy Salas for Assembly 2016 CA Assm. -

Learn Which Candidates We Supported in Your Community PFIZER PAC ~ OUR VOICE in the POLITICAL PROCESS a Message from Rich Bagger, Chairman Pfizer PAC
PFIZER PAC & CORPORATE POLITICAL CONTRIBUTIONS REPORT 2005 – 2006 CYCLE Learn which candidates we supported in your community PFIZER PAC ~ OUR VOICE IN THE POLITICAL PROCESS A Message From Rich Bagger, Chairman Pfizer PAC Dear Colleagues: One of our five immediate priorities at Pfizer is to engage more actively and meaningfully with patients, doctors, payers, governments and other key stakeholders. We’re reaching out to these important groups and working harder to meet their needs. We're also working harder to engage all stakeholders in the dialogue on health policy and actively participate in the discussion over how to improve the quality of healthcare, access to medicines, and incentives for innovation. Pfizer PAC is one of the key ways in which we engage with candidates for public office. Through Pfizer PAC, we support candidates who understand the importance of innovative life sciences companies like Pfizer in fighting disease, improving health outcomes, and ensuring access to vital medicines. This report includes a list of candidates and political committees that Pfizer PAC supported during the 2005-06 election cycle. I hope you will take some time to review this report and see which candidates Pfizer PAC supported in your region. This was a successful year for Pfizer PAC. In the past election cycle, Pfizer PAC supported more than 2,277 candidates from both political parties, and at all levels of government. You, and Pfizer colleagues across America, definitely made a difference this past year through Pfizer PAC, by supporting candidates for public office who value access and innovation in healthcare. Thank you for your support—this report explains how Pfizer PAC put your generous contributions to use. -

Revised Meeting Notice
15.5171.01000 September 2, 2014 REVISED MEETING NOTICE Representative Chet Pollert, Chairman, has called a meeting of the BUDGET SECTION. Date: Wednesday, September 24, 2014 Time: 9:30 a.m. Place: Senate Chamber, State Capitol, Bismarck Agenda: Presentations by representatives of the Office of Management and Budget regarding the status of the general fund, revised 2013-15 biennium and preliminary 2015-17 biennium revenue forecasts, key economic indicators, irregularities in the fiscal practices of the state, employees receiving bonuses above the 25 percent limitation, tobacco settlement proceeds, and federal grant applications; by state agency representatives regarding Emergency Commission requests; by representatives of the Game and Fish Department on approval of land purchases; by representatives of the Department of Corrections and Rehabilitation on prison population, inmate admissions, and the number of inmates not admitted; by representatives of the Department of Human Services regarding transfers between line items or subdivisions; by representatives of the State Fire Marshal on income and expenditures of fire departments and reserve fund balances; by representatives of the Information Technology Department regarding the department's annual report; by the Legislative Council staff of the 2014 North Dakota Finance Facts, on the status of the state's federal funds receipts on block grant hearings required during the 2015 legislative session, and a resolution draft authorizing the Budget Section to hold any required legislative block -

Agenda BUDGET SECTION Wednesday, June 21, 2017 Senate Chamber, State Capitol Bismarck, North Dakota
19.5013.02000 Revised 6/20/2017 NORTH DAKOTA LEGISLATIVE MANAGEMENT Tentative Agenda BUDGET SECTION Wednesday, June 21, 2017 Senate Chamber, State Capitol Bismarck, North Dakota 1:00 p.m. Call to order Roll call 1:05 p.m. Presentation by Legislative Council staff of the following: • Supplementary Rules of Operation and Procedure of the North Dakota Legislative Management • Final budget status report on appropriations and estimated revenues - 2017-19 biennium • 65th Legislative Assembly Changes to Agency Budgets - 2017-19 Biennium • 65th Legislative Assembly State Budget Actions for the 2017-19 Biennium • Estimated Revenue Sources and Distributions for Major State Funds for the 2017-19 Biennium • Duties and Responsibilities of the Budget Section for the 2017-18 Interim • Oil and Gas Tax Revenue Allocation Flowchart 1:20 p.m. Presentations by representatives of the Office of Management and Budget regarding: • Status of the general fund • Report on any tobacco settlement proceeds • Reports from state agencies applying for federal grants estimated to be $25,000 or more pursuant to North Dakota Century Code Section 54-27-27 • Irregularities in the fiscal practices of the state pursuant to Section 54-14-03.1 • Status of the voluntary separation incentive program 1:45 p.m. Committee consideration of a state agency request pursuant to Chapter 54-16 that has * been authorized by the Emergency Commission and requires consideration by the Budget Section • Adjutant General (Request #1897) - Request is to authorize the expenditure of up to $8,523,161 from the state disaster relief fund as appropriated by the 2017 Legislative Assembly for paying the state share of expenses relating to previous state disasters in accordance with Section 37-17.1-27 during the 2017-19 biennium 2:00 p.m. -

Ieps and SECTION 504 - WHAT's the DIFFERENCE?
February 2017 - In This Issue: IEPs AND SECTION 504 - WHAT'S THE DIFFERENCE? SUPPORT PATHFINDER FUNDING US DEPARTMENT ED NEWS TRAINING OPPORTUNITIES NEWS FROM NDDPI RAISING PRE-SCHOOLERS RAISING ELEMENTARY STUDENTS LIFE WITH TEENS RESOURCES SPOTLIGHT AGENCY/ORGANIZATION SPOTLIGHT IEPs and Section 504 - What's the Difference? To be eligible for individualized assistance under Section 504, a student The staff at Pathfinder is frequently asked must have a disability that "substantially limits" one or more "major life to explain the differences between an IEP activities" (very broadly defined). The major difference between a 504 (Individualized Education Program) and a plan and an IEP is that, for a 504 plan, the student does NOT need Section 504 accommodation plan. We specialized instruction to make effective progress. Instead, the student agree that it can be confusing, so here is a may need only accommodations (such as additional time, special short primer on some key points: seating, or sensory breaks) and/or related services (such as a reading program, speech and language services, or occupational therapy) in Legal Framework order to access the general curriculum. It is important to note a child who is on an IEP is automatically protected under Section 504. In most An Individualized Education Program (IEP) is a written statement of cases, there is no need for two plans, as any needed accommodations a student's educational program designed to meet a child's and related services are typically included in the IEP. individual needs. Every child who receives special education services must have an IEP. The Individuals with Disabilities Placement Education Act of 2004 (IDEA) at the federal level outline the process for how to develop an IEP. -

Tobacco Control Policy Making in North Dakota: a Tradition of Activism
Tobacco Control Policy Making in North Dakota: A Tradition of Activism Jennifer R. Welle MPH Jennifer K. Ibrahim Ph.D. Stanton A. Glantz Ph.D. Center for Tobacco Control Research and Education Institute for Health Policy Studies School of Medicine University of California, San Francisco San Francisco CA 94118 June 2004 Tobacco Control Policy Making in North Dakota: A Tradition of Activism Jennifer R. Welle MPH Jennifer K. Ibrahim Ph.D. Stanton A. Glantz Ph.D. Center for Tobacco Control Research and Education Institute for Health Policy Studies School of Medicine University of California, San Francisco San Francisco CA 94118 June 2004 Supported in part by National Cancer Institute Grant CA-61021. Copyright 2004 by J.R. Welle, J.K. Ibrahim and S.A. Glantz. Permission is granted to reproduce this report for nonprofit purposes designed to promote the public health, so long as this report is credited. This report is available on the World Wide Web at http://repositories.cdlib.org/ctcre/tpmus/ND2004 .This report is one of a series of reports that analyze tobacco industry campaign contributions, lobbying, and other political activity throughout the United States and elsewhere. The other reports are available on the World Wide Web at http://repositories.cdlib.org/ctcre/. 1 2 EXECUTIVE SUMMARY North Dakota has a long history of tobacco-related legislation dating back to the late 1800's, well before the formal organization of health advocates for tobacco control. Citizens of North Dakota recognized the negative health effects of tobacco smoke before most of the nation and made attempts to regulate the sale and use of tobacco products throughout the early 1900's.