Risk Perception and Coping Behavior of Construction Workers on Occupational Health Risks—A Case Study of Nanjing, China
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Structural Components, Lifting Mechanism, Crane Control Project Has Been Established with a View to Remove the Need to Have Workers in High Places
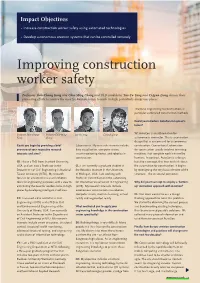
Impact Objectives • Increase construction worker safety using automated technologies • Develop autonomous erection systems that can be controlled remotely Improving construction worker safety Professors Shih-Chung Kang and Chia-Ming Chang and PhD candidates Yao-Yu Yang and Ci-Jyun Liang discuss their pioneering efforts to remove the need for human beings to work in high, potentially dangerous places structural engineering to construction, in particular automated construction methods. Could you introduce AutoCon in layman’s terms? Professor Shih-Chung Professor Chia-Ming Yao-Yu Yang Ci-Jyun Liang YY: AutoCon is an abbreviation for Kang Chang autonomous connector. This is a connector design that is customised for autonomous Could you begin by providing a brief Laboratories. My research interests include construction. Conventional automation overview of your respective research data visualisation, computer vision, for construction usually involves inventing interests and aims? smart monitoring device, and robotics in machines that complete work initiated by construction. humans. In contrast, AutoCon is a design, SK: I have a PhD from Stanford University, but also a concept, that tries to think about USA, and am now a Professor in the CL: I am currently a graduate student at the automation for construction. It begins Department of Civil Engineering in National the Robotics Institute in the University by redesigning the very basic element of the Taiwan University (NTU). My research of Michigan, USA. I am working with structure – the structural connector. focuses on advanced visual and robotics Professor Vineet Kamat in the Laboratory tools for engineering purposes, with a view to for Interactive Visualisation in Engineering Why did your team opt to employ a ‘bottom- eliminating the need for workers to be in high (LIVE). -

Identifying Determinants of Construction Worker Performance on Construction Sites: a Literature Review
International Journal of Innovation, Management and Technology, Vol. 8, No. 1, February 2017 Identifying Determinants of Construction Worker Performance on Construction Sites: A Literature Review Chioma S. Okoro, Innocent Musonda, and Justus Agumba executing the processes and activities in construction, they Abstract—The construction industry in many developed and have a significant influence on labour productivity and it is developing countries suffers from delays and cost overruns due important to know what they need and what affects their to poor labour productivity. This paper aims to identify performance [9]. Continuous attention to the determinants determinants of construction workers’ performance on of construction workers’ performance is vital if maximal construction sites in terms of ratio of output to input (productivity). A literature review of relevant literature was productivity in the industry is desired. conducted from journals and conference proceedings and Research has been conducted on the determinants of theses, based on international and South African context. The labour productivity. Ref. [10] used a Health and Labour study identified that wages/salary, working time, financial Questionnaire and a Quantity and Quality instrument to initiatives, communication, nutrition, fatigue and health, measure the effect of health status of workers (including adequacy of plans and specifications, availability of industrial and construction workers). Reference [11] consumables, education and training on the job, management dynamics, safety measures and proper work planning explored project managers’ perceptions (in Uganda) on the determine construction workers’ performance on construction labour productivity factors in relation to time, cost and sites. The findings of the present study could help constitution quality only. Ref. -

Employment in the Construction Industry in the Past 30 Years
TMCIT/2001 INTERNATIONAL LABOUR ORGANIZATION The construction industry in the twenty- first century: Its image, employment prospects and skill requirements Tripartite Meeting on the Construction Industry in the Twenty-first Century: Its Image, Employment Prospects and Skill Requirements Geneva, 2001 INTERNATIONAL LABOUR OFFICE GENEVA Contents Introduction........................................................................................................................................ 1 The context ................................................................................................................................ 1 Background to the Meeting........................................................................................................ 2 Outline of the report................................................................................................................... 3 1. Construction output and employment: The global picture......................................................... 5 1.1. Output and employment at the end of the twentieth century........................................... 5 1.2. Global trends in output and employment......................................................................... 8 1.3. The role of construction employment and characteristics of the workforce.................... 11 1.4. Construction in the eyes of the workforce....................................................................... 13 2. Recent changes in employment relationships and industrial structure ..................................... -

Construction Workers' Health and Safety During Post Disaster Reconstruction Phase: a Case Study in Nepal
Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 3-29-2019 Construction Workers' Health and Safety During Post Disaster Reconstruction Phase: A Case Study in Nepal S M Jamil Uddin Florida International University, [email protected] Follow this and additional works at: https://digitalcommons.fiu.edu/etd Part of the Construction Engineering and Management Commons Recommended Citation Uddin, S M Jamil, "Construction Workers' Health and Safety During Post Disaster Reconstruction Phase: A Case Study in Nepal" (2019). FIU Electronic Theses and Dissertations. 4011. https://digitalcommons.fiu.edu/etd/4011 This work is brought to you for free and open access by the University Graduate School at FIU Digital Commons. It has been accepted for inclusion in FIU Electronic Theses and Dissertations by an authorized administrator of FIU Digital Commons. For more information, please contact [email protected]. FLORIDA INTERNATI ONAL UNIVERSITY Miami, Florida CONSTRUCTION WORKERS’ HEALTH A ND SAFETY DURING POST DISASTER RECONSTRUCTION PHASE: A CASE STUDY IN NEPAL A thesis submitted in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE in CONSTRUCTION M ANAGEMENT by S M Jamil Uddin 2019 To: Dean John L. Volakis College of Engineering and Computing This thesis, written by S M Jamil Uddin, and entitled Construction Workers’ Health and Safety during Post Disaster Reconstruction Phase: A Case Study in Nepal, having been approved in respect to style and intellectual content, is referred to you for judgment. We have read this thesis and recommend that it be approved. _______________________________________ N. Emel Ganapati _______________________________________ Jose A. -

2020 Construction Apprenticeship Guidebook 1 2020 Construction Apprenticeship Guidebook
King County • Pierce County • Snohomish County 2020 Construction Apprenticeship Guidebook 1 2020 Construction Apprenticeship Guidebook View online at www.bitly.com/apprenticeshipguidebook. Produced and compiled by In partnership with www.seattle.gov/priorityhire www.soundtransit.org And with help from www.wabuildingtrades.org www.wsdot.wa.gov www.portseattle.org www.kingcounty.gov/priorityhire www.kingcounty.gov/depts/transportation/metro www.tukwilawa.gov On the cover: Terrance is a laborer apprentice and graduate of the PACT pre-apprenticeship program. Prior to working in construction, Terrance was homeless and struggled to find work. He found out about PACT from friends. Once he signed up, PACT helped him get his life back. He got his driver’s license and earned his high school diploma. Terrance now makes over $31 an hour plus benefits working for Jansen Inc., has an apartment and provides for his family; they no longer rely on welfare or food banks. Terrance’s advice to others is to go for it – you have nothing to lose! Learn more about other pathways into construction on Apprentices in Action (page 3). Updated February 2020 2 Table of Contents Introduction 1 Union Apprenticeship cont. Construction Worker Pathway 2 Drywall Finishers 28 Apprentices in Action 3 Electricians (King) 29 Apprenticeship vs. College 4 Electricians (Pierce) 30 Support Services 5 Electricians (Snohomish) 31 RPAC 7 Elevator Constructors 32 Floor Layers 33 Pre-Apprenticeship 8 Glaziers 34 ANEW 9 Heat & Frost Insulators 35 Carpenters 10 Ironworkers 36 Cement Masons -

Migrant Work & Employment in the Construction Sector
Migrant Work & Employment in the Construction Sector Michelle BUCKLEY, Adam ZENDEL, Jeff BIGGAR Lia FREDERIKSEN and Jill WELLS MIGRANT WORK & EMPLOYMENT IN THE CONSTRUCTION SECTOR Labour Migration Branch ILO Migrant Work & Employment in the Construction Sector Migrant Work & Employment in the Construction Sector by Michelle Buckley, Adam Zendel, Jeff Biggar, Lia Frederiksen and Jill Wells International Labour Organization – Geneva Copyright © International Labour Organization 2016 First edition 2016 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Con- vention. Nevertheless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Licensing), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: [email protected]. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with a reproduction rights organization may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. Buckley, Michelle; Zendel, Adam; Biggar, Jeff; Frederiksen, Lia; Wells, Jill. Migrant work and employment in the construction sector / Michelle Buckley, Adam Zendel, Jeff Biggar, Lia Frederiksen and Jill Wells ; International Labour Office, Sectoral Policies Department, Conditions of Work and -

BCC JOBS BOARD February 10, 2021
BCC JOBS BOARD February 10, 2021 Firms posting their open opportunities with the Builders of Color Coalition actively welcome diverse applicants, and look forward to hearing from you. Please let firms know that you heard of the position via BCC. Project Accountant HYM Investment Group Assist the Accounting Manager in facilitating transactional accounting in QuickBooks and Yardi systems, and in the creation of financial packages. Assistant Project Manager - Construction HYM Investment Group Assist in managing and coordinating all construction operations throughout a major commercial interiors construction project. Structural Engineer Nitsch Engineering Support our fast-growing structural engineering department. Chief Engineer Lincoln Property Company Supervise 3 to 4 maintenance personnel and MEP outside contractors. Real Estate Development Manager Juno Residential Oversee the execution of Juno’s multifamily projects on time and on budget – in some cases leading the entitlements, planning, and permitting process. Designer / Architect Studio G Architects Creative and experienced Designer or Architect with 5-8 years’ experience. Project Architect / Project Manager Studio G Architects Design and management of a mix of project types including educational, housing, and institutional. Valuations Asset Management Analyst TA Realty This role focuses on the technical build out and maintenance of analytic tools. To apply, submit a resume to [email protected]. Project Architect CBT We are seeking a skilled Project Architect to come join our team here at CBT! Proposal Manager Dimeo Construction Company Join our marketing team to help execute and lead the firm’s new pursuit qualifications and proposal development fulfillment process. HVAC Service Technician Cummings Properties Full-time HVAC service technician to include service and installation work on water source heat pumps, cooling towers, RTU’s with gas/dx cooling, make up air units, exhausts, control wiring and more. -

HEALTH and SOCIAL EQUITY in REAL ESTATE Examples from the Field HEALTH and SOCIAL EQUITY in REAL ESTATE Examples from the Field ABOUT the URBAN LAND INSTITUTE
HEALTH AND SOCIAL EQUITY IN REAL ESTATE Examples from the Field HEALTH AND SOCIAL EQUITY IN REAL ESTATE Examples from the Field ABOUT THE URBAN LAND INSTITUTE The Urban Land Institute is a global, member-driven organization comprising more than 45,000 real estate and urban development professionals dedicated to advancing the Institute’s mission of providing leadership in the responsible use of land and in creating and sustaining thriving communities worldwide. ULI’s interdisciplinary membership represents all aspects of the industry, including developers, property owners, investors, architects, urban planners, public officials, real estate brokers, appraisers, attorneys, engineers, financiers, and academics. Established in 1936, the Institute has a presence in the Americas, Europe, and Asia Pacific regions, with members in 80 countries. The extraordinary impact that ULI makes on land use decision-making is based on its members sharing expertise on a variety of factors affecting the built environment, including urbanization, demographic and population changes, new economic drivers, technology advancements, and environmental concerns. Peer-to-peer learning is achieved through the knowledge shared by members at thousands of convenings each year that reinforce ULI’s position as a global authority on land use and real estate. In 2019 alone, more than 2,400 events were held in about 330 cities around the world. Drawing on the work of its members, the Institute recognizes and shares best practices in urban design and development for the benefit of communities around the globe. More information is available at uli.org. Follow ULI on Twitter, Facebook, LinkedIn, and Instagram. About the ULI Greenprint Center for Building Performance The ULI Greenprint Center for Building Performance is a worldwide alliance of leading real estate owners, investors, and strategic partners committed to improving the environmental performance of the global real estate industry. -

Somerset Ave. Project Plan 2021
Construction Management Plan DRAFT 10/20/2020 Table of Contents 1. Public Safety…………………………..………………….…………………………………………2 1.1. Police Details 1.2. Perimeter Protection 1.3. Emergency Site Access 1.4. Snow Removal 1.5. Street Cleaning 2. Abutter and Municipal Coordination…………………………………………………………….3 2.1. Abutter Coordination 2.2. Impact on Existing Construction Projects 2.3. Signage 2.4. Utility Connections 3. Construction Logistics………………………………………………………………..…...………4 3.1. Deliveries 3.2. Material Handling 3.3. Construction Waste 3.4. Construction Hours 3.5. Construction Worker Parking 3.6. Portable Sanitary Facilities 3.7. Wash Stations 4. Mitigation Measures…………………………………………………………………………..……6 4.1. Environmental 4.2. Air Quality and Dust Control 4.3. On-site Dewatering 4.4. Pest Control 4.5. Noise Control 4.6. Vibration Monitoring 4.7. Preconstruction Surveys 5. Exhibits…………………………………………………………………………………….………....7 5.1. Exhibit A – Logistics Plan 5.2. Exhibit B – Loading Lane and Sidewalk Detail 5.3. Exhibit C – Site Signage 5.4. Exhibit D – Dust Control Plan 5.5. Exhibit C – Fall Rescue Plan Public Safety Police Details Police details will be provided during construction activities as required to facilitate traffic flow and pedestrian safety. Perimeter Protection This project is zero lot line on all sides. We anticipate installing concrete jersey barriers with fence and scrim along Somerset Avenue and temporary fence panels with scrim along Cottage Park Road. Lot lines abutting neighbors will be protected with temporary fence panels as needed. Emergency Site Access Access to the site for emergency vehicles will be maintained at all times and will follow the site specific NFPA 241 plan. The site will be available for inspection by the fire and police departments upon completion of the perimeter fencing installation. -
A Safety Elements Model for the Building Construction Industry Cliff Dunlap Dunlap Louisiana State University and Agricultural and Mechanical College, [email protected]
Louisiana State University LSU Digital Commons LSU Doctoral Dissertations Graduate School 2012 A safety elements model for the building construction industry Cliff Dunlap Dunlap Louisiana State University and Agricultural and Mechanical College, [email protected] Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_dissertations Part of the Engineering Science and Materials Commons Recommended Citation Dunlap, Cliff Dunlap, "A safety elements model for the building construction industry" (2012). LSU Doctoral Dissertations. 2005. https://digitalcommons.lsu.edu/gradschool_dissertations/2005 This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Doctoral Dissertations by an authorized graduate school editor of LSU Digital Commons. For more information, please [email protected]. A SAFETY ELEMENTS MODEL FOR THE BUILDING CONSTRUCTION INDUSTRY A Dissertation Submitted to the Graduate Faculty of the Louisiana State University and Agricultural and Mechanical College in partial fulfillment of the requirements for the degree of Doctor of Philosophy in The Department of Engineering Science by Cliff Dunlap B.A., Ambassador University, 1966 December 2012 ACKNOWLEDGMENTS I would like to extend my special thanks to my Committee Chair, Dr. Isabelina Nahmens and the other members of the committee in alphabetical order, Dr. Eurico D’Sa (Graduate School Dean Representative), Dr. Craig Harvey, Dr. Sherif Ishak, Dr. Joe Kotrlik and Dr. Jared Llorens for their time effort and patience on my Dissertation. I would also like to extend my special thanks to the members of the special Louisiana State University Safety Council (LSUSC), Dr. Laura Ikuma and Mr. -

The Influence of Social Capitalism on Construction Safety Behaviors: an Exploratory Megaproject Case Study
CORE Metadata, citation and similar papers at core.ac.uk Provided by espace@Curtin sustainability Article The Influence of Social Capitalism on Construction Safety Behaviors: An Exploratory Megaproject Case Study Xiuyu Wu 1, Heap-Yih Chong 2, Ge Wang 3,* ID and Shuquan Li 1 1 School of Management Science and Engineering, Tianjin University of Finance & Economics, Tianjin 300222, China; [email protected] (X.W); [email protected] (S.L) 2 School of Design and the Built Environment, Curtin University, Perth WA 6845, Australia; [email protected] 3 College of Public Administration, Huazhong Agricultural University, Wuhan 430070, China * Correspondence: [email protected]; Tel.: +86-027-8728-4349 Received: 30 July 2018; Accepted: 28 August 2018; Published: 30 August 2018 Abstract: Health and safety issues are critical factors influencing the sustainable development of mega construction projects. The impact of social capitalism on health and safety activities has been widely discussed in sustainability domains; nevertheless, its influence towards workers’ safety behaviors in mega construction projects remains largely unknown. To address this research gap, the current study aims to determine the influence of social capitalism on safety behaviors from a two-fold perspective between project managers and construction workers. An exploratory case study was adopted from a mega construction project in Tianjin, China. The results reveal that (a) the social network between project managers and construction workers manifests itself as close communication and contact, trust and emotional identification, common language, vision, and values; (b) project managers’ management behaviors show stronger influences on construction workers’ safety compliance behaviors, while their leadership behaviors show stronger influences on construction workers’ safety participation behaviors; and (c) the practice of social capitalism promotes enforcement of commands and compulsory norms and plays a positive regulatory role on safety behaviors. -
An Analysis of Construction Accidents from a Design Perspective
An Analysis of Construction Accidents from a Design Perspective Michael Behm, PhD, CSP Department of Technology Systems East Carolina University Greenville, North Carolina January 2006 The Center to Protect Workers’ Rights Suite 1000 ● 8484 Georgia Ave. ● Silver Spring, MD 20910 301-578-8500 ● Fax: 301-578-8572 ● www.cpwr.com ● www.elcosh.org © 2006, The Center to Protect Workers' Rights. All rights reserved. This research was made possible by the Center to Protect Workers' Rights (CPWR) as part of a cooperative agreement with the National Institute for Occupational Safety and Health, NIOSH (NIOSH grant CCU317202). The research is solely the responsibility of the authors and does not necessarily represent the official views of NIOSH. CPWR—a research, development, and training arm of the Building and Construction Trades Department, AFL-CIO—is uniquely situated to serve workers, contractors, and the scientific community. A major CPWR activity is to improve safety and health in the U.S. construction industry. CPWR, Suite 1000, 8484 Georgia Ave., Silver Spring, MD 20910, 301-578-8500, www.cpwr.com. Acknowledgements The author wishes to thank Dr. Anthony Veltri and Dr. John Gambatese of Oregon State University. This research study would not have been possible without their support. Abbreviations/Terms Constructor Includes construction firms, contractors, and subcontractors responsible for building a project and employing construction workers Design professional Includes architects, designers, and design engineers responsible for a project’s design Designing for safety The consideration of construction site safety in the preparation of plans and specifications for construction projects Disabling injury An injury that leaves a worker temporarily or permanently disabled FACE NIOSH Fatality Assessment and Control Evaluation program NIOSH National Institute for Occupational Safety and Health OSHA U.S.