325024-Eng.Pdf (1.099Mb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
PASC Project Capitalization.Pdf
Table of content Acronyms ........................................................................... 2 THANKS .............................................................................. 3 Introduction ....................................................................... 5 About MBOSCUDA ........................................................ 5 About PASC .................................................................... 5 Section 1: Background and Objectives of the Project .......... 8 1.1 Background and Justification of the Project ............ 8 1.2 Objectives and Expected Results of the Project ...... 10 1.3 Target Population .................................................. 11 1.4 General Approach and Methodology ...................... 12 Section 2: Activities of the Project...................................... 15 Activity 1: Stimulate and accompany the restructuring of emerging Mbororo pastoralist CBOs ............................. 15 Activity 2: Train leaders of Mbororo pastoralist CBOs on group management ................................... 16 Activity 3. Train leaders of Mbororo pastoralist CBOs on Resource Mobilisation................................... 17 Activity 4. Train Mbororo councillors on Lobbying and Advocacy techniques ...................................... 19 Section 3: Outcomes of the Project .................................... 20 3.1 Outcomes at the level of the CBOs ......................... 20 3.2 Outcomes at the level of MBOSCUDA ................... 23 Section 4: Challenges, Lessons and Future Perspectives -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

Ouest Uest E
quête d’assurance quête en transfrontaliers clients Les le Maire et son adjoint et son le Maire Kwemo Pierre fait enfermer ErnestOuandié honorent Patient etNdom Walla Kah Basile, Louka Adamou, Koupit Ouest Echos N° 1171 du 20 du 1171 N° Echos Ouest AFRILAND QUITTE GUINÉE LA EQUATO, LES PRODUCTEURS DE L’OUEST INQUIETS... Récipissé N°341 / RDDJ / C19 / BAPP DEVOIR DE MÉMOIRE : MÉMOIRE DE DEVOIR Since 1994 (vingt troisième année) O O COMMUNE DEBANWA COMMUNE PremierJournal national d’informations Régionales uest uest au 26 Janvier 2021 2021 Janvier 26 au l’arbitrage du Premier Ministre choix dusite et demandent Les populations s’opposent au première chaire Pierre Castel du pays L’Université deDschang hôte de la PARTENARIAT PRIVÉAU CAMEROUN PUBLIC PARTENARIAT CONSTRUCTION DU PEAGE AUTOMATIQUE DEBANDJA AUTOMATIQUE PEAGE DU CONSTRUCTION Tomaïno Ndam Njoya à Foumban à Njoya Ndam Tomaïno Awa se Fonka brûle au contact de E E INSTALLATION DU PRÉFET DU PRÉFET DU NOUN INSTALLATION Michel Eclador PEKOUA Eclador Michel publication de Directeur Les Monts d’Or 2020 2020 d’Or Monts Les Prix : 400 F. CFA F. 400 : Prix LA RÉGION DEL’OUEST RÉGION LA CÉLÈBRE SES AWARDS SES CÉLÈBRE c’est bientôt !!! bientôt c’est Actualités INSTALLATION DU NOUVEAU PRÉFET DU NOUN : Le gouverneur Awa Fonka perd sa sérénité à Foumban La scène a médusé les milliers de populations venus accueillir à la place des fêtes de Foumban, le nouveau préfet du département du Noun, Um Donacien, nommé le 18 décembre 2020 en remplacement de monsieur Boyomo Donatien, muté. l'occasion de la cérémonie de gramme de la plus leur temps à afficher leur mul- Njoya. -

Masks on the Move Defying Genres, Styles, and Traditions in the Cameroonian Grassfields
Masks on the Move Defying Genres, Styles, and Traditions in the Cameroonian Grassfields Silvia Forni n the realm of African art, masks are some of the most This article investigates the longstanding history of commer- exemplary and iconic artworks. Whether displayed cial practices and stylistic experimentation that characterize to be admired for their shape, form, and volumes, or the production of masks and other artworks in the Grassfields presented in dialogue with ethnographic information of Western Cameroon. While I acknowledge the importance of and contextual images, masks are omnipresent in col- long-distance and international trade as an important stimulus lections and displays of African art. As aesthetic and for creativity and artistic production, my intention is to high- ethnographic objects, masks are used as gateways to the under- light the significance of contemporary artistic inventions in Istanding and appreciation of “cultural styles” as well as the for- shaping local understanding of aesthetics and material displays. mal and creative solutions adopted by artists and workshops. Yet Collections, museums, eco-museological itineraries and, more the appeal of masks also relies on their perceived irreducible dif- recently, experimentations and artistic interventions by contem- ference and mysterious spiritual aura. Even when isolated and porary artists Hervé Youmbi and Hervé Yamguen (Fig. 1) have stripped of their fiber costumes and attachments, there is always produced a complex and intriguing regional and national artistic a reference to the body of an absent wearer, thus evoking a sit- scene. Here the taxonomies distinguishing commercial produc- uated and embodied history of production, performance, and tions from “authentic artworks” have been blurred and subverted social meaning that often does not accompany the mask into the in local practices, where masks are now moving between spheres museum. -

Dictionnaire Des Villages Du Département Bamoun 42 P
OFFICE DE LA RECHERCHE REfIlUBLIQUE FEDERALE SCIENTIFIQUE ET 'rECHNIQUE DU OUTRE-MER CAMEROUN CENTRE OR5TOM DE YAOUNDE 1 DICTIONNAIRE DES VILLAGES . DU DEPARTEMENT BAMOUN ~prèS la documentation réunie ~ ~ction de Géographiy de l'ORS~ REPERTOIRE GEOGRAPHIQUE DU CAMEROUN FASCICULE n° 16 SH. n° 44 YAOUNDE Janvier 1968 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fesc. Tabl.eau de là population du Cameroun, 68 p. Fév. 1965 SH. N° 17 Fasc. 2 Dictionnaire des villages du Dia et Lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des ~illages de la Haute-Sanaga, 53 p. Août 1965 SH. N° 23 Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, ~~ p. Octobre 1965 SH. N° ?4 Fasc. 5 Dictionnaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du l'-Jtem 126 p. Décembre 1965 SH. N° 26 Fasc. 7 Dictionnaire des villages de la Mefou 108 p. Janvier 1966 SH. N" 27 Fasc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 5H. N° 28 Fasc. 9 Dictionnaire des villages de la Lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam 60 P. Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko 34 p. Juin 1966 SH 39 Fasc. 13 Dictionnaire des villages de Lom-et-Djérem 35 p. Juillet 1967 SH. 40 Fasc. 14 Dictionnaire des villages de la Kadei 52 p. Août 1967 SH. 41 Fasc. -
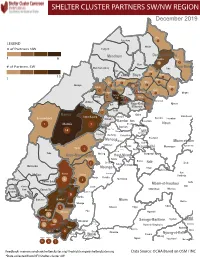
NW SW Presence Map Complete Copy
SHELTER CLUSTER PARTNERS SW/NWMap creation da tREGIONe: 06/12/2018 December 2019 Ako Furu-Awa 1 LEGEND Misaje # of Partners NW Fungom Menchum Donga-Mantung 1 6 Nkambe Nwa 3 1 Bum # of Partners SW Menchum-Valley Ndu Mayo-Banyo Wum Noni 1 Fundong Nkum 15 Boyo 1 1 Njinikom Kumbo Oku 1 Bafut 1 Belo Akwaya 1 3 1 Njikwa Bui Mbven 1 2 Mezam 2 Jakiri Mbengwi Babessi 1 Magba Bamenda Tubah 2 2 Bamenda Ndop Momo 6b 3 4 2 3 Bangourain Widikum Ngie Bamenda Bali 1 Ngo-Ketunjia Njimom Balikumbat Batibo Santa 2 Manyu Galim Upper Bayang Babadjou Malentouen Eyumodjock Wabane Koutaba Foumban Bambo7 tos Kouoptamo 1 Mamfe 7 Lebialem M ouda Noun Batcham Bafoussam Alou Fongo-Tongo 2e 14 Nkong-Ni BafouMssamif 1eir Fontem Dschang Penka-Michel Bamendjou Poumougne Foumbot MenouaFokoué Mbam-et-Kim Baham Djebem Santchou Bandja Batié Massangam Ngambé-Tikar Nguti Koung-Khi 1 Banka Bangou Kekem Toko Kupe-Manenguba Melong Haut-Nkam Bangangté Bafang Bana Bangem Banwa Bazou Baré-Bakem Ndé 1 Bakou Deuk Mundemba Nord-Makombé Moungo Tonga Makénéné Konye Nkongsamba 1er Kon Ndian Tombel Yambetta Manjo Nlonako Isangele 5 1 Nkondjock Dikome Balue Bafia Kumba Mbam-et-Inoubou Kombo Loum Kiiki Kombo Itindi Ekondo Titi Ndikiniméki Nitoukou Abedimo Meme Njombé-Penja 9 Mombo Idabato Bamusso Kumba 1 Nkam Bokito Kumba Mbanga 1 Yabassi Yingui Ndom Mbonge Muyuka Fiko Ngambé 6 Nyanon Lekié West-Coast Sanaga-Maritime Monatélé 5 Fako Dibombari Douala 55 Buea 5e Massock-Songloulou Evodoula Tiko Nguibassal Limbe1 Douala 4e Edéa 2e Okola Limbe 2 6 Douala Dibamba Limbe 3 Douala 6e Wou3rei Pouma Nyong-et-Kellé Douala 6e Dibang Limbe 1 Limbe 2 Limbe 3 Dizangué Ngwei Ngog-Mapubi Matomb Lobo 13 54 1 Feedback: [email protected]/ [email protected] Data Source: OCHA Based on OSM / INC *Data collected from NFI/Shelter cluster 4W. -

MBENGWI COUNCIL DEVELOPMENT PLAN Email: [email protected] Kumbo, the ………………………
REPUBLIQUE DU CAMEROUN REPUBLIC OF CAMEROON PAIX- TRAVAIL- PATRIE PEACE- WORK-FAHERLAND ----------------------------- ----------------------------- MINISTERE DE L’ADMINISTRATION MINISTRY OF TERRITORIAL ADMINSTRATION TERRITORIALE ET AND DECENTRALISATION DECENTRALISATION ----------------------------- ----------------------------- NORTH WEST REGION REGION DU NORD OUEST ----------------------------- ----------------------------- MOMO DIVISION DEPARTEMENT DE MOMO ----------------------------- -------------------------- MBENGWI COUNCIL COMMUNE DE MBENGWI ----------------------------- ------------------------------- [email protected] Kumbo, the ………………………. MBENGWI COUNCIL DEVELOPMENT PLAN Email: [email protected] Kumbo, the ………………………. Elaborated with the Technical and Financial Support of the National Community Driven Development Program (PNDP) March 2012 i MBENGWI COUNCIL DEVELOPMENT PLAN Elaborated and submitted by: Sustainable Integrated Balanced Development Foundation (SIBADEF), P.O.BOX 677, Bamenda, N.W.R, Cameroon, Tel: (237) 70 68 86 91 /98 40 16 90 / 33 07 32 01, E-mail: [email protected] March 2012 ii Table of Content Topic Page 1 INTRODUCTION........................................................................................................ 1 1.1 Context and Justification.............................................................................................. 1 1.2 CDP objectives............................................................................................................. 2 1.3 Structure of the work................................................................................................... -

PC19 Inf. 12 (In English and French / En Inglés Y Francés / En Anglais Et Français)
PC19 Inf. 12 (In English and French / en inglés y francés / en anglais et français) CONVENTION ON INTERNATIONAL TRADE IN ENDANGERED SPECIES OF WILD FAUNA AND FLORA CONVENCIÓN SOBRE EL COMERCIO INTERNACIONAL DE ESPECIES AMENAZADAS DE FAUNA Y FLORA SILVESTRES CONVENTION SUR LE COMMERCE INTERNATIONAL DES ESPECES DE FAUNE ET DE FLORE SAUVAGES MENACEES D'EXTINCTION ____________ Nineteenth meeting of the Plants Committee – Geneva (Switzerland), 18-21 April 2011 Decimonovena reunión del Comité de Flora – Ginebra (Suiza), 18-21 de abril de 2011 Dix-neuvième session du Comité pour les plantes – Genève (Suisse), 18 – 21 avril 2011 PRELIMINARY REPORT ON SUSTAINABLE HARVESTING OF PRUNUS AFRICANA (ROSACEAE) IN THE NORTH WEST REGION OF CAMEROON The attached information document has been submitted by the CITES Secretariat1. El documento informativo adjunto ha sido presentado por la Secretaría CITES2. Le document d'information joint est soumis par le Secrétariat CITES3. 1 The geographical designations employed in this document do not imply the expression of any opinion whatsoever on the part of the CITES Secretariat or the United Nations Environment Programme concerning the legal status of any country, territory, or area, or concerning the delimitation of its frontiers or boundaries. The responsibility for the contents of the document rests exclusively with its author. 2 Las denominaciones geográficas empleadas en este documento no implican juicio alguno por parte de la Secretaría CITES o del Programa de las Naciones Unidas para el Medio Ambiente sobre la condición jurídica de ninguno de los países, zonas o territorios citados, ni respecto de la delimitación de sus fronteras o límites. -

Commodification of Care and Its Effects on Maternal Health in the Noun Division (West Region – Cameroon) Ibrahim Bienvenu Mouliom Moungbakou
Moungbakou BMC Medical Ethics 2018, 19(Suppl 1):43 https://doi.org/10.1186/s12910-018-0286-1 RESEARCH Open Access Commodification of care and its effects on maternal health in the Noun division (West Region – Cameroon) Ibrahim Bienvenu Mouliom Moungbakou Abstract Background: Since the mid-1980s, there has been a gradual ethical drift in the provision of maternal care in African health facilities in general, and in Cameroon in particular, despite government efforts. In fact, in Cameroon, an increasing number of caregivers are reportedly not providing compassionate care in maternity services. Consequently, many women, particularly the financially vulnerable, experience numerous difficulties in accessing these health services. In this article, we highlight the unequal access to care in public maternity services in Cameroon in general and the Noun Division in particular. Methods: For this study, in addition to documentary review, two qualitative data collection techniques were used: direct observation and individual interviews. Following the field work, the observation data were categorized and analyzed to assess their relevance and significance in relation to the topics listed in the observation checklist. Interviews were recorded using a dictaphone; they were subsequently transcribed and the data categorized and coded. After this stage, an analysis grid was constructed for content analysis of the transcripts, to study the frequency of topics addressed during the interviews, as well as divergences and convergences among the respondents. Results: The results of this data analysis showed that money has become the driving force in service provision. As such, it is the patient’s economic capital that counts. Considered “clients”, pregnant women without sufficient financial resources wait long hours in corridors; some die in pain under the indifferent gaze of the professionals who are supposed to take care of them. -
Programming of Public Contracts Awards and Execution for the 2020
PROGRAMMING OF PUBLIC CONTRACTS AWARDS AND EXECUTION FOR THE 2020 FINANCIAL YEAR CONTRACTS PROGRAMMING LOGBOOK OF DEVOLVED SERVICES AND OF REGIONAL AND LOCAL AUTHORITIES NORTH-WEST REGION 2021 FINANCIAL YEAR SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of No Designation of PO/DPO Amount of Contracts No. page contracts REGIONAL 1 External Services 9 514 047 000 3 6 Bamenda City Council 13 1 391 000 000 4 Boyo Division 9 Belo Council 8 233 156 555 5 10 Fonfuka Council 10 186 760 000 6 11 Fundong Council 8 203 050 000 7 12 Njinikom Council 10 267 760 000 8 TOTAL 36 890 726 555 Bui Division 13 External Services 3 151 484 000 9 14 Elak-Oku Council 6 176 050 000 9 15 Jakiri Council 10 266 600 000 10 16 Kumbo Council 5 188 050 000 11 17 Mbiame Council 6 189 050 000 11 18 Nkor Noni Council 9 253 710 000 12 19 Nkum Council 8 295 760 002 13 TOTAL 47 1 520 704 002 Donga Mantung Division 20 External Services 1 22 000 000 14 21 Ako Council 8 205 128 308 14 22 Misaje Council 9 226 710 000 15 23 Ndu Council 6 191 999 998 16 24 Nkambe Council 14 257 100 000 16 25 Nwa Council 10 274 745 452 18 TOTAL 48 1 177 683 758 Menchum Division 27 Furu Awa Council 4 221 710 000 19 28 Benakuma Council 9 258 760 000 19 29 Wum Council 7 205 735 000 20 30 Zhoa Council 5 184 550 000 21 TOTAL 25 870 755 000 MINMAP/Public Contracts Programming and Monitoring Division Page 1 of 37 SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of No Designation of PO/DPO Amount of Contracts No. -

JAKIRI COUNCIL DEVELOPMENT PLAN Kumbo, the ………………………
REPUBLIQUE a DU CAMEROUN REPUBLIC OF CAMEROON PAIX- TRAVAIL- PATRIE PEACE- WORK-FAHERLAND ----------------------------- ----------------------------- MINISTERE DE L’ADMINISTRATION MINISTRY OF TERRITORIAL ADMINSTRATION TERRITORIALE ET AND DECENTRALISATION DECENTRALISATION ----------------------------- ----------------------------- NORTH WEST REGION REGION DU NORD OUEST ----------------------------- ----------------------------- BUI DIVISION DEPARTEMENT DE BUI ----------------------------- -------------------------- JAKIRI COUNCIL COMMUNE DE JAKIRI ----------------------------- ------------------------------- [email protected] Kumbo, the ………………………. Email: [email protected] COUNCIL DEVELOPMENT PLAN Kumbo, the ………………………. Elaborated with the Technical and Financial Support of the National Community Driven Development Program (PNDP) June 2012 i JAKIRI COUNCIL DEVELOPMENT PLAN Elaborated and submitted by: Sustainable Integrated Balanced Development Foundation (SIBADEF), P.O.BOX 677, Bamenda, N.W.R, Cameroon, Tel: (237) 70 68 86 91 /98 40 16 90 / 33 07 32 01, E-mail: [email protected] June 2012 ii Table of content Table of content ....................................................................................................................................................... iii EXECUTIVE SUMMARY ............................................................................................................................................. viii 1.NTRODUCTION ...................................................................................................................................................... -

Community Media Is 10% Media and 90% Community a Mapping Project on the Potentials of Community Media in Cameroon in Times of Conflict
1 CCMN Cameroon Community Media Network Community Media is 10% Media and 90% Community A Mapping Project on the Potentials of Community Media in Cameroon in Times of Conflict A project by: Financed by: P.2 Editorial P.5 Community Media as Conveyer of a peaceful solution to the current Anglophone Crisis P.8 Community Media produce Open Spaces for Communities in Times of War P.12 CCMN In numbers P.15 List of CCMN Members P.17 Who is CCMN P.19 We’ve come a long way! We Need Women’s voices in media P.22 CCMN Staff P.24 CCMN and Peace Journalism Peace Journalistic Approaches and Professionalism can lower P.26 Risk for Journalists in Conflict Situation P.28 CCMN in South West/Littoral P.30 CCMN in North West/West P.34 Program Content P.36 Languages in the Network 2 3 There is no better time than now to sound the Community media play a crucial role in favouring clarion call for peace public debate and preserving the country’s precious diversity of people and cultures RT REV FONKI SAMUEL JOHANNES SINGER Moderator of the PCC Project Officer Cameroon Bread for the World Over the past years and decades, media consumption At Bread for the World, we are convinced that Cameroon Community Media “ been out of school for the past three academic years – has changed profoundly all over the globe. We have Cameroon’s community media precisely play a crucial Network (CCMN) which has brought the call for peace is urgent! access to an ever broadening range of international role in favouring public debate and preserving the together media practitioners and We are grateful to our partners, Bread for the World media and often receive the same „latest news“ – country’s precious diversity of people and cultures.