EHA Annual Report 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dhulia District
FOREST RESOURCES OF DHULIA DISTRICT OF MAHARASHTRA STATE FOREST SVB."BY OF INDIA CENTRAL ZONE NAGPUR 1988 M.bMIJ ~... ~. ~~ -. ----~-. I -= e • ••~, , FOREST RESOURCES OF DHULIA DISTRICT OF MAHARASHTRA STATE FOREST SVBJ7'EY OF INIJI~t CENTRAL ZONE NAGPUR 1988 PRE l' l\ C Ii: This report contains the result of the inventory of the for"ests of Dhul ia district in Maharashtra, wade b~' the Central Zone (~f the Forest Survey of India. The inventory waS wade during the period November .1982 to March 1983. The report covers that part of the distr'ict which i:.> included in North Dhulia and West Dhulia Forest Divisions. P~rt of the district covered in Mewasi Forest Division was surveyed during 1977-79 and a report on the forest resources of this part was published earlif:r. The total forest area of Dhulia district ~s 4503 Sq.km., but this l~eport describes Uw situation of ~. about 3970 Sq. km. forest area which forror..; part of North & W~st Dhulia Forest Divisions. The total growing stock in the forests of 3 North & Y~est Forest Divis ions is about 3.38 x l~ m . The figure of average growing ~,;tock in one ·hectare of forest works out at 32.86 m3 . The three sp~cies which occur in preponderance are Anogeissus latifolia, Tectona grandis and Boswellia serrata. The three species account for near ly t .... VlO third of the growing stock. I About 40% of the populat.ion in the region covered by the inventory is that of t~e tribals who depend substantially on the forest for their livelihood, But unfortunately the forest resou~ce is fast dwindling on aocount of various biotic pressures. -

Response to COVID-19 in Difficult Areas a Quick Look at Our Support to COVID Healthcare Initiatives Outside Our Regions of Focus
December 2020 Field Note # 6 Response to COVID-19 in Difficult Areas A quick look at our support to COVID healthcare initiatives outside our regions of focus 1. Context As the COVID-19 situation unravelled itself, it was becoming evident that an integrated healthcare response is the only way to effectively contain the speed and spread of infection in the country. The Foundation started supporting such an integrated response in select-regions of states where we have our own field operations or our partners have a strong ground presence. However, learning from our experiences from the initial period of organising immediate responses to healthcare needs, we found immense value in supporting credible not- for-profit, public spirited organisations to enable a community-based COVID-19 response in some of the most difficult locations situated outside our regions of focus. Fig. 1: Illustrative reach of such support In brief, such support is organised around following principles: a. These not-for-profit, public spirited organizations must, on priority, respond to the COVID-19 specific healthcare needs of the communities in rural/tribal areas b. They should maximise focus on community-based COVID healthcare work to build community awareness, surveillance, isolation and timely referral c. These could be well-reputed, public spirited hospitals building their COVID preparedness, isolation of suspected cases, RT-PCR testing and management of confirmed cases d. For management of confirmed cases at facility level, their focus should be more on provisioning secondary healthcare rather than tertiary or quaternary care The organisations that have been selected for this support have been categorised into the following: Category A: Integrated COVID response at community and facility level Category B: COVID response only at community level Category C: COVID response only at the facility level or hospital setting In addition, we also supported a few organizations who were doing good work in difficult-to-access regions, even if they did not have a significant COVID response as of then. -

Groundwater Brochure the Dang District Gujarat
For Official Use Technical Report Series GROUNDWATER BROCHURE THE DANG DISTRICT GUJARAT Compiled by B.K.Gupta Scientist – C Government of India Ministry of Water Resources Central Ground Water Board West Central Region Ahmedabad March, 2014 THE DANG DISTRICT AT A GLANCE Sl.No. Items Statistics 1 GENERAL INFORMATION i) Geographical area as per state territory/as per village papers 1764 (Sq. Km) ii) Administrative Divisions (As on 3/2010) : Number of Talukas/ One / Number of villages/ No of villages having drinking water facility as on 1.04.2009 311/311 iii) Populations (As on 2011 census) 227000 Population density 126/sq.km iv) Average Annual Rainfall (mm) (1951to 1980) 1928, normal annual rain fall (mm), 2011 1635 2 GEOMORPHOLOGY Major Physiographic Units: Deccan Trap country, terraced topography with flat topped conical hills, Small plateau and steep sided narrow valleys. ( RL between 105 to 1317 m above sea level) Major Drainages: Purna, Ambika, Khapri , Gira and Ghogha 3 MAJOR SOIL TYPES: Lateritic soils, deep black clayey and loamy soils and red sandy soils. 4 NUMBERS OF GROUND WATER MONITORING WELLS CGWB (As on 31-03-2012) No of Dug Wells 25 No of Piezometers 2 5 PREDOMINANT GEOLOGICAL FORMATIONS: Deccan trap basalt with dykes. 6 HYDROGEOLOGY Major Water Bearing Formations: Deccan trap basalt with dikes and alluvium. Pre- monsoon depth to water level ( May 2012) 2.89m (Jakhana) to 12.38 m ( Mheskatri) Post- monsoon depth to water level (November 2012) 0.50m (Jakhana/ChinchPada/Ghubita) to 9.55m (Mhesktri) The seasonal ( Pre-Post -

Sr.No. First Name Last Name Designation Email ID STD Code Contact No
Directorate of Vocational Education & Training,Maharashtra State 3-Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 Phone :+91-22-2262 0293/2262 0603/2262 0604 Fax:+91-22-2265 9235 (Training)/2267 5628 (Education) Website:www.dvet.gov.in Contact Details Sr.No. First Name Last Name Designation Email ID STD Code Contact No. Office Name, Address (including District / Taluka) DVET HO 1 Anil Jadhao I/C Director [email protected] 022 22695819 Directorate of Vocational Education & Training, 3- Ext:4004 Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 2 Joint Director [email protected] 022 Directorate of Vocational Education & Training, 3- Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 3 Anil Jadhao Joint Director [email protected] 022 22621008 Directorate of Vocational Education & Training, 3- Ext:2001 Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 4 Prafulla Wakade Joint Director [email protected] 022 22694598 Directorate of Vocational Education & Training, 3- Ext:2002 Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 5 Deputy Director [email protected] 022 Directorate of Vocational Education & Training, 3- Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 6 Yogesh Patil Deputy Director [email protected] 022 22694597 Directorate of Vocational Education & Training, 3- Ext:1003 Mahapalika Marg, P.O. Box 10036, Mumbai , District : Mumbai, Taluka: Mumbai, Pin 400 001 7 Anil Gavit Deputy Director [email protected] 022 Ext:2001 Directorate of Vocational Education & Training, 3- Mahapalika Marg, P.O. -

District Census Handbook, Dhule
CENSUS OF INDIA 1981 DISTRICT CENSUS HANDBOOK DHULE Compiled by THE MAHARASlITRA CENSUS DIRECTORATE BOMBAY Price : Rs. 30.00 PRINTED IN INDIA BY THE MANAGER. YERA VDA PRISON PRESS, PUNE AND PUBLISHED BY THE DIRECTOR, GOVERNMENT PRINTING AND STATIONERY, MAHARASHTRA STATE, BOMBAY-400 004 1985 '": ~co ":;: 0 • u © • 0 B .~ .g Q: :r • cr "0 @ I '1 1: >: 1~ '" I w '" " .....J . 0 • ~ ~ e 0 ::> I c '"~ <l: 0 · ::I: e i 0 a:: Ol 0 0- g~ 2" 0 z." ] ~ I ." DC Vl .2 0 Q ; 0 0 ~ ~ 0 0 1j <l: cr 0 :l"Pj "0 .c C ~ .. t- g ~ a:: 0 ~ ,. .c § ;~ <l: 0 6 ,. E '" I U ~ ~ ~ ~ 0 ~ ~ Vi < B-1 <l: . ! ~ ; ~ · Vi 0> ~ i < . ~~ ~ ;3 0 cr I C "0 · ~ C 2 ~ ·0 ~ 0 i 0 0";' x· t- s ('; c. 0 0 ~ . o • If) ,f~ ~2 ·~ t I V> § ;> ~ ~I '" cii Ii: :0" £ a · V> '" 0 ~ 1- " () ..(- /r ,9 tl' 8- 'J Ir J " & J 0 S <:) i" ~ I U- ";, 0 "r % ~ "'(j.\6,;~r§\ ,\oc.: ~'r::/l.O «- po.~tc.~ " ~ .. -:' ..l.. le ~ .:t () If) 'Of <l: <! ~ ... (J 0: 0 ... .£ i, "0 '"" </I 1 <!> ,.0 ~ 0 ~ .> I ':i , l, V> "8" .c ~r·,-- l' "0 .. ,.. i .~ ~ I'. ~ s:::" ~ "0 i'" 1 .c .c ~ "~ " U; 0 " a E ~ 0- ~ l' ::. ] I "0 ~ :r :; Vl . a :;: , VI ~ r e-'" (\ ~~ ..] MOTIF 'The Bhils of Maharashtra are mainly concentrated in Dhule district. They have kng history since ancient times. The earliest mention of their name occurs in the Ramayana and the Maha bharata. Bhils possibly belong 10 a proto Mediterranean race who spread far and wide when a climatic crisis occurred in the gral>s steppes 0 f the Sahara. -

Census of India 2011
Census of India 2011 GUJARAT SERIES-25 PART XII-B DISTRICT CENSUS HANDBOOK THE DANGS VILLAGE AND TOWN WISE PRIMARY CENSUS ABSTRACT (PCA) DIRECTORATE OF CENSUS OPERATIONS GUJARAT r INDIA u p a v GUJARAT a N o F T DISTRICT THE DANGS ro m S C T A o KILOMETRES n I g a 10 5 0 10 R d A h T R.Z an A kh T ari P F ro a m ir .G I V R y a S r 0 a 8 H S R I D R .P u rn a 2 T 7 1 H S 4 F 1 S rom SH Va H lsa d 1 I 7 4 R ari hap A R.K S V at A WAGHAI lg abu N B To S T H AHWA 1 4 H C I R T S I D R . M A m b SH i 1 c 5 a R S .Kha pari BOUNDARY, STATE............................................ ,, DISTRICT...................................... R . A S URBAN AREA WITH POPULATION S m H A H IV, V, VI ................................................................... b 1 i 5 c 1 a 7 4 HEADQUARTERS: DISTRICT/ TALUKA ............. / SAPUTARA A STATE HIGHWAY................................................. SH 174 T o IMPORTANT METALLED ROADS........................ H N a s na ik RAILWAY LINE, NARROW GAUGE...................... urga m S R Fro A RIVER AND STREAM............................................ A PART OF DISTRICT THE DANGS CENSUS OF INDIA 2011 GUJARAT SERIES-25 PART XII - B DISTRICT CENSUS HANDBOOK THE DANGS VILLAGE AND TOWN WISE PRIMARY CENSUS ABSTRACT (PCA) Directorate of Census Operations GUJARAT Motif Purna Wildlife Sanctuary The Purna Sanctuary at a distance of about 60 km north of Dangs is situated at Mahal in the Western Ghats of Gujarat. -
Application ID Name of Candidate Address Email Id Mobile No DOB
MAHARASHTRA INFORMATION TECHNOLOGY CORPORATION (A Government of Maharashtra Enterprise) Result Report of Agriculture Department - Krishi Sevak Examination - 2019 Circle : Nashik Sufficient Employee Son/daug revenue Non- 1991 of Handicapped Earth hter of Final ST-PESA proof_ST- ST-PESA ST-PESA Creamy Sport 865 census Election Ex- Ex- Project quake Orphan Part time Govt. Highest Educational sucidal Normalized Application ID Name of candidate Address Email Id Mobile No DOB Gender Category Division Applied for or Not PESA District Taluka PH or not PH Type layer person border employee after 1994 serviceman servicemen affected affected Candidate employee Employee Qualification farmer Marks AT-UMBARDE POST-MANI TEL-SURGANA AGRICLR_KS_0008674 RAJENDRA GOPAL GAVIT DIST-NASHIK 422211 [email protected] 9921819629 3/2/1996 MALE ST Krishi Sevak_Nashik Yes Yes NASHIK SURGANA No No No No No No No No No No No No No Under graduate No 134 AT BORVIHIR POST RAIPUR TAL NAVAPUR AGRICLR_KS_0014401 SUNIL VIKRAM GAVIT DIST NANDURBAR 425418 [email protected] 7276895611 6/1/1992 MALE ST Krishi Sevak_Nashik Yes Yes NANDURBAR NAVAPUR No No No No No No No No No No No No No Graduate No 126 At-Kerobanagar(Vathoda) Post- Kelzar Tq- AGRICLR_KS_0021714 PRAKASH LAXMAN THAKARE Baglan(Satana) Dist-Nashik 423301 [email protected] 9404142405 9/9/1988 MALE ST Krishi Sevak_Nashik Yes Yes NASHIK BAGLAN No No No No No No No No No No No No No Post-Graduation No 123 At karambhel post dalwat Tal igatpuri dist [email protected] AGRICLR_KS_0056979 Jayashree -

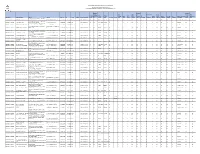
Dedicated COVID Health Center / DCHC Facility Wise Report 17 Dec 2020
CATII - Dedicated COVID Health Center / DCHC Facility Wise Report 17 Dec 2020 Compa tible Isolati Total Isolatio to on O2 Isolatio n beds O2 Biome beds Total No of Manif State / UT Facilty n beds for Suppor Availabl Availabl dical Updated # District Name Facilty Name Category Type of ICU Ventila old Name ID (excludi Suspect ted e ppes e n95 Waste On Confir beds tors Availa ng ICU ed beds Manag med ble beds) cases ement Cases Syste m Swasthya hospital Cat. II - Dedicated medical COVID Health Private 1 Maharashtra AHMEDNAGAR reasearch centre Center / DCHC Hospitals 33221 18 13 5 5 5 3 Yes 100 380 Yes 16/12/2020 Cat. II - Dedicated Pathak Hospital COVID Health Private 2 Maharashtra AHMEDNAGAR Sangamner Center / DCHC Hospitals 35081 10 9 1 5 2 1 Yes 25 25 Yes 9/12/2020 Sai Covid Care Cat. II - Dedicated Centre COVID Health Private 3 Maharashtra AHMEDNAGAR Shrirampur Center / DCHC Hospitals 35838 25 22 3 22 3 1 Yes 200 200 Yes 2/10/2020 Medicare Hospital Cat. II - Dedicated Bolhegaon Phata COVID Health Private 4 Maharashtra AHMEDNAGAR Nagar Center / DCHC Hospitals 34094 20 15 5 20 10 2 Yes 500 500 Yes 16/10/2020 Cat. II - Dedicated Ahmednagar Burn COVID Health Private 5 Maharashtra AHMEDNAGAR Centre Center / DCHC Hospitals 35603 12 12 0 12 2 2 Yes 1000 1000 Yes 10/9/2020 Suvidha Hospital, Bhide Chowk Cat. II - Dedicated Savedi naka COVID Health Private 6 Maharashtra AHMEDNAGAR Ahmednagar Center / DCHC Hospitals 33444 15 12 3 5 7 0 Yes 15 50 Yes 21/09/2020 Harishchandra Multispeciality Cat. -

CIN/BCIN Prefill Company/Bank SIEMENS LIMITED Date of AGM
Note: This sheet is applicable for uploading the particulars related to the unclaimed and unpaid amount pending with company. Make sure that the details are in accordance with the information already provided in e-form IEPF-2 L28920MH1957PLC010839 12-FEB-2021 CIN/BCIN Prefill Company/Bank SIEMENS LIMITED Date of AGM FY-1 FY-2 FY-3 FY-4 FY-5 FY-6 FY-7 Sum of unpaid and unclaimed dividend 0.00 0.00 0.00 7564908.00 0.00 0.00 0.00 Number of underlying Shares 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of matured deposits 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of matured debentures 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of application money due for refund 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of interest on matured deposits 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of interest on matured debentures 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of interest on application money due for refund 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Redemption amount of preference shares 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sales proceed for fractional shares 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Sum of Other Investment Types 0.00 0.00 0.00 0.00 0.00 0.00 0.00 Validate Clear Is the shares Is the transfer from Proposed Date of Investment Investor Middle Investor Last Father/Husband Father/Husband Father/Husband Last DP Id-Client Id- Amount Joint Holder unpaid Investor First Name Address Country State District Pin Code Folio Number Investment Type transfer to IEPF PAN Date of Birth Aadhar Number Nominee Name Remarks (amount / Financial Year Name Name First Name Middle Name Name Account Number transferred Name suspense (DD-MON-YYYY) shares )under account any litigation. -

Maharashtra State Legislative Council Electoral Roll-2017 Nashik Division Teacher Constituency DISTRICT :-Dhule PART NO -: 7 TALUKA :-SAKRI Mother Roll
Maharashtra State Legislative Council Electoral Roll-2017 Nashik Division Teacher Constituency DISTRICT :-Dhule PART NO -: 7 TALUKA :-SAKRI Mother Roll Name Of Elector Name if Father /mother Address Gende Sr No Schoo/College Name Age EPIC No Elector Photo 1 AAHIRRAO PANKAJ AAHIRRAO DAMODAR VIDYA NAGAR SAKRI DIST DHULE AUIDYAGIK PRASHIKSHAN 46 M 0 SANSTHA, SAKRI TAL.SAKRI DIS 2 ADAGLE KHUSHAL ADAGLE PARBAT ARIHANT NAGAR SAKRI DIST. JANATA MADHYAMIK VIDYALAY, 43 M 0 DHULE VITAI, TAL.SAKRI DIST.D 3 AGRAWAL RAJENDRA AGRAWAL VISHNUDAYAL SUTAR GALLI SAKRI DHULE NEW ENGLISH SCHOOL & 54 M 0 KANISHTHA MAHAVIDYALAY SAKRI 4 AHER NIMBA AHER HARI 14, ARIHANT NAGAR, AT. PO. V.V.M.S S.G.PATIL ARTS, SCIENCE 57 M 0 NAMPUR, TAL. SATANA, DIST. & COMMERCE COLLEGE NASHIK 5 AHIRE BABITA AHIRE RAMDAS AT POST BEHED TA SAKRI DIST NEW ENGLISH SCHOOL SAKRI DIS 47 F ZQS56502876 DHULE T DHULE 6 AHIRE BALU AHIRE GOPAL AT POST NIJAMPUR TAL SAKRI MAHATMA GANDHI VIDYALAYAA 56 M DKZ1062009 DIST DHULE VASKHEDI TAL SAKRI DIST 7 AHIRE BHAIYYASAHEB AHIRE JIJABRAO AT. PO. AINCHALE, TAL. SAKRI, SHIVAJI MADHYAMIK VIDYALAYA, 31 M 0 DIST. DHULE VALHAVE, POST. AMKHEL 8 AHIRE BHAUSAHEB AHIRE POPAT BALHANE SAKRI DHULE SANJAY GANDHI SEC. & HIGH SEC 46 M 0 SCHOOL KUDASHI TAL. 9 AHIRE CHOTIRAM AHIRE SONU AT CHINCHPADA POST INDRA GANDHI MADHYAMIK 26 M 0 PANKHEDA TA SAKRI DIST DHULE VIDYALAY PIMPALNER TA SAKRI 1 Maharashtra State Legislative Council Electoral Roll-2017 Nashik Division Teacher Constituency DISTRICT :-Dhule PART NO -: 7 TALUKA :-SAKRI Mother Roll Name Of Elector Name if Father /mother Address Gende Sr No Schoo/College Name Age EPIC No Elector Photo 10 AHIRE DINESH AHIRE BHIKAN AT POST BALHANE TAL SAKRI NEW ENGLISH SCHOOL BALHANE, 34 M 0 DIST DHULE TAL SAKRI DIST DHULE 11 AHIRE DIPCHAND AHIRE SAJAN AT. -

District Census Handbook, Nashik, Part XII-A & B, Series-14
CENSUS OF INDIA 1991 DISTRICT CENSUS HANDBOOK NASHIK Compiled by THE MAHARASHTRA CENSUS DIRECTORATE PRINTED IN INDIA BY THE MANAGER, GOVERNMENT PRESS, MUMBAI-400 004 AND PU:BLISHED BY THE DIRECTOR, GOVERNMENT PRINTING AND STATIqNERY MAHARASHTRA STATE, MUMBAI-400 004. 1995 Price Rs. 100 i I I ~ ~ '; z ~ ~ I- ~ I I ct ® D:: 1) oCt J: oCt - :IE E e is '" MOTIF 'Grapes' of Nashik district are famous for their exhilarating taste and rich flavour. It relished by the people all over India and highly in demand thi~ fruit which is a table fruit of the rich and dream of the poor. Grapes account one third area of the total area under fruit cultivation. Agriculture is the main economic activity of the district -and about 70 per cent working population is dependant on agriculture occupation. Since the commen cement of the five years plans, a number of schemes, regarding plantation of fruits und~rtaken by the Govern ment and due to planning schemes there is marked increase in the fruit products. The soil, climate and sufficient water of tapi and Godavari rivers is favourable for frutis. CONTENTS PAGE Foreword v Preface ix Acknowledgements xi District Highlights - 1991 Census xiii Name of the headquarters of Districttrahsil, their rural/urban status and distance from district headquarters XIV Important Statistics - I (a) 1 Important Statistics - I (b) 4 Ranking of tahsils in the district - II 6 Summary Table 1 - Population of the District at the Censuses from 1901 to 1991 8- Summary Table 2 - Number of inhabited villages and related population in 9 specified population size ranges. -

List for Website Updation
Investor First Investor Last Amount to be Proposed date of Name Investor Middle Name Name Address Country State District Pin Code Folio Number transferred Transfer to IEPF NILKANTH,870/2B,BHANDARKAR MR HARISHCHANDRAKOLTE NA ROAD, PUNE INDIA MAHARASHTRA PUNE 411004 PTSE0000093 294000.00 31-AUG-2020 NATIONAL HSG.SOC,GATE NO.2,HOUSE NO.44, BANER MR DILIPCHAVAN NA RD.PUNE INDIA MAHARASHTRA PUNE 411007 PTSE0000176 1050.00 31-AUG-2020 ASHOKA THILLERY CANNANORE MR D UNNIKRISHNAN KERALA INDIA KERALA CANNANORE 670001 PTSE0000291 8750.00 31-AUG-2020 FLAT 5,BLDG.NO.8-17,KUBERA PARK MR ISHRATALI NA KONDHWA,LULLANAGAR,PUNE INDIA MAHARASHTRA PUNE 411040 PTSE0000304 8750.00 31-AUG-2020 BLOCK NO. 2, INDIRA APTS., CHINTAMAN NGR., SAHAKAR MR CHANDRASHEKHARBHIDE NA NGR.,PUNE INDIA MAHARASHTRA PUNE 411009 PTSE0000313 4375.00 31-AUG-2020 NO 9 SANO LAI APARTMENTS MS VIDYASWAMINATHAN NA SALISBURY PARK PUNE INDIA MAHARASHTRA PUNE 411037 PTSE0000350 13125.00 31-AUG-2020 A3/12 ROYAL ORCHARD D P ROAD MR SUDHIRNERUKAR NA AUNDH PUNE INDIA MAHARASHTRA PUNE 411017 PTSE0000379 875.00 31-AUG-2020 C-4,VISHWAKARMA NAGAR SUS MR NITINAMBHAIKAR NA ROAD, PASHAN PUNE INDIA MAHARASHTRA PUNE 411021 PTSE0000578 3500.00 31-AUG-2020 MR ALINDPRASAD NA A 552 SARITA VIHAR NEW DELHI INDIA DELHI NEW DELHI 110028 PTSE0000614 3500.00 31-AUG-2020 FLAT NO 1 PLOT NO B-82 TULSHIBAGHWALE COLONY MR PANKAJAMBARDEKAR NA SAHAKARNAGAR NO 2 PUNE INDIA MAHARASHTRA PUNE 411009 PTSE0000639 3500.00 31-AUG-2020 181 SHURKWAR PETH SHINDI ALI MR GOPALDEORE NA PUNE INDIA MAHARASHTRA PUNE 411002 PTSE0000659 3500.00 31-AUG-2020 B-7/99 SHANTHI RAKSHAK SOC.