Social Impact of the Arfon Community Link Project
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gwynedd Bedstock Survey 2018/19 Content 1
Tourism Accommodation in Gwynedd Gwynedd Bedstock Survey 2018/19 Content 1. Introduction ................................................................................................................................... 1 2. Main Findings of the Gwynedd Tourism Accommodation Survey 2018/19 .................................. 2 3. Survey Methodology .................................................................................................................... 14 4. Analysis according to type of accommodation ............................................................................ 16 5. Analysis according to Bedrooms and Beds................................................................................... 18 6. Analysis according to Price ........................................................................................................... 21 7. Analysis according to Grade ......................................................................................................... 24 8. Comparison with previous surveys .............................................................................................. 26 9. Main Tourism Destinations .......................................................................................................... 29 10. Conclusions .................................................................................................................................. 49 Appendix 1: Visit Wales definitions of different types of accommodation .......................................... 51 Appendix 2: -

Moving Mountains! Under the Care of Cadw a Walk Around the Slate Landscape of Llanberis Duration: 1½ Hours - Easy-Moderate Walk
FOLLOW THE STORY: Discover more about the life of the quarrymen and their families in north Wales by visiting Cae’r Gors, the childhood home of author Kate Roberts in Rhosgadfan near Caernarfon, now Moving Mountains! under the care of Cadw A Walk around the slate landscape of Llanberis Duration: 1½ hours - Easy-Moderate Walk Start at the car park at Padarn Leaving the museum, turn right Country Park (1) Postcode LL55 and follow the wall to a footbridge 4TY. Towering above you are the over the river and across the park slabs and waste of Dinorwic Quarry, to Dolbadarn Castle (6) built by once one of the largest slate Llywelyn the Great. quarries in the world. In the late 19th century it employed 3000 On reaching the main road you will men who produced 100,000 tons of see the Snowdon Mountain Railway slate per year. Station (7). Finish at the Electric Mountain (8) visitor centre and take Keeping the railway on your right a tour of the power station. There take a walk up the designated is also an Our Heritage exhibition National Slate Museum © Our Heritage footpath and up the steps to the here. Quarry Hospital (2). Opened in the 1860s the hospital provided medical care to quarrymen. It NORTH Quarry is now open to the public and Hospital features a display of the innovative 2 equipment once used there, 0 metres 200 including amputation tools and an 3 x-ray machine. Caernarfon Vivian Quarry From here follow the road past Llyn Padarn the vast hole of the now flooded Llanberis Lake Railway 4 Gilfach Ddu Railway Station Vivian Slate Quarry (3). -

Penrhos, Waunfawr, Gwynedd LL55 4AJ £169,995
Penrhos, Waunfawr, Gwynedd LL55 4AJ ● £169,995 Unlock the potential in this attractive home. Detached House In Need Of Renovation . Economy 7 Night Storage Heating . 3 Bedrooms, Bathroom & Dressing Room . Superb Views – Scenic Setting . Sizeable Lounge, Sitting & Dining Room . Generous Rear Garden & Off Road Parking . Fitted Kitchen & Workshop/Utility Room . Advantage Of No Onward Chain . Partial uPVC Double Glazing . Viewing Is Highly Recommended Cy merwy d pob gof al wrth baratoi’r many lion hy n, ond eu diben y w rhoi arweiniad Ev ery care has been taken with the preparation of these particulars but they are f or cyff redinol y n unig, ac ni ellir gwarantu eu bod y n f anwl gy wir. Cofiwch ofy n os bydd general guidance only and complete accuracy cannot be guaranteed. If there is any unrhy w bwy nt sy ’n neilltuol o bwy sig, neu dy lid ceisio gwiriad proff esiynol. point which is of particular importance please ask or prof essional v erification should Brasamcan y w’r holl ddimensiy nau. Nid y w cyf eiriad at ddarnau gosod a gosodiadau be sought. All dimensions are approximate. The mention of any f ixtures f ittings &/or a/neu gyf arpar y n goly gu eu bod mewn cyf lwr gweithredol eff eithlon. Darperir appliances does not imply they are in f ull eff icient working order. Photographs are ffotograff au er gwy bodaeth gyff redinol, ac ni ellir casglu bod unrhy w eitem a prov ided f or general inf ormation and it cannot be inf erred that any item shown is ddangosir y n gy nwysedig y n y pris gwerthu. -

Vaynol Old Hall
NORTH WEST WALES DENDROCHRONOLOGY PROJECT DATING OLD WELSH HOUSES VAYNOL OLD HALL, Pentir, near Bangor, Gwynedd (formerly Caernarfonshire) Parish: Pentir. NGR: SH 5384 6953 © Crown copyright: Royal Commission on the Ancient and Historical Monuments of Wales: Dating Old Welsh Houses: North West Wales Dendrochronology Project HOUSE DETAILS: An ‘important sub-medieval house which appears to be constructed in at least three or four phases, beginning in the early-mid C16 as a 2-unit house with lateral chimney, consisting of the ground floor of hall, passage and small outer room. It reached the present E-shaped plan in the early-mid C17, with the addition of a storeyed porch over the entrance, and a similar oriel bay at the E end: rear stair wing dated on close- studding, 1638. The E-plan was completed towards the end of the C17 with the addition of a larger N wing on the W side [...]. Outbuildings attached to the W end are later, mostly C19.’ (CADW listing description). ‘Lavish version of Snowdonia plan-type with projecting oriel, porch and later kitchen (?1660s) giving a busy front elevation. House has a contemporary rear parlour wing. Service rooms were in basement under the hall. Hall has a lateral chimney, framed ceiling, 16 panels; broad chamfered beams with curved stops with a torus’ (Richard Suggett, RCAHMW). Description in RCAHMW Caernarvonshire Vol. II, no. 1387a. Cantref: Arfon. Commote: Maenol Bangor (Atlas of Caernarvonshire p 71). Dendrochronology results: (a) Hall Range – felling dates: Winter 1557/8 and Summer 1562. Lower purlin 1561 (30½C); Principal rafters (3/4) 1557(52C), 1551(19+8C NM); 1536(17¼C NM); Tiebeams (0/2); Strut (0/1); Collar (0/1); (b, c) Middle Range and Rear Range – felling date: Winter 1628/9. -
Welsh Indices of Multiple Deprivation Chapter 17 – Figure 2
DOCUMENT 5.17.1.2 Welsh Indices of Multiple Deprivation Chapter 17 – Figure 2 National Grid (North Wales Connection Project) Regulation 5(2)(a) including (l) and (m) of the Infrastructure Planning (Applications: Prescribed Forms and Procedure) Regulations 2009 Application Reference EN020015 September 2018 ¯ NWC ROUTE LEGEND AMLWCH PORT LLANBADRIG 1 of 1 AMLWCH RURAL MECHELL N A TIO SEC LLANEILIAN HOLYHEAD TOWN LEGEND PORTHYFELIN 2 B MOELFRE ON CTI LLANFAETHLU SE ORDER LIMITS - OPTION A PORTHYFELIN 1 SECTION CUTLINES MORAWELON LLANNERCH-Y-MEDD B N WELSH INDEX OF MULTIPLE O TI DEPRIVATION (WIMD) 2014 LONDON ROAD C E BRYNTEG S 10% MOST DEPRIVED C N PARC A'R O MYNYDD TI C LLANBEDRGOCH 10-20% MOST DEPRIVED E VALLEY 2 S LLANGOED TREARDDUR 2 20-30% MOST DEPRIVED LLANDDYFNAN VALLEY 1 MAESHYFRYD PENTRAETH LLANFAIR-YN-NEUBWLL 1 30-50% MOST DEPRIVED KINGSLAND 50% LEAST DEPRIVED BODFFORDD C N CYNGAR BEAUMARIS TREARDDUR 1 LLANFAIR-YN-NEUBWLL 2 BRYNGWRAN IO T MENAI C (BANGOR) E TUDUR S CWM CADNANT CEFNI GLYDER D CADNANT N ABERFFRAW & IO (ISLE OF HIRAEL & GARTH 1 T ANGLESEY) RHOSNEIGR 2 C PANDY E HIRAEL & S TYSILIO GARTH 2 BRAINT DEINIOL BRYN LLANFIHANGEL D YSGEIFIOG MARCHOG 2 N GWYNGYLL ABERFFRAW & O I E MARCHOG 1 RHOSNEIGR 1 T BODORGAN C N DEWI E IO E HENDRE (GWYNEDD) S T N PENTIR 1 OGWEN 2 C IO PENTIR 2 E T S C LLANIDAN F E N ARLLECHWEDD S IO T C E S Y FELINHELI OGWEN 1 BETHEL & RHOSYR CWM-Y-GLO 1 TREGARTH PENISARWAUN & MYNYDD GERLAN LLANDYGAI MENAI (CAERNARFON) LLANRUG CADNANT (GWYNEDD) SEIONT 2 BETHEL & DEINIOLEN SEIONT 1 CWM-Y-GLO 2 PEBLIG BONTNEWYDD (CAERNARFON) LLANBERIS LLANWNDA GROESLON TALYSARN A 11/07/2018 ENVIRONMENTAL STATEMENT JB HC EK PENYGROES WAUNFAWR (GWYNEDD) Rev Date Description GIS Chk App LLANLLYFNI Scheme: & CLYNNOG NORTH WALES CONNECTION PROJECT Document Number: 5.17.1.2 Document Title: FIGURE 17.2 WELSH INDICES OF MULTIPLE DEPRIVATION OPTION A Creator: Date: Checker: Date: Approver: Date: Contains OS data © Crown copyright and database right 2018. -

3 Stad Cae Uchaf, Rhosgadfan, Gwynedd LL54 7HR New Price
3 Stad Cae Uchaf, Rhosgadfan, Gwynedd LL54 7HR ● New Price £164,500 A practical family home with exceptional views - an excellent choice for sure! . Modern Detached Dormer Bungalow . Superb Sea Views - Especially From 1st Floor . Spacious Family Sized Accommodation . Sizeable Gardens & Decked Patio . 3 Bedrooms - Master With En-suite . Off Road Parking For 2 Vehicles . 2 Reception Rooms & Useful Utility . Pleasant Rural Village Location . uPVC Double Glazing & Oil Central Heating . Viewing Essential To Fully Appreciate Cy merwy d pob gof al wrth baratoi’r many lion hy n, ond eu diben y w rhoi arweiniad Ev ery care has been taken with the preparation of these particulars but they are f or cyff redinol y n unig, ac ni ellir gwarantu eu bod y n f anwl gy wir. Cofiwch ofy n os bydd general guidance only and complete accuracy cannot be guaranteed. If there is any unrhy w bwy nt sy ’n neilltuol o bwy sig, neu dy lid ceisio gwiriad proff esiynol. point which is of particular importance please ask or prof essional v erification should Brasamcan y w’r holl ddimensiy nau. Nid y w cyf eiriad at ddarnau gosod a gosodiadau be sought. All dimensions are approximate. The mention of any f ixtures f ittings &/or a/neu gyf arpar y n goly gu eu bod mewn cyf lwr gweithredol eff eithlon. Darperir appliances does not imply they are in f ull eff icient working order. Photographs are ffotograff au er gwy bodaeth gyff redinol, ac ni ellir casglu bod unrhy w eitem a prov ided f or general inf ormation and it cannot be inf erred that any item shown is ddangosir y n gy nwysedig y n y pris gwerthu. -

Gwynedd Archives, Caernarfon Record Office
GB 0219 Penyrorsedd Gwynedd Archives, Caernarfon Record Office This catalogue was digitised by The National Archives as part of the National Register of Archives digitisation project NRA 28851 The National Archives - HAY 1988 NATION^: REGISTER OF ARCHIVES PENYRORSEDD SLATE SPARRY COMPANY RECORDS Caernarvonshiro Record Office 19 7 3 Records deposited by Penyrorsedd Slate Quarry Company Ltd. Catalogued by Mrs. M.A * Aris Senior Assistant Archivist Class Mark t Penyrorsodd INSPECTION OP THESE RECORDS IS SUBJECT TO A 30 YEAR RULE. Contents X FINANCIAL 1-7 Ledgers* 8-15 Cash books. 16-20 Other accounts. II PRODUCTION 21-28 Production account books. 29-38 Other production books. 39 - 51 Stock books. 52-58 Cost books. 59 - 70 Letting lists. 71 - 82 Analysis of costs. 83 - 89 Production and wages sheets III SALES 90 - 98 Order books, etc. 99-103 Price lists. 104 Character book. IV SLATE SHIPMENTS 105 ** 116 Cargo books. V WAGES, ETC. 117 - 150 Time books and wages books. 151 - 154 Other wages books. 155 - 160 Registers of Employees. 161 - 180 National Insurance register 181 - 185 Subsistence analysis books. 186 - 196 Analysis of pay. 197 - 200 Other wages records. VI QUARRY NOTICES 201 - 222 Quarry notices. VII ACCIDENT RECORDS 223 - 270 Accident books* notices of accidents, etc. 271 * 285 Compensation account books 286 ** 290 Other registers. VIII CORRESPONDENCE, ETC. 291 - 328 General correspondence and other papers, 329 * 330 Repairs to farms and cottages. 331 - 362 Rainfall charts. 363 - 366 Medical Club records. 367 - 374 Quarry Union Works Committee records. PLANS 375 - 423 Plans X PHOTOGRAPHS CHS.1245/1-26 Photographs X FINANCIAL 1 - 7 Ledgers! 1. -
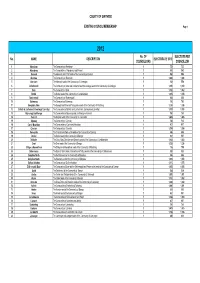
2012 Gwynedd
COUNTY OF GWYNEDD EXISTING COUNCIL MEMBERSHIP Page 1 2012 No. OF ELECTORS PER No. NAME DESCRIPTION ELECTORATE 2012 COUNCILLORS COUNCILLOR 1 Aberdaron The Community of Aberdaron 1 733 733 2 Aberdovey The Communities of Aberdovey and Pennal 1 960 960 3 Abererch The Abererch and Y Ffôr wards of the Community of Llannor 1 998 998 4 Abermaw The Community of Barmouth 1 1,608 1,608 5 Abersoch The Abersoch ward of the Community of Llanengan 1 558 558 6 Arllechwedd The Community of Aber and Llanllechid and the Llandygai ward of the Community of Llandygai 1 1,010 1,010 7 Bala The Community of Bala 1 1,362 1,362 8 Bethel The Bethel ward of the Community of Llanddeiniolen 1 1,015 1,015 9 Bontnewydd The Community of Bontnewydd 1 836 836 10 Botwnnog The Community of Botwnnog 1 700 700 11 Bowydd & Rhiw The Bowydd and Rhiw and Tanygrisiau wards of the Community of Ffestiniog 1 1,218 1,218 12 Brithdir & Llanfachreth/ Ganllwyd/ Llanelltyd The Communities of Brithdir and Llanfachreth, Ganllwyd and Llanelltyd 1 1,103 1,103 13 Bryn-crug/ Llanfihangel The Communities of Bryn-crug and Llanfihangel-y-Pennant 1 761 761 14 Cadnant The Dwyrain ward of the Community of Caernarfon 1 1,405 1,405 15 Clynnog The Community of Clynnog 1 723 723 16 Corris/ Mawddwy The Communities of Corris and Mawddwy 1 917 917 17 Criccieth The Community of Criccieth 1 1,354 1,354 18 Cwm-y-Glo The Ceunant and Cwm-y-Glo wards of the Community of Llanrug 1 696 696 19 Deiniol The Deiniol ward of the Community of Bangor 1 537 537 20 Deiniolen The Clwt y Bont, Deiniolen and Dinorwic wards of -

6 Rhes Ganol, Rhosgadfan, Gwynedd LL54 7HT £129,950
6 Rhes Ganol, Rhosgadfan, Gwynedd LL54 7HT ● £129,950 Excellently presented throughout – it’s ready when you are - so what are you waiting for? . End Terrace House (In A Row Of 3) . Exceptional Views Of Sea & Anglesey . Modernised & With An Attractive Interior . uPVC Double Glazing & LPG Central Heating . 3 Bedrooms & Contemporary Bathroom . Gardens & Off Road Parking For 1 Vehicle . Lounge Fitted With Multi-Fuel Stove . Perfect Investment Or First Time Buy . Dining Room & Modern Hi-Gloss Kitchen . Internal Viewing Highly Recommended Dafydd Hardy Estate Agents Limited for themselves and for the vendor of this property whose agents they are give notice that: (1) These particulars do not constitute any part of an offer or a contract. (2) All statements contained in these particulars are made w ithout responsibility on the part of Dafydd Hardy Estate Agents Limited. (3) None of the statements contained in these particulars are to be relied upon as a statement or representation of fact. (4) Any intending purchaser must satisfy himself/herself by inspection or otherwise as to the correctness of each of the statements contained in these particulars. (5) The vendor does not make or give and neither do Dafydd Hardy Estate Agents Limited nor any person in their employment has any authority to make or give any representation or warranty whatever in relation to this property. (6) Where every attempt has been made to ensure the accuracy of the floorplan contained here, measurements of doors, w indows, rooms and any other items are approximate and no responsibility is taken for any error, omission, or mis-statement. -

Bryn Mafon, Caeathro, Caernarfon, Gwynedd, LL55 2TE Offers in the Region Of
Offers in the Region of: £750,000 Bryn Mafon, Caeathro, Caernarfon, Gwynedd, LL55 2TE EPC Band F Bryn Mafon is a highly individual Countryside Residence situated in a pleasant location on the periphery of the Royal town of Caernarfon, standing in some 3¼ Acres with a tree lined driveway, several enclos ed paddocks with stable block and much more besides whilst scenic views can be WC enjoyed from the first floor over the surrounding countryside, including the mountains of Swimming Pool 7.34m x 13.52m (24'1" x 44'4") Snowdonia. Thought to have been a former farmhouse, Bryn Mafon was extensively enlarged and Changing Room/Sauna 4.52m x 7.33m (14'10" x 24'1") re-modelled in the late 1970s, becoming a substantial, versatile and practical family home with the Car Port 8.35m x 5.66m (27'5" x 18'7") addition of recreational facilities of an indoor heated swimming pool complete with changing Workshop 10.74m x 3.72m (35'3" x 12'2") Please note that the shaded room, sauna and tennis court. The adjoining paddocks appear to offer good grazing and with the Stables stable block and tack room, there’s certainly appeal here if you have equestrian interests or wish area is not included in sale. keep livestock or simply be more self-sufficient. The driveway culminates in a spacious parking and turning area together with a generous car port and useful workshop. There’s a real sense of privacy Accommodation & Amenities here which is welcome whilst being within minutes of Caernarfon, convenient for the A55 · Highly Individual Detached Country Residence expressway, the university city of Bangor and the beauty of both the coast and Snowdonia. -

Bodwyn Farm Caeathro Caernarfon Gwynedd Ll55 2Tg
BODWYN FARM / FFERM BODWYN CAEATHRO CAERNARFON GWYNEDD LL55 2TG 104.23 acres (42.18 hectares) or thereabouts of land including a substantial character residence with garden grounds and a walled garden together with some traditional farm buildings Available to let as a whole on a 6 year Farm Business Tenancy agreement, commencing on 1st May 2015 Particulars prepared in April 2015 The Tenant will be allowed to declare the land on his Single Application Form (SAF) 2015 in order to receive an allocation of Basic Payment Scheme (BPS) entitlements as well as putting the land forward for the Glastir schemes, if desired Tenders to be in hand no later than 12 noon on 27th April 2015 For further details, please contact Sion Wyn Jones MRICS Menai Bridge: (01248) 362524 e-mail: [email protected] Oddeutu 104.23 erw (42.18 hectar) o dir, yn cynnwys tŷ sylweddol hanesyddol gyda gerddi helaeth a gardd o fewn wal, ynghyd a rhai adeiladau fferm traddodiadol Ar gael i’w osod yn gyfan ar Gytundeb Tenantiaeth Busnes Fferm i gychwyn ar y 1af o Fai 2015 Bydd modd i’r tenant gynnwys y tir ar ei Ffurflen Taliad Fferm Sengl (SAF) 2015 ar gyfer hawlio cyfran o Gynllun y Taliad Sylfaenol (BPS) yn ogystal a cynnig y tir ar gyfer Cynllun Glasdir, os yw’n dymuno Cynnigion i law dim hwyrach na hanner dydd, Ebrill 27, 2015 I dderbyn manylion pellach cysylltwch a Sion Wyn Jones MRICS Menai Bridge: (01248) 362524 e-mail: [email protected] Particulars prepared in April 2015 INTRODUCTION / CYFLWYNIAD Bodwyn Farm is a useful lowland holding, which comprises of 104.23 acres (42.18 hectares) or thereabouts of land including a substantial character residence with garden grounds and a walled garden together with some traditional farm buildings. -

Communities First Alysarn & Antlle N Ew Sletter
Cylchlythyr Talysarn a Nantlle Hydref 2011_Cylchlythyr Talysarn a Nantlle 11/10/2011 10:45 Page 5 Talysarn & Nantlle Communities First Partnership Partnership News Autumn 2011 Give it a Go Day On one of the hottest days we had r this summer, we held a ‘Give it a go’ e day here in the Community Centre in t Talysarn. The purpose of the day was t to raise awareness of the different e types of training that’s available. l During the day there was an s opportunity to have a go at different w courses such as green woodworking, genealogy, flower arranging, sewing e and much more. There was also wide range of information on other courses N that are available by local training e l providers. In addition there were activities for l the children such as bouncy castle, games, t face painting, etc. n Several individuals have put their names down a for courses such as Green Woodworking and Genealogy. Arrangements are now being made N to start a Green Woodworking Course, Genealogy and Cooking courses. & n r a s If you’d like to put your name y down for any of the above l courses, or you’d like to do a something else, contact us here at the office. T Canolfan Talysarn, Ffordd yr Orsaf, Talysarn, CAERNARFON, Gwynedd LL54 6HL 01286 881103 [email protected] Llywodraeth Cynulliad Cymru communities first cymunedau yn gyntaf Welsh Assembly Government Cylchlythyr Talysarn a Nantlle Hydref 2011_Cylchlythyr Talysarn a Nantlle 11/10/2011 10:45 Page 6 Young People Sustainable Energy Project Bike Restoration Thanks to the Police we First there was the Energy Awareness Day when received 10 bikes so that the young people could numbers of people from the community saw complete a bike restoration course with Dewi, projects, watched films, listened to speakers and Cycle Wales, who’s based at one of the units in signed up for free energy-saving gadgets.