('Ct-3')(2011/C 172/01
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Serious Adverse Event Reporting in Investigator-Initiated Clinical Trials
For debate Serious adverse event reporting in investigator-initiated clinical trials “Commonly ew drugs and medical devices offer improve- Summary ments in health care. Clinical research is under- reported SAEs Reporting adverse events (AEs) and serious AEs taken to elucidate such benefits, but also to N (SAEs) are practical steps to ensure safety for should be identify potential harms. Adverse event (AE) and serious volunteers and patients in medical research involving adopted as AE (SAE) data are crucial information in drug and device medications, treatments and devices. However, the fi universal development studies (Box 1). De nitions and re- burden and cost of reporting should be proportionate quirements for safety reporting in Australia are outlined with the public health benefit of this information. 1 endpoints to be by the international guidelines, and the National Health Unfortunately, in Australia there is clear evidence of mandated in all and Medical Research Council (NHMRC) National state- ever-increasing requirements from sponsors and ment on ethical conduct in human research 2 ethics committees to report AEs and SAEs unnec- Phase IV clinical . Further, the NHMRC has provided clarification on how AEs should essarily, leading to a decrease in the uptake of trials” be reported and who has responsibility for reviewing and research, particularly less well funded investigator- acting on them.3 Such guidelines are practical steps to initiated trials. ensure safety for participants in all research involving We believe that individual AE reports to ethics interventions, including post-marketing surveillance and committees serve no useful purpose, because in most cases the study group identity (drug exposure) Phase IV trials (Box 2) of approved medicines, treatments is not known in studies with blinded treatment arms and devices. -

Serious Adverse Events and Suspected Unexpected Adverse Events
Adverse Events/Adverse Reactions/Serious Adverse Reactions/ Serious Adverse Events and Suspected Unexpected Adverse Events SOP Title AE/AR/SAE/SAR/SUSAR SOP No. SOP 3 Author Julia Farmery Consulted Departments Lincolnshire Clinical Trials Unit, Research and Development, Trust consultants and research staff. Lead Manager Dr. Tanweer Ahmed Director of LCRF and Sign and Print Name Research and Development Manager Version 2 Current version published 21.07.2011 Review date of SOP 21.07.2013 Version 1 (10.03.2010) Superseded. (Changes Superseded on 21.07.2011 detailed on index of SOP) Tracked Changes to SOP 3 – Adverse Events/Serious Adverse Events and Suspected Unexpected Adverse Events Paragraph Changes 1 - Purpose Detailed information of what the SOP is for and how staff should deal with this. It sets out the principles by AE/AR SAE/SAR/SUSARS will be recorded and methods by which they are categorised. It has detailed instructions that are to be followed that are in line with statutory law and regulations. 2 - Adverse Included Medicine for Human Use Regulation at the Events beginning. Added a detailed explanation about AR, ADR. More detail on what determines an event as a SAE, SAR and SUSAR. Included Medicines for Human Use (Clinical Trials) Regulations (2004) 3 - SUSAR Replaced definition with UK Clinical Trials Regulations with Medicines for Human Use (Clinical Trials) Regulations A brief explanation of what a SUSAR is. Replaced adverse events with reactions 4 - IMP 5 - NIMP 6 - SOP title SOP applies to all staff within ULHT. SOP defines responsibilities for trials sponsored and hosted by ULHT. -

FDA Guidance for Clinical Trial Sponsors
Guidance for Clinical Trial Sponsors Establishment and Operation of Clinical Trial Data Monitoring Committees For questions on the content of this guidance, contact the Office of Communication, Training, and Manufacturers Assistance (CBER) at 800-835-4709 or 301-827-1800. U.S. Department of Health and Human Services Food and Drug Administration Center for Biologics Evaluation and Research (CBER) Center for Drug Evaluation and Research (CDER) Center for Devices and Radiological Health (CDRH) March 2006 OMB Control No. 0910-0581 Expiration Date: 10/31/2021 See additional PRA statement in Section 8 of this guidance Contains Nonbinding Recommendations Guidance for Clinical Trial Sponsors Establishment and Operation of Clinical Trial Data Monitoring Committees Additional copies of this guidance are available from: Office of Communication, Training and Manufacturers Assistance, HFM-40 Center for Biologics Evaluation and Research Food and Drug Administration 1401 Rockville Pike, Rockville, MD 20852-1448 Phone: 800-835-4709 or 301-827-1800 Internet: http://www.fda.gov/cber/guidelines.htm or Office of Training and Communication Division of Communications Management Drug Information Branch, HFD-210 Center for Drug Evaluation and Research Food and Drug Administration 5600 Fishers Lane, Rockville, MD 20857 Phone: 301-827-4573 Internet: http://www.fda.gov/cder/guidance/index.htm or The Division of Small Manufacturers, International, and Consumer Assistance (DSMICA) Center for Devices and Radiological Health Food and Drug Administration 1350 Piccard Drive, Rockville, MD 20850 Phone: 800-638-2041 or 301-443-6597 Internet: http://www.fda.gov/cdrh Email: [email protected] Facts-on-Demand (faxback): 800-899-0381 or 301-827-0111 Contains Nonbinding Recommendations Table of Contents 1. -

KLH-21-Version7.Pdf, File Type
KLH-21 version 6 Reporting Adverse Reactions to Medicinal Products for Human Use in a Clinical Trial and to Medicinal Products without Marketing Authorisation. With effect as of 1 December 2016, this guideline supersedes guideline KLH-21, version 5. This guideline defines the procedure for reporting suspected unexpected serious adverse reactions (“SUSAR”) to medicinal products used in clinical trials reported/permitted pursuant to Section 55(4) and (5) of Act No. 378/2007 Coll. on Pharmaceuticals and on Amendments to Some Related Acts (Act on Pharmaceuticals), as amended. The guideline is intended for the sponsors, investigators and persons cooperating with them within the clinical trial, for holders of registration decisions, if they participate in implementation of clinical trials. The purpose of prompt reports of suspected serious unexpected adverse reactions in clinical trials is to feed new and important information into the pharmacovigilance system of clinical trials that ensures timely identification of signals, which can represent a health risk to the included subjects or possibly may result in a change of the safety profile of the investigational medicinal product (the risk outweighs the potential benefit). The functional pharmacovigilance system also allows for evaluating identified serious signals and, if necessary, for taking measures to minimise the risk associated with the use of the investigational medicinal products for the subjects participating in the trial, including ensuring that all the parties involved (sponsors, investigators, participating subjects, regulatory bodies and members of ethics committees) are informed in timely manner. The guideline defines the “reporting obligation” of all those who are involved in the system, the scope of such obligations and the manner of performing such obligations (see the overview table at the end of this guideline). -

Management of Safety Information from Clinical Trials
CIOMS Management of Safety Information from Clinical Trials CIOMS Management of Safety Information from CIOMS publications may be obtained directly from CIOMS, c/o World Health Organization, Avenue Appia, 1211 Geneva 27, Management of Switzerland or by e-mail to [email protected] Both CIOMS and WHO publications are distributed by the Safety Information World Health Organization, Marketing and Dissemination, Avenue Appia, 1211 Geneva 27, Switzerland and are available from Clinical Trials from booksellers through the network of WHO sales agents. A list of these agents may be obtained from WHO by writing to the above address. Report of CIOMS Working Group VI Price: CHF 40.– Geneva 2005 GGROUP6_COVERROUP6_COVER DDEF.inddEF.indd 1 77.8.2007.8.2007 112:17:502:17:50 Management of Safety Information from Clinical Trials Report of CIOMS Working Group VI Geneva 2005 ggroup6_PH.inddroup6_PH.indd 1 77.8.2007.8.2007 112:19:132:19:13 Copyright © 2005 by the Council for International Organizations of Medical Sciences (CIOMS) ISBN 92 9036 079 8 ggroup6_PH.inddroup6_PH.indd 2 77.8.2007.8.2007 112:19:152:19:15 Acknowledgements he Council for International Organizations of Medical Sciences (CIOMS) T gratefully acknowledges the contributions of the members of CIOMS Working Group VI on the Management of Safety Information from Clinical Trials as well as the drug regulatory authorities, pharmaceutical companies and other organizations and institutions which supported the work that resulted in this publication. Hard work, drafting and redrafting of papers, their reviews and a number of debates in the Working Group required patience, motivation and active collaboration from all members. -

Clinical Trials Directive
L 121/34 EN Official Journal of the European Communities 1.5.2001 DIRECTIVE 2001/20/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 4 April 2001 on the approximation of the laws, regulations and administrative provisions of the Member States relating to the implementation of good clinical practice in the conduct of clinical trials on medicinal products for human use THE EUROPEAN PARLIAMENT AND THE COUNCIL OF THE (3) Persons who are incapable of giving legal consent to EUROPEAN UNION, clinical trials should be given special protection. It is incumbent on the Member States to lay down rules to this effect. Such persons may not be included in clinical Having regard to the Treaty establishing the European trials if the same results can be obtained using persons Community, and in particular Article 95 thereof, capable of giving consent. Normally these persons should be included in clinical trials only when there are grounds for expecting that the administering of the Having regard to the proposal from the Commission (1), medicinal product would be of direct benefit to the patient, thereby outweighing the risks. However, there is a need for clinical trials involving children to improve Having regard to the opinion of the Economic and Social the treatment available to them. Children represent a Committee (2), vulnerable population with developmental, physiological and psychological differences from adults, which make age- and development- related research important for Acting in accordance with the procedure laid down in Article their benefit. Medicinal products, including vaccines, for 251 of the Treaty (3), children need to be tested scientifically before wide- spread use. -

1 SPONSOR: UZ Leuven Eudract NUMBER: 2016-004859-77 DATE
SPONSOR: UZ Leuven TITLE: Effect of pembrolizumab (Keytruda®) on biomarkers related to intratumoral immunity, proliferation and apoptosis in early breast cancer. EudraCT NUMBER: 2016-004859-77 DATE: July 17, 2018 Principal investigator Prof. Dr. Ann Smeets Investigators: Prof. Dr. Ines Nevelsteen and Prof. Dr. Hans Wildiers Signature Principal investigator: 1 TABLE OF CONTENTS 1.0 TRIAL SUMMARY.................................................................................................... 6 2.0 TRIAL DESIGN.......................................................................................................... 6 2.1 Trial Design : ........................................................................................................... 6 2.2 Trial Diagram phase 0 trial .................................................................................... 7 3.0 OBJECTIVES & HYPOTHESeS .............................................................................. 8 3.1 Primary Objective & Hypothesis .......................................................................... 8 3.2 Secondary Objectives & Hypotheses ..................................................................... 8 4.0 BACKGROUND & RATIONALE .......................................................................... 10 4.1 Background ........................................................................................................... 10 4.1.1 Early breast cancer .............................................................................................. 10 4.1.2 -

Workstream 6: Pharmacovigilance 1.0 Introduction
MRC/DH joint project to codify good practice in publicly-funded UK clinical trials with medicines Workstream 6: Pharmacovigilance 1.0 Introduction.......................................................................................................... 2 1.1 Background................................................................................................ 2 1.2 Definitions.................................................................................................. 3 2.0 Definition of Sponsor for Pharmacovigilance................................................... 4 3.0 General Considerations: Risk Adapted Approaches to Safety Reporting 4 4.0 Adverse Events: - Investigator Responsibilities............................................... 5 5.0 Assessment of Adverse Events.......................................................................... 5 5.1 Assessment of Seriousness........................................................................ 5 5.2 Assessment of Causality............................................................................. 6 5.3 Assessment of Expectedness..................................................................... 6 5.4 Assessment of Adverse Events: Responsibilities......................................... 6 5.5 Assessment of Adverse Events in Blinded Trials........................................ 7 6.0 Adverse Events: - Sponsor Responsibilities...................................................... 8 6.1 Expedited Reporting to Competent Authorities.......................................... -
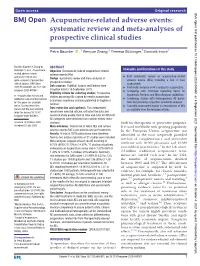
Acupuncture- Related Adverse Events: Systematic Review and Meta
Open access Original research BMJ Open: first published as 10.1136/bmjopen-2020-045961 on 6 September 2021. Downloaded from Acupuncture-related adverse events: systematic review and meta- analyses of prospective clinical studies Petra Bäumler ,1 Wenyue Zhang,2 Theresa Stübinger,1 Dominik Irnich1 To cite: Bäumler P, Zhang W, ABSTRACT Strengths and limitations of this study Stübinger T, et al. Acupuncture- Objective Overview on risks of acupuncture- related related adverse events: adverse events (AEs). ► First systematic review on acupuncture- related systematic review and Design Systematic review and meta- analyses of meta- analyses of prospective adverse events (AEs) including a risk of bias prospective studies. clinical studies. BMJ Open assessment. Data sources PubMed, Scopus and Embase from 2021;11:e045961. doi:10.1136/ ► First meta- analyses on AEs related to acupuncture. inception date to 15 September 2019. bmjopen-2020-045961 ► Complying with Preferred Reporting Items for Eligibility criteria for selecting studies Prospective Systematic Reviews and Meta- Analyses guidelines. ► Prepublication history and studies assessing AEs caused by needle acupuncture ► Combining studies with heterogeneous AE defini- additional supplemental material in humans as primary outcome published in English or for this paper are available tions but providing respective sensitivity analyses. German. online. To view these files, ► Causality assessment based on descriptions of AEs Data extraction and synthesis Two independent please visit the journal online. as available from the included articles. (http:// dx. doi. org/ 10. 1136/ researchers selected articles, extracted the data and bmjopen- 2020- 045961). assessed study quality. Overall risks and risks for different AE categories were obtained from random effects meta- Received 16 October 2020 analyses. -
Study Protocol
CLINICAL TRIAL PROTOCOL Code: SAINT Title of trial: Pilot study to evaluate the potential of ivermectin to reduce COVID-19 transmission Phase: IIa Date of protocol: 12 of August 2020 - Version 2.0 EudraCT number: 2020-001474-29 Sponsor: Clínica Universidad de Navarra Written by: Carlos Chaccour MD PhD Principal Investigator: Dr. Carlos Chaccour Department: División of Infectious Diseases Clínica Universidad de Navarra CONFIDENTIAL MAY NOT BE USED, DIVULGED OR PUBLISHED WITHOUT TRIAL SPONSOR'S CONSENT. Sponsor: Clínica Universidad de Navarra EUDRACT No.: 2020-001474-29 Protocol: SAINT PROTOCOL SIGNATURES SHEET Protocol: Pilot study to evaluate the potential of ivermectin to reduce COVID-19 transmission I have read this protocol and accept the obligation to direct this trial in accordance with all the stipulations of the protocol and with the Helsinki Declaration. Dr. Carlos Chaccour 12 agosto 2020 Principal investigator/ Signature Date trial coordinator Dr. Enrique Aubá Guedea 12 agosto 2020 Deputy Chief Medical Officer Sponsor's Signature Date Clínica Universidad de Navarra Version 2.0 - 12 of August 2020 Page 2 of 48 Sponsor: Clínica Universidad de Navarra EUDRACT No.: 2020-001474-29 Protocol: SAINT CONTENTS 1. GENERAL INFORMATION ....................................................................................................... 7 1.1. Identification of trial .................................................................................................... 7 1.2. Details of sponsor ....................................................................................................... -
Data and Safety Monitoring Guidance
DATA AND SAFETY MONITORING GUIDANCE Harvard Catalyst | The Clinical and Translation Science Center Regulatory Foundations, Ethics, and Law Program Updated 14JUL2020 SECTION ONE: OVERVIEW OF DATA AND SAFETY MONITORING 1 SECTION TWO: DATA AND SAFETY MONITORING FOR CLINICAL TRIALS 5 SECTION THREE: DATA AND SAFETY MONITORING PLANS (DSMPS) 4 SECTION FOUR: DATA AND SAFETY MONITORING BOARDS (DSMBS) 8 FREQUENTLY ASKED QUESTIONS 17 ATTRIBUTION, SHARING, AND ADAPTING THE TRAINING GUIDANCE 19 DSMB/P TEMPLATES AND EXAMPLES 20 ACKNOWLEDGEMENTS 21 CONTACT US 22 RESOURCES 23 APPENDIX A: PRINCIPAL INVESTIGATOR’S RESPONSIBILITIES 26 APPENDIX B: INDEPENDENT MONITORS/MONITORING GROUP 29 APPENDIX C: DSMP TEMPLATE 30 APPENDIX D: DSMB TEMPLATE 34 Updated 14JUL2020 Section One: Overview of Data and Safety Monitoring1 Background A clinical trial depends upon a relationship between research participants and investigators; each must fulfill certain obligations for the effort to succeed. A clinical trial also relies upon a partnership between investigator and institution/sponsor; together they must ensure proper monitoring and conduct of the clinical trial, in accordance with applicable regulations and Good Clinical Practice (GCP). To ensure the safety of research participants, federal regulations require provisions to monitor data collected in the course of a research study, where appropriate (see 45 CFR 46.111(a)(6); 21 CFR 56.111(a)(6)). Data and safety monitoring aims both to protect participants and ensure the integrity and validity of research data. All studies involving human subjects require some level of data and safety monitoring. This includes physiologic, toxicity, and dose-finding studies (phase I); efficacy studies (phase II); and efficacy, effectiveness, and comparative trials (phase III).