UC Irvine UC Irvine Previously Published Works
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Applications of Laser Spectroscopy Constitute a Vast Field, Which Is Difficult to Spectroscopy Cover Comprehensively in a Review
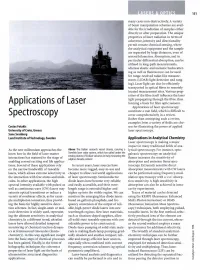
LASERS & OPTICS 151 many cases non-destructively. A variety of beam manipulation schemes are avail able for the irradiation of samples either directly or after preparation. The unique properties of laser radiation in terms of coherence, intensity and directionality permit remote chemical sensing, where the analytical equipment and the sample are separated by large distances, even of several kilometres. Absorption, and in particular differential absorption, can be utilised in long-path measurements, whereas elastic and inelastic backscatter- ing as well as fluorescence can be used for range-resolved radar-like measure ments (LIDAR: light detection and rang ing). Laser light can also be efficiently transported in optical fibres to remotely located measurement sites. Various prop erties of the fibre itself influence the laser light propagating through the fibre, thus Applications of Laser forming a basis for fibre optic sensors. Applications of laser spectroscopy constitute a vast field, which is difficult to Spectroscopy cover comprehensively in a review. Rather than attempting such a review, examples from a variety of fields are cho Costas Fotakis sen for illustrating the power of applied University of Crete, Greece laser spectroscopy. Sune Svanberg Lund Institute of Technology, Sweden Applications in Analytical Chemistry Laser spectroscopy is making a major impact in many traditional fields of ana As the new millennium approaches the Above The Italian research vessel Urania, carrying a lytical spectroscopy. For instance, opto- know how in the field of laser-matter Swedish laser radar system, which has sailed under the galvanic spectroscopy on analytical smoky plumes of Sicilian volcanos in Italy measuring the interactions has matured to the stage of sulphur dioxide content flames increases the sensitivity of enabling several exciting real life applica absorption and emission flame spec tions. -

American Society for Laser Medicine and Surgery Abstracts 1 AMERICAN SOCIETY for LASER MEDICINE and SURGERY
American Society for Laser Medicine and Surgery Abstracts 1 AMERICAN SOCIETY FOR LASER MEDICINE AND SURGERY ABSTRACTS Conclusion: These initial data suggest that AFxL pre-treatment CUTANEOUS LASER is likely to enhance the uptake of IngMeb in the skin. This might enable treatment of hyperkeratotic lesions as well as increase SURGERY overall efficacy when treating AK’s with IngMeb. #2 #1 SPLIT FACE COMPARISON OF THE EFFECTS OF FRACTIONAL LASER-MEDIATED DELIVERY OF VITAMIN CE FERULIC FORMULA SERUM TO INGENOL MEBUTATE - PRELIMINARY RESULTS DECREASE POST-OPERATIVE RECOVERY AND FROM AN IN VITRO FRANZ CELL STUDY INCREASE NEOCOLLAGENOSIS IN FRACTIONAL Andre´s M. Erlendsson, Elisabeth H. Taudorf, ABLATIVE LASER RESURFACING FOR Andre´ H. Eriksson, John R. Zibert, Uwe Paasch, PHOTODAMAGE R. Rox Anderson, Merete Haedersdal Jill Waibel, Adam Wulkan Bispebjerg Hospital, University of Copenhagen, Copenhagen, Miami Dermatology & Laser Institution, Miami, FL; Denmark; LEO Pharma A/S, Ballerup, Denmark; University of Miami University, Miami, FL Leipzig, Leipzig, Germany; Wellman Center for Photomedicine, Background: New fractional ablative laser skin resurfacing is Massachusetts General Hospital, Harvard Medical School, associated with shorter periods of recovery time in comparison Boston, MA with older ablative technology. However one deterrent is the Background: Ingenol Mebutate gel (IngMeb) is a new FDA seven days of downtime associated with the procedure. Previous approved field directed treatment against Actinic Keratosis (AK). studies have shown that application of vitamin C, E and ferulic A recent study on clinically typical AK’s showed complete acid improves wound healing and promotes the induction of clearance rates of 34% for trunk and extremities, and 42% for face collagen. -

Footprints in Laser Medicine and Surgery: Beginnings, Present, and Future
Review Article Med Laser 2017;6(1):1-4 Review Article https://doi.org/10.25289/ML.2017.6.1.1 pISSN 2287-8300ㆍeISSN 2288-0224 Footprints in Laser Medicine and Surgery: Beginnings, Present, and Future Ki Uk Song Light-based science and technology has been evolving throughout history. One of the most significant advances in light-based science and technology is the laser. Early in its development, the laser offered Brighlans, Inc., Manila, Philippines physically unique and attractive characteristics with much potential to solve the conditions of medicine and surgery, opening many gateways for laser applicability through research by renowned physicians. In collaboration with physicians, the medical industry has continued to develop better and more efficient technological advancements. The laser has now become one of the most advanced medical solutions for a variety clinical cases. Moreover, there are some procedures for which the laser is now mandatory. Despite many challenges that still lie ahead, practitioners and patients alike are thrilled to see even more exciting progress in the fast-expanding field of laser medicine and surgery. Key words Laser; History; Selective photothermolysis; Scanning technology; Fractionated laser Received May 12, 2017 Revised June 6, 2017 Accepted June 6, 2017 Correspondence Ki Uk Song Brighlans, Inc., Heritage Tower, #1851 Vasquez Street, Malate, Manila, Philippines Tel.: +63-2-521-0441 Fax: +63-2-521-0441 E-mail: [email protected] C Korean Society for Laser Medicine and Surgery CC This is an open access article distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/ licenses/by-nc/4.0) which permits unrestricted non- commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. -

Evaluation of Stimulated Raman Scattering Microscopy for Identifying Squamous Cell Carcinoma in Human Skin
Lasers in Surgery and Medicine 45:496–502 (2013) Evaluation of Stimulated Raman Scattering Microscopy for Identifying Squamous Cell Carcinoma in Human Skin 1,2 1 1 1,3 4 Richa Mittal, MS, Mihaela Balu, PhD, Tatiana Krasieva, PhD, Eric O. Potma, PhD, Laila Elkeeb, MD, 4 1Ã Christopher B. Zachary, MBBS, FRCP, and Petra Wilder-Smith, DDS, PhD 1Beckman Laser Institute and Medical Clinic, University of California, Irvine, California 92612 2Department of Chemical Engineering and Materials Sciences, University of California, Irvine, California 92697 3Department of Chemistry, University of California, Irvine, California 92697 4Department of Dermatology, University of California, Irvine, California 92697 Background and Significance: There is a need to uncontrolled growth of epithelial keratinocytes. It is develop non-invasive diagnostic tools to achieve early and estimated that 700,000 cases of SCC are diagnosed accurate detection of skin cancer in a non-surgical manner. annually in the US, resulting in approximately 2,500 In this study, we evaluate the capability of stimulated deaths [2,3]. Although most of the non-melanoma skin Raman scattering (SRS) microscopy, a potentially non- cancer cases can be cured, rising incidence and local invasive optical imaging technique, for identifying the invasiveness constitute an important clinical challenge. pathological features of s squamous cell carcinoma (SCC) Today, non-melanoma skin cancer is diagnosed by visual tissue. inspection followed by invasive skin biopsy and histopath- Study design: We studied ex vivo SCC and healthy skin logical examination. Patients with SCC are at an increased tissues using SRS microscopy, and compared the SRS risk of future SCC tumor development, especially in the contrast with the contrast obtained in reflectance confocal same location or surrounding tissue. -

Application of Two-Photon Absorbing Fluorene-Containing Compounds in Bioimaging and Photodyanimc Therapy
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2014 Application of Two-Photon Absorbing Fluorene-Containing Compounds in Bioimaging and Photodyanimc Therapy Xiling Yue University of Central Florida Part of the Chemistry Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Doctoral Dissertation (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Yue, Xiling, "Application of Two-Photon Absorbing Fluorene-Containing Compounds in Bioimaging and Photodyanimc Therapy" (2014). Electronic Theses and Dissertations, 2004-2019. 4634. https://stars.library.ucf.edu/etd/4634 APPLICATION OF TWO-PHOTON ABSORBING FLUORENE- CONTAINING COMPOUNDS IN BIOIMAGING AND PHOTODYNAMIC THERAPY by XILING YUE B. S. Fudan University, 2009 A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Chemistry in the College of Science at the University of Central Florida Orlando, Florida Fall Term 2014 Major Professor: Kevin D. Belfield ABSTRACT Two-photon absorbing (2PA) materials has been widely studied for their highly localized excitation and nonlinear excitation efficiency. Application of 2PA materials includes fluorescence imaging, microfabrication, 3D data storage, photodynamic therapy, etc. Many materials have good 2PA photophysical properties, among which, the fluorenyl structure and its derivatives have attracted attention with their high 2PA cross-section and high fluorescence quantum yield. Herein, several compounds with 2PA properties are discussed. -

Lasers in Skin Cancer Treatment Podcast Audio Transcription
Lasers in Skin Cancer Treatment Podcast Audio Transcription Opening Welcome to Light Talk. A podcast series exclusively for members of the American Society for Laser Medicine and Surgery. Light Talk supports the mission of ASLMS which is to promote excellence in patient care by advancing biomedical application of lasers and other energy-based technologies world-wide. We hope you enjoy this edition of Light Talk with our host, Dr. Nazanin Saedi. Discussion DR. NAZANIN SAEDI Hi, I’m Nazanin Saedi and I am here today with Dr. Anthony Rossi who is an assistant attending at Memorial Sloan Kettering Cancer Center. Anthony, thank you so much for joining us. DR. ANTHONY M. ROSSI Thanks for having me. DR. SAEDI So, Anthony, can you tell us a little bit about your research in using lasers to treat skin cancers? We often think of surgical options for our skin cancer patients, but how do lasers play a role? DR. ROSSI Sure so, you know, for certain patients who have early skin cancers like early superficial basal cell carcinomas, or squamous cell carcinoma in situ, some of these can be amenable to be treated with lasers instead of your traditional surgical approach. So, it’s really important to understand which ones to select and which ones not to treat. Right? We don’t want to treat very deep invasive, infiltrative basal cell with a very superficial laser because we will be missing the deeper component. But for these early lesions, and for patients who don’t necessarily want to have surgery, treating them with a CO2 laser which is what I have been doing, guided by confocal microscopy can really help us hone in on the areas that are positive and then ablate that tissue and then, which is really important, is follow up with them to make sure they aren’t having any regrowth. -

The American Society for Laser Medicine and Surgery, Inc
ASLMS Fact Sheet WHAT IS ASLMS? The American Society for Laser Medicine and Surgery, Inc. (ASLMS) was founded in 1980 and is the world’s largest professional organization dedicated to promoting excellence in patient care by advancing laser applications and other energy based technologies. WHO BELONGS TO ASLMS? Membership includes physicians and surgeons representing diverse medical specialties, nurses and allied health care professionals, scientists involved with product development, biomedical engineers, biologists, industry leaders and equipment manufacturers. ASLMS offers students, residents, fellows and PhD candidates free membership for the duration of their training, waives the annual conference registration fee and offers reduced course fees for them as well. HOW MANY MEMBERS DOES ASLMS HAVE? The Society currently has more than 3,200 members. Nearly 20% are located outside the United States. WHAT DOES ASLMS DO? The vision of ASLMS is to be the world’s preeminent resource for laser research, education, technology and clinical knowledge. The mission of ASLMS is to promote excellence in patient care by advancing biomedical application of lasers and other related technologies worldwide. ASLMS works toward this ambitious mission by: • Conducting an annual conference for the multidisciplinary exchange of information on the latest discoveries, applications and research involving medical lasers and light energy sources • Publishing the world’s foremost laser journal, Lasers in Surgery and Medicine aslms-fact-sheet pg. 1 • Raising more than $1 million in the past five years for applied medical laser and related light energy technology research projects and grants • Establishing practice guidelines and safety standards for physician and non- physician use of lasers and related light-based technologies • Providing in-service education and testifying before regulatory authorities, including the U.S. -

Meeting Materials
BUSINESS, CONSUMER SERVICES, AND HOUSING AGENCY EDMUND G. BROWN JR., GOVERNOR STATE BOARD OF OPTOMETRY 2450 DEL PASO ROAD, SUITE 105, SACRAMENTO, CA 95834 P (916) 575-7170 F (916) 575-7292 www.optometry .ca.gov Continuing Education Course Approval Checklist Title: Provider Name: ☐Completed Application Open to all Optometrists? ☐ Yes ☐No Maintain Record Agreement? ☐ Yes ☐No ☐Correct Application Fee ☐Detailed Course Summary ☐Detailed Course Outline ☐PowerPoint and/or other Presentation Materials ☐Advertising (optional) ☐CV for EACH Course Instructor ☐License Verification for Each Course Instructor Disciplinary History? ☐ Yes ☐No 1 2 NVISION ORGANIZATION Providers List with NPI And Medical License #'s Medical CE dic Center Doctor License # Degree Phone Email Address Provider? State Personal NPI # are Torrance Amarprett Brar, M.D. A77993 MD 310‐714‐7494 amar.brar@nvisionce Yes CA 1356361109 Y Fullerton Franklin Lusby, M.D. G41830 MD 858‐449‐9867 [email protected] Yes CA Need NPI # N Torrance Franklin Lusby, M.D. G41830 MD 858‐449‐9867 [email protected] Yes CA Need NPI # N Laguna Hills George Baerveldt, M.D. A39678 MD Newport george.baerveldt@nv Yes CA 1316027493 y San Francisco George V Simon M.D. G23786 MD Concord Yes CA 1225251697 San Francisco Jeffery Machat, M.D. C139286 MD San Francisco Jeff.Machat@nvision Yes CA 1255790085 Camarillo John Davidson, M.D. G71316 MD Camarillo doctorjohn@johndav Yes CA 1205870748 Y Ontario Jonathan R. Pirnazar A72632 MD Laguna Hills [email protected] Yes CA 1962436410 Y Laguna Hills Jonathan R. Pirnazar, M.D. A72632 MD Laguna Hills [email protected] Yes CA 1962436410 Y La Jolla Mihir Parikh, M.D. -
Applications of Laser Spectroscopy Svanberg, Sune
Applications of Laser Spectroscopy Svanberg, Sune 1998 Link to publication Citation for published version (APA): Svanberg, S. (1998). Applications of Laser Spectroscopy. (Lund Reports in Atomic Physics; Vol. LRAP-234). Atomic Physics, Department of Physics, Lund University. Total number of authors: 1 General rights Unless other specific re-use rights are stated the following general rights apply: Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal Read more about Creative commons licenses: https://creativecommons.org/licenses/ Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. LUND UNIVERSITY PO Box 117 221 00 Lund +46 46-222 00 00 Europhysics News Manuscript, April 26) Applications of Laser Spectroscopy Sune Svanberg Lund Laser Centre, Lund University and Division of Atomic Physics, Lund Institute of Technology P.O. Box 118, S-221 00 Lund, Sweden Introduction Laser radiation is finding many applications for analysis and diagnostics based on the wavelength dependent interaction between electromagnetic radiation and matter. -

Laser Medicine and Biomedical Optical Imaging
Chapter 13. Laser Medicine and Biomedical Optical Imaging Laser Medicine and Biomedical Optical Imaging RLE Groups Optics and Quantum Electronics Group Academic Staff Professor James G. Fujimoto Research Staff and Visiting Scientists Dr. Yu Chen, Dr. Iwona Gorczynska, Dr. Robert Huber (Ludwig Maximilians University, Munich, Germany) Scientific Collaborators Dr. Peter M. Andrews (Georgetown University), Dr. David Boas (Massachusetts General Hospital), Dr. Sven Bursell (Joslin Diabetes Center), Alex Cable (Thorlabs, Inc.), Royce Chen (New England Eye Center), Dr. Alan Clermont (Joslin Diabetes Center), Dr. James Connolly (Beth Israel Deaconess Medical Center), Dr. Anna Devor (Massachusetts General Hospital), Dr. Jay Duker (New England Eye Center), Dr. Edward Feener (Joslin Diabetes Center), Dr. James Jiang (Thorlabs, Inc.), Dr. Hiroshi Mashimo (Veteran’s Administration Boston Medical Center), Brian Monson (New England Eye Center), Lana Ruvinskaya (Massachusetts General Hospital), Dr. Joseph Schmitt (LightLab Imaging), Dr. Joel Schuman (University of Pittsburgh Medical Center) Graduate Students Desmond C. Adler, Aaron D. Aguirre, Shu-Wei Huang, Jonathan J. Liu, Vivek J. Srinivasan Technical and Support Staff Dorothy A. Fleischer, Donna L. Gale Research Areas and Projects 1. Optical coherence tomography (OCT) technology 1.1 Ultrahigh resolution OCT 1.2 High speed OCT using Fourier domain detection 1.2.1 Spectral domain OCT 1.2.2 Swept source OCT imaging 2. Ophthalmic OCT 2.1 Technology for clinical ophthalmic OCT 2.2 Ultrahigh resolution OCT study of retinal pathologies 2.3 Three-dimensional visualization methods for ophthalmic imaging 2.4 Small animal retinal imaging 2.5 Swept source/Fourier domain OCT retinal imaging 3. Optical Biopsy using OCT 3.1 Ultrahigh-speed 3D endomicroscopy 3.2 Endoscopic imaging of Barrett’s esophagus 3.3 OCT imaging of kidney microanatomy ex vivo 4. -

The Applications of Laser Spectroscopy in Analytical
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 2002 The pplica ations of laser spectroscopy in analytical chemistry and biochemistry: investigating the photophysics of hypericin and hypocrellin, as well as the structure of porcine fructose-1,6-bisphosphatase Jin Wen Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Analytical Chemistry Commons Recommended Citation Wen, Jin, "The ppa lications of laser spectroscopy in analytical chemistry and biochemistry: investigating the photophysics of hypericin and hypocrellin, as well as the structure of porcine fructose-1,6-bisphosphatase " (2002). Retrospective Theses and Dissertations. 489. https://lib.dr.iastate.edu/rtd/489 This Dissertation is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. -

Observation and Optimization of 2 Μm Mode-Locked Pulses in All-Fiber Net
Opto-Electronic Original Article Advances 2020, Vol. 3, No. 11 DOI: 10.29026/oea.2020.200001 Observation and optimization of 2 μm mode‐locked pulses in all‐fiber net anomalous dispersion laser cavity Wanzhuo Ma1,2, Desheng Zhao1,2, Runmin Liu1,2, Tianshu Wang1,2*, Quan Yuan1,2, Hao Xiong1,2, Haiying Ji1,2 and Huilin Jiang1,2 We integrally demonstrate 2 μm mode-locked pulses performances in all-fiber net anomalous dispersion cavity. Stable mode-locking operations with the center wavelength around 1950–1980 nm can be achieved by using the nonlinear po- larization rotation structure and properly designing the dispersion management component. Conventional soliton is firstly obtained with a total anomalous dispersion cavity. Due to the contribution of commercial ultra-high numerical aperture fibers, net dispersion is reduced to -0.077 ps2. So that stretched pulse with 19.4 nm optical bandwidth is obtained and the de-chirped pulse-width can reach 312 fs using extra-cavity compression. Under pump power greater than 890 mW, stretched pulse can evolve into noise-like pulse with 41.3 nm bandwidth. The envelope and peak of such broadband pulse can be compressed with up to 2.2 ps and 145 fs, respectively. The single pulse energy of largely chirped stretched and noise-like pulse can reach 1.785 nJ and 1.53 nJ, respectively. Furthermore, extra-cavity compression can also contribute to a significant increase of peak power. Keywords: fiber lasers; mode-locked lasers; 2 μm fiber lasers Ma W Z, Zhao D S, Liu R M, Wang T S, Yuan Q et al.