Obstetric Risk Factors and Pelvic Floor Symptoms Associated with Stage II
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Laparoscopic Organopexy with Non-Mesh Genital (LONG)
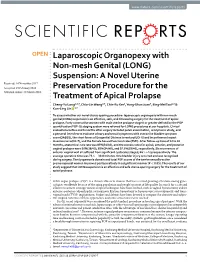
www.nature.com/scientificreports OPEN Laparoscopic Organopexy with Non-mesh Genital (LONG) Suspension: A Novel Uterine Received: 14 November 2017 Accepted: 19 February 2018 Preservation Procedure for the Published: xx xx xxxx Treatment of Apical Prolapse Cheng-Yu Long1,2,3, Chiu-Lin Wang2,3, Chin-Ru Ker1, Yung-Shun Juan4, Eing-Mei Tsai1,3 & Kun-Ling Lin 1,3 To assess whether our novel uterus-sparing procedure- laparoscopic organopexy with non-mesh genital(LONG) suspension is an efective, safe, and timesaving surgery for the treatment of apical prolapse. Forty consecutive women with main uterine prolapse stage II or greater defned by the POP quantifcation(POP-Q) staging system were referred for LONG procedures at our hospitals. Clinical evaluations before and 6 months after surgery included pelvic examination, urodynamic study, and a personal interview to evaluate urinary and sexual symptoms with overactive bladder symptom score(OABSS), the short forms of Urogenital Distress Inventory(UDI-6) and Incontinence Impact Questionnaire(IIQ-7), and the Female Sexual Function Index(FSFI). After follow-up time of 12 to 30 months, anatomical cure rate was 85%(34/40), and the success rates for apical, anterior, and posterior vaginal prolapse were 95%(38/40), 85%(34/40), and 97.5%(39/40), respectively. Six recurrences of anterior vaginal wall all sufered from signifcant cystocele (stage3; Ba>+1) preoperatively. The average operative time was 73.1 ± 30.8 minutes. One bladder injury occurred and was recognized during surgery. The dyspareunia domain and total FSFI scores of the twelve sexually-active premenopausal women improved postoperatively in a signifcant manner (P < 0.05). -

Chapter 14 – Female Reproductive Organs
Chapter 14 – Female reproductive organs The fee allowance for a hysteroscopy procedure includes an amount for dilation and curettage (D&C) and the insertion of a Mirena coil so we will not reimburse additional fees charged for these procedures. Similarly, where a therapeutic hysteroscopy is carried out, we will not pay any additional fees charged for a diagnostic hysteroscopy. The fee allowance for a hysterectomy procedure for ovarian malignancy includes an amount for the removal of the omentum and so this should not be charged as an additional procedure. A cystoscopy should not be charged as an additional procedure alongside any suspension/uro-gynaecological procedure. The insertion of a suprapubic catheter is considered part and parcel of procedures such as a suprapubic sling or the retropubic suspension of the bladder neck and so we will not pay any additional fees charged for this procedure. The fee allowance for a colposcopy procedure includes an amount for a punch biopsy. The fee allowance for a therapeutic laparoscopy includes an amount for a diagnostic laparoscopy. The code for the insertion of a prosthesis into the ureter is intended for use by urologists inserting a stent and not for circumstances where the ureter is being identified during hysterectomy. However, we recognise this does involve some additional work and consider a small uplift in the fee to be reasonable. Many pathological processes result in the formation of adhesions so ‘adhesiolysis’ is considered to be a normal part and parcel of these procedures. Therefore, we do not have a specific code for the division of adhesions. -

To Repair Uterine Prolapse
IP 372/2 [IPGXXX] NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of uterine suspension using mesh (including sacrohysteropexy) to repair uterine prolapse Uterine prolapse happens when the womb (uterus) slips down from its usual position into the vagina. Uterine suspension using mesh involves attaching 1 end of the mesh to the lower part of the uterus or cervix. The other end is attached to a bone at the base of the spine or to a ligament in the pelvis. The procedure can be done through open abdominal surgery or laparoscopy (keyhole surgery). The aim is to support the womb. Introduction The National Institute for Health and Care Excellence (NICE) has prepared this interventional procedure (IP) overview to help members of the interventional procedures advisory committee (IPAC) make recommendations about the safety and efficacy of an interventional procedure. It is based on a rapid review of the medical literature and specialist opinion. It should not be regarded as a definitive assessment of the procedure. Date prepared This IP overview was prepared in January 2016. Procedure name Uterine suspension using mesh (including sacrohysteropexy) to repair uterine prolapse. Specialist societies Royal College of Obstetricians and Gynaecologists (RCOG) British Society of Urogynaecology (BSUG) British Association of Urological Surgeons (BAUS). IP overview: Uterine suspension using mesh (including sacrohysteropexy) to repair uterine prolapse. Page 1 of 75 IP 372/2 [IPGXXX] Description Indications and current treatment Uterine prolapse is when the uterus descends from its usual position, into and sometimes through, the vagina. It can affect quality of life by causing symptoms of pressure and discomfort, and by its effects on urinary, bowel and sexual function. -

NVA Research Update E- Newsletter September – October – November 2016
NVA Research Update E- Newsletter September – October – November 2016 www.nva.org __________________________ Vulvodynia The Vulvar Pain Assessment Questionnaire inventory. Dargie E, Holden RR, Pukall CF. Pain. 2016 Aug 1. https://www.ncbi.nlm.nih.gov/pubmed/27780177 Millions suffer from chronic vulvar pain (ie, vulvodynia). Vulvodynia represents the intersection of 2 difficult subjects for health care professionals to tackle: sexuality and chronic pain. Those with chronic vulvar pain are often uncomfortable seeking help, and many who do so fail to receive proper diagnoses. The current research developed a multidimensional assessment questionnaire, the Vulvar Pain Assessment Questionnaire (VPAQ) inventory, to assist in the assessment and diagnosis of those with vulvar pain. A large pool of items was created to capture pain characteristics, emotional/cognitive functioning, physical functioning, coping skills, and partner factors. The item pool was subsequently administered online to 288 participants with chronic vulvar pain. Of those, 248 participants also completed previously established questionnaires that were used to evaluate the convergent and discriminant validity of the VPAQ. Exploratory factor analyses of the item pool established 6 primary scales: Pain Severity, Emotional Response, Cognitive Response, and Interference with Life, Sexual Function, and Self-Stimulation/Penetration. A brief screening version accompanies a more detailed version. In addition, 3 supplementary scales address pain quality characteristics, coping skills, and the impact on one's romantic relationship. When relationships among VPAQ scales and previously researched scales were examined, evidence of convergent and discriminant validity was observed. These patterns of findings are consistent with the literature on the multidimensional nature of vulvodynia. The VPAQ can be used for assessment, diagnosis, treatment formulation, and treatment monitoring. -

Controversies and Complications in Pelvic Reconstructive Surgery (Didactic)
Controversies and Complications in Pelvic Reconstructive Surgery (Didactic) PROGRAM CHAIR Andrew I. Sokol, MD Cheryl B. Iglesia, MD Charles R. Rardin, MD Sponsored by AAGL Advancing Minimally Invasive Gynecology Worldwide Professional Education Information Target Audience Educational activities are developed to meet the needs of surgical gynecologists in practice and in training, as well as, other allied healthcare professionals in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. -

Gender Reassignment Surgery Policy Number: PG0311 ADVANTAGE | ELITE | HMO Last Review: 07/01/2021
Gender Reassignment Surgery Policy Number: PG0311 ADVANTAGE | ELITE | HMO Last Review: 07/01/2021 INDIVIDUAL MARKETPLACE | PROMEDICA MEDICARE PLAN | PPO GUIDELINES This policy does not certify benefits or authorization of benefits, which is designated by each individual policyholder terms, conditions, exclusions and limitations contract. It does not constitute a contract or guarantee regarding coverage or reimbursement/payment. Self-Insured group specific policy will supersede this general policy when group supplementary plan document or individual plan decision directs otherwise. Paramount applies coding edits to all medical claims through coding logic software to evaluate the accuracy and adherence to accepted national standards. This medical policy is solely for guiding medical necessity and explaining correct procedure reporting used to assist in making coverage decisions and administering benefits. SCOPE X Professional X Facility DESCRIPTION Transgender is a broad term that can be used to describe people whose gender identity is different from the gender they were thought to be when they were born. Gender dysphoria (GD) or gender identity disorder is defined as evidence of a strong and persistent cross-gender identification, which is the desire to be, or the insistence that one is of the other gender. Persons with this disorder experience a sense of discomfort and inappropriateness regarding their anatomic or genetic sexual characteristics. Individuals with GD have persistent feelings of gender discomfort and inappropriateness of their anatomical sex, strong and ongoing cross-gender identification, and a desire to live and be accepted as a member of the opposite sex. Gender Dysphoria (GD) is defined by the Diagnostic and Statistical Manual of Mental Disorders - Fifth Edition, DSM-5™ as a condition characterized by the "distress that may accompany the incongruence between one’s experienced or expressed gender and one’s assigned gender" also known as “natal gender”, which is the individual’s sex determined at birth. -

Oophorectomy Or Salpingectomy— Which Makes More Sense?
Oophorectomy or salpingectomy— which makes more sense? During hysterectomy for benign indications, many surgeons routinely remove the ovaries to prevent cancer. Here’s what we know about this practice. William H. Parker, MD CASE Patient opts for hysterectomy, asks than age 45 to prevent the subsequent devel- about oophorectomy opment of ovarian cancer (FIGURES 1 and 2). Your 46-year-old patient reports increasingly The 2002 Women’s Health Initiative re- severe dysmenorrhea at her annual visit, and a port suggested that exogenous hormone use pelvic examination reveals an enlarged uterus. was associated with a slight increase in the You order pelvic magnetic resonance imaging, risk of breast cancer.2 After its publication, which shows extensive adenomyosis. the rate of oophorectomy at the time of hys- After you counsel the patient about terectomy declined slightly, likely reflect- IN THIS her options, she elects to undergo lapa- ARTICLE ing women’s desire to preserve their own roscopic supracervical hysterectomy and source of estrogen.3 For women younger Algorithm: Should asks whether she should have her ovaries than age 50, further slight declines in the rate the ovaries removed at the time of surgery. She has no of oophorectomy were seen from 2002 to be removed? family history of ovarian or breast cancer. 2010. However, in the United States, almost page 54 What would you recommend for this 300,000 women still undergo “prophylactic” woman, based on her situation and current bilateral salpingo-oophorectomy every year.4 medical research? The lifetime risk of ovarian cancer Ovarian cancer does among women with a BRCA 1 mutation not come from the prophylactic procedure should be is 36% to 46%, and it is 10% to 27% among ovary considered only if 1) there is a rea- women with a BRCA 2 mutation. -

Salpingectomy for Ovarian Cancer Prevention Approved 11/9/2017
Health Evidence Review Commission (HERC) Coverage Guidance: Opportunistic Salpingectomy for Ovarian Cancer Prevention Approved 11/9/2017 HERC Coverage Guidance Opportunistic salpingectomy during gynecological procedures is recommended for coverage, without an increased payment (i.e., using a form of reference-based pricing) (weak recommendation). Note: Definitions for strength of recommendation are in Appendix A. GRADE Informed Framework Element Description. Table of Contents HERC Coverage Guidance ............................................................................................................................. 1 Rationale for development of coverage guidances and multisector intervention reports .......................... 3 GRADE-Informed Framework ....................................................................................................................... 4 Should opportunistic salpingectomy be recommended for coverage for ovarian cancer risk reduction? .................................................................................................................................................................. 4 Clinical Background ....................................................................................................................................... 7 Indications ................................................................................................................................................. 7 Technology Description ........................................................................................................................... -
Table of Contents
Society for Sex Therapy and Research SSTAR 2008: 33rd Annual Meeting Continuing Medical Education Credit is provided through joint sponsorship with The American College of Obstetricians and Gynecologists (ACOG). Intercontinental Hotel Chicago, Illinois USA March 13-15, 2008 TABLE OF CONTENTS President‘s Welcome ..........................................................................................................1 SSTAR 2009: 34th Annual Meeting – Arlington, Virginia, USA ........................................2 SSTAR 2008 Fall Clinical Meeting – New York, New York USA ....................................2 SSTAR Executive Council and Administrative Staff ..........................................................3 Continuing Education Accreditations & Approvals ............................................................5 Acknowledgements ..............................................................................................................6 Program Schedule ................................................................................................................7 2008 Award Recipients ....................................................................................................14 SSTAR Health Professional Book Award .............................................................14 Sex, Therapy, and Kids Recipient: Sharon Lamb, EdD SSTAR Service Award ..........................................................................................14 Recipient: Bill Maurice, MD SSTAR Student Research Award Abstract ............................................................15 -

Co™™I™™Ee Opinion
The American College of Obstetricians and Gynecologists WOMEN’S HEALTH CARE PHYSICIANS COMMITTEE OPINION Number 673 • September 2016 (Replaces Committee Opinion No. 345, October 2006) Committee on Gynecologic Practice This Committee Opinion was developed by the American College of Obstetricians and Gynecologists’ Committee on Gynecologic Practice and the American Society for Colposcopy and Cervical Pathology (ASCCP) in collaboration with committee member Ngozi Wexler, MD, MPH, and ASCCP members and experts Hope K. Haefner, MD, Herschel W. Lawson, MD, and Colleen K. Stockdale, MD, MS. This document reflects emerging clinical and scientific advances as of the date issued and is subject to change. The information should not be construed as dictating an exclusive course of treatment or procedure to be followed. Persistent Vulvar Pain ABSTRACT: Persistent vulvar pain is a complex disorder that frequently is frustrating to the patient and the clinician. It can be difficult to treat and rapid resolution is unusual, even with appropriate therapy. Vulvar pain can be caused by a specific disorder or it can be idiopathic. Idiopathic vulvar pain is classified as vulvodynia. Although optimal treatment remains unclear, consider an individualized, multidisciplinary approach to address all physical and emotional aspects possibly attributable to vulvodynia. Specialists who may need to be involved include sexual counselors, clinical psychologists, physical therapists, and pain specialists. Patients may perceive this approach to mean the practitioner does not believe their pain is “real”; thus, it is important to begin any treatment approach with a detailed discussion, including an explanation of the diagnosis and determination of realistic treatment goals. Future research should aim at evaluating a multimodal approach in the treatment of vulvodynia, along with more research on the etiologies of vulvodynia. -

Abdominal Sacrohysteropexy Versus Vaginal Hysterectomy for Pelvic Organ Prolapse in Young Women
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Bhalerao AV et al. Int J Reprod Contracept Obstet Gynecol. 2020 Apr;9(4):1434-1441 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20201201 Original Research Article Abdominal sacrohysteropexy versus vaginal hysterectomy for pelvic organ prolapse in young women Anuja V. Bhalerao, Vaidehi A. Duddalwar* Department of Obstetrics and Gynecology, N. K. P. Salve Institute of Medical Sciences, Nagpur, Maharashtra, India Received: 11 February 2020 Accepted: 03 March 2020 *Correspondence: Dr. Vaidehi A. Duddalwar, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: Pelvic organ prolapse (POP) is the descent of the pelvic organs beyond their anatomical confines. The definitive treatment of symptomatic prolapse is surgery but its management in young is unique due to various considerations. Aim of this study was to evaluate anatomical and functional outcome after abdominal sacrohysteropexy and vaginal hysterectomy for pelvic organ prolapse in young women. Methods: A total 27 women less than 35 years of age with pelvic organ prolapse underwent either abdominal sacrohysteropexy or vaginal hysterectomy with repair. In all women, pre-op and post-op POP-Q was done for evaluation of anatomical defect and a validated questionnaire was given for subjective outcome. Results: Anatomical outcome was significant in both groups as per POP-Q grading but the symptomatic outcome was better for sacrohysteropexy with regard to surgical time, bleeding, ovarian conservation, urinary symptoms, sexual function. -

(8Th Edition) Procedure Code ACHI (8
Appendix 1. Procedure and Diagnostic Codes Used to Identify Prior Procedures Procedure ACHI (8th ACHI (8th edition) procedure names ICD-10- ICD-10-AM edition) AM diagnosis name procedure diagnosis code code Gynecological laparoscopy 35638-00 Laparoscopic wedge resection of ovary 35638-01 Laparoscopic partial oophorectomy 35638-02 Laparoscopic oophorectomy, unilateral 35638-03 Laparoscopic oophorectomy,bilateral 35638-04 Laparoscopic ovarian cystectomy, unilateral 35638-05 Laparoscopic ovarian cystectomy, bilateral 35638-06 Laparoscopic salpingotomy 35638-07 Laparoscopic partial salpingectomy, unilateral 35638-08 Laparoscopic partial salpingectomy, bilateral 35638-09 Laparoscopic salpingectomy, unilateral 35638-10 Laparoscopic salpingectomy, bilateral 35638-11 Laparoscopic salpingo-oophorectomy, unilateral 35638-12 Laparoscopic salpingo-oophorectomy, bilateral 35638-14 Laparoscopic uterosacral nerve ablation 35637-02 Laparoscopic diathermy of lesion of pelvic cavity 35637-04 Laparoscopic ventrosuspension 35637-07 Laparoscopic rupture of ovarian cyst or abscess 35637-08 Laparoscopic ovarian drilling 35637-10 Laparoscopic excision of lesion of pelvic cavity 35729-00 Laparoscopic transposition of ovary 90430-00 Laparoscopic repair of ovary 90433-00 Other laparoscopic repair of fallopian tube 35694-00 Laparoscopic salpingoplasty 35694-01 Laparoscopic anastomosis of fallopian tube 35694-02 Laparoscopic salpingolysis 35694-03 Laparoscopic salpingostomy 35694-06 Laparoscopic salpingotomy 35649-01* Myomectomy of uterus via laparoscopy Hysteroscopy, including operative hysteroscopy 35630-00 Diagnostic hysteroscopy 35649-00 Hysterotomy 35633-00 Division of uterine adhesions 35634-00 Division of uterine septum via hysteroscopy 35649-02 Division of uterine septum via hysterotomy 35633-01 Polypectomy of uterus via hysteroscopy 35623-00 Myomectomy of uterus via hysteroscopy Baldwin HJ, Patterson JA, Nippita TA, Torvaldsen S, Ibiebele I, Simpson JM, et al. Antecedents of abnormally invasive placenta in primiparous women: the risk from gynecologic procedures.