A Hospital-Based Study on Clinical Data, Demographic Data and Visual
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treat Cataracts and Astigmatism with One
TREAT CATARACTS Cataract patients have a choice Eye with cataract See life through the AcrySof® IQ Toric IOL. of treatments, including the As the eye ages, the lens becomes AND ASTIGMATISM WITH breakthrough AcrySof® IQ Toric cloudier, allowing less light to pass Ask your doctor about your options. intraocular lens (IOL) that treats through. The light that doesn’t make ONE PROCEDURE pre-existing corneal astigmatism at the it to the retina is diffused or scattered, same time that it corrects cataracts. leaving vision defocused and blurry. With a single procedure, you have the potential to enjoy freedom from glasses or contacts for distance vision with enhanced image quality – and see life through a new lens. 1. Independent third party research; Data on File, December 2011. Cataracts and astigmatism defined. Important Product Information A cataract is like a cloud over the eye’s lens, Eye with astigmatism CAUTION: Restricted by law to sale by or on the order of a physician. DESCRIPTION: interfering with quality of vision and making The AcrySof® IQ Toric Intraocular Lenses (IOLs) are artificial lenses implanted in the normal activities, such as driving a car, reading When the surface of the cornea has eye of adult patients following cataract surgery. These lenses are designed to correct pre-existing corneal astigmatism, which is the inability of the eye to focus clearly at a newspaper or seeing people’s faces, an uneven curvature, shaped more any distance because of difference curvatures on the cornea, and provide distance vision. WARNINGS / PRECAUTIONS: You may experience and need to contact your increasingly difficult. -

Proposed International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales
Proposed International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales C. P. Wilkinson, MD,1 Frederick L. Ferris, III, MD,2 Ronald E. Klein, MD, MPH,3 Paul P. Lee, MD, JD,4 Carl David Agardh, MD,5 Matthew Davis, MD,3 Diana Dills, MD,6 Anselm Kampik, MD,7 R. Pararajasegaram, MD,8 Juan T. Verdaguer, MD,9 representing the Global Diabetic Retinopathy Project Group Purpose: To develop consensus regarding clinical disease severity classification systems for diabetic retinopathy and diabetic macular edema that can be used around the world, and to improve communication and coordination of care among physicians who care for patients with diabetes. Design: Report regarding the development of clinical diabetic retinopathy disease severity scales. Participants: A group of 31 individuals from 16 countries, representing comprehensive ophthalmology, retina subspecialties, endocrinology, and epidemiology. Methods: An initial clinical classification system, based on the Early Treatment Diabetic Retinopathy Study and the Wisconsin Epidemiologic Study of Diabetic Retinopathy publications, was circulated to the group in advance of a workshop. Each member reviewed this using e-mail, and a modified Delphi system was used to stratify responses. At a later workshop, separate systems for diabetic retinopathy and macular edema were developed. These were then reevaluated by group members, and the modified Delphi system was again used to measure degrees of agreement. Main Outcome Measures: Consensus regarding specific classification systems was achieved. Results: A five-stage disease severity classification for diabetic retinopathy includes three stages of low risk, afourthstageofseverenonproliferativeretinopathy,andafifthstageofproliferativeretinopathy.Diabeticmacular edema is classified as apparently present or apparently absent. If training and equipment allow the screener to make a valid decision, macular edema is further categorized as a function of its distance from the central macula. -

Clinical Protocol P-321-202
Clinical Protocol P-321-202 Project Number P-1003-I101 Compound Number/ Name P-321 Ophthalmic Solution Protocol Number P-321-202 Protocol Title Randomized, Double-Masked, Parallel Group Study of P-321 Ophthalmic Solution Compared to Placebo in Subjects with Dry Eye Disease Assessing Safety and Efficacy Over 28 Days Sponsor Parion Sciences, Inc. 2800 Meridian Parkway Suite 195 Durham, NC 27713 Medical Monitor Authors Issue Date Original: Version 1.0 released 29 April 2016 Amendment 1.0: Version 2.0 Released 10 February 2017 Sponsor Signature and Date _____________________________________________ The information in this document is confidential and is provided to you as an investigator or consultant for review by you, your staff, and the applicable Institutional Review Board/Independent Ethics Committee. Your acceptance of this document constitutes agreement that you will not disclose the information contained herein to others without written authorization from Parion Sciences. Parion Sciences, Inc. P-321 Ophthalmic Solution Protocol P-321-202 Amendment 01 PARION SCIENCES, INC. Clinical Protocol P-321-202 Investigator Signature Page Project Number P-1003-I101 Compound Number/ Name P-321 Ophthalmic Solution Protocol Number P-321-202 Protocol Title Randomized, Double-Masked, Parallel Group Study of P - 321 Ophthalmic Solution Compared to Placebo in Subjects with Dry Eye Disease Assessing Safety and Efficacy Over 28 Days Sponsor Parion Sciences, Inc. 2800 Meridian Parkway Suite 195 Durham, NC 27713 Issue Date Original: Version 1.0 released 29 April 2016 Amendment 1.0: Version 2.0: Released 10 February 2017 I have reviewed and understand this protocol and all amendments associated with it. -
LCD): Computerized Corneal Topography (L33810
Local Coverage Determination (LCD): Computerized Corneal Topography (L33810) Links in PDF documents are not guaranteed to work. To follow a web link, please use the MCD Website. Contractor Information CONTRACTOR NAME CONTRACT TYPE CONTRACT NUMBER JURISDICTION STATE(S) First Coast Service Options, Inc. A and B MAC 09102 - MAC B J - N Florida First Coast Service Options, Inc. A and B MAC 09202 - MAC B J - N Puerto Rico First Coast Service Options, Inc. A and B MAC 09302 - MAC B J - N Virgin Islands LCD Information Document Information LCD ID Original Effective Date L33810 For services performed on or after 10/01/2015 LCD Title Revision Effective Date Computerized Corneal Topography For services performed on or after 01/08/2019 Proposed LCD in Comment Period Revision Ending Date N/A N/A Source Proposed LCD Retirement Date N/A N/A AMA CPT / ADA CDT / AHA NUBC Copyright Notice Period Start Date Statement N/A CPT codes, descriptions and other data only are copyright 2019 American Medical Association. All Rights Notice Period End Date Reserved. Applicable FARS/HHSARS apply. N/A Current Dental Terminology © 2019 American Dental Association. All rights reserved. Copyright © 2019, the American Hospital Association, Chicago, Illinois. Reproduced with permission. No portion of the AHA copyrighted materials contained within this publication may be copied without the express written consent of the AHA. AHA copyrighted materials including the UB-04 codes and descriptions may not be removed, copied, or utilized within any Created on 01/02/2020. Page 1 of 7 software, product, service, solution or derivative work without the written consent of the AHA. -
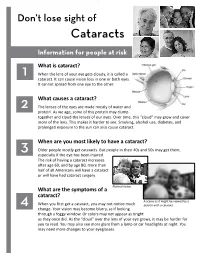
Don't Lose Sight of Cataract
Don’t lose sight of Cataracts Information for people at risk What is cataract? 1 When the lens of your eye gets cloudy, it is called a cataract. It can cause vision loss in one or both eyes. It cannot spread from one eye to the other. What causes a cataract? 2 The lenses of the eyes are made mostly of water and protein. As we age, some of this protein may clump together and cloud the lenses of our eyes. Over time, this “cloud” may grow and cover more of the lens. This makes it harder to see. Smoking, alcohol use, diabetes, and prolonged exposure to the sun can also cause cataract. When are you most likely to have a cataract? 3 Older people mostly get cataracts. But people in their 40s and 50s may get them, especially if the eye has been injured. The risk of having a cataract increases after age 60, and by age 80, more than half of all Americans will have a cataract or will have had cataract surgery. Normal vision. What are the symptoms of a cataract? A scene as it might be viewed by a 4 When you first get a cataract, you may not notice much person with a cataract. change. Your vision may become blurry, as if looking through a foggy window. Or colors may not appear as bright as they once did. As the “cloud” over the lens of your eye grows, it may be harder for you to read. You may also see more glare from a lamp or car headlights at night. -

Division of Health Care Financing & Policy SB 278 Section 16
Division of Health Care Financing & Policy SB 278 Section 16 - Physician Rates Reporting Facility & Non-Facility Rate Comparison Nevada 2016 2016 Medicaid Medicaid Medicaid Medicare Medicare vs. vs. Procedure Code & Description Rates (1) Non-Facility Facility Medicare Medicare Rates for Rates for Non-Facility Facility 10021 Fna w/o image 70.92 128.90 72.80 (57.98) (1.88) 10022 Fna w/image 65.39 148.21 68.38 (82.82) (2.99) 10030 Guide cathet fluid drainage 154.73 827.01 176.71 (672.28) (21.98) 10035 Perq dev soft tiss 1st imag 86.35 568.38 90.92 (482.03) (4.57) 10036 Perq dev soft tiss add imag 43.52 495.42 45.82 (451.90) (2.30) 10040 Acne surgery 87.47 106.03 92.10 (18.56) (4.63) 10060 Drainage of skin abscess 95.60 122.68 101.60 (27.08) (6.00) 10061 Drainage of skin abscess 178.04 215.50 188.01 (37.46) (9.97) 10080 Drainage of pilonidal cyst 103.29 188.83 107.87 (85.54) (4.58) 10081 Drainage of pilonidal cyst 172.45 281.57 177.64 (109.12) (5.19) 10120 Remove foreign body 103.22 159.56 108.73 (56.34) (5.51) 10121 Remove foreign body 185.58 287.08 194.44 (101.50) (8.86) 10140 Drainage of hematoma/fluid 118.06 170.87 124.18 (52.81) (6.12) 10160 Puncture drainage of lesion 95.62 136.49 100.72 (40.87) (5.10) 10180 Complex drainage wound 178.97 258.94 188.14 (79.97) (9.17) 11000 Debride infected skin 28.42 56.88 29.76 (28.46) (1.34) 11001 Debride infected skin add-on 14.22 22.40 14.87 (8.18) (0.65) 11004 Debride genitalia & perineum 579.35 608.28 608.28 (28.93) (28.93) 11005 Debride abdom wall 781.65 822.97 822.97 (41.32) (41.32) 11006 Debride -

Current Developments in Corneal Topography and Tomography
diagnostics Review Current Developments in Corneal Topography and Tomography Piotr Kanclerz 1,2,* , Ramin Khoramnia 3 and Xiaogang Wang 4 1 Hygeia Clinic, Department of Ophthalmologyul, Ja´skowaDolina 57, 80-286 Gda´nsk,Poland 2 Helsinki Retina Research Group, University of Helsinki, 00100 Helsinki, Finland 3 The David J. Apple International Laboratory for Ocular Pathology, Department of Ophthalmology, University of Heidelberg, 69120 Heidelberg, Germany; [email protected] 4 Department of Cataract, Shanxi Eye Hospital, Taiyuan 030002, China; [email protected] * Correspondence: [email protected] Abstract: Introduction: Accurate assessment of the corneal shape is important in cataract and refractive surgery, both in screening of candidates as well as for analyzing postoperative outcomes. Although corneal topography and tomography are widely used, it is common that these technologies are confused. The aim of this study was to present the current developments of these technologies and particularly distinguish between corneal topography and tomography. Methods: The PubMed, Web of Science and Embase databases were the main resources used to investigate the medical literature. The following keywords were used in various combinations: cornea, corneal, topography, tomography, Scheimpflug, Pentacam, optical coherence tomography. Results: Topography is the study of the shape of the corneal surface, while tomography allows a three-dimensional section of the cornea to be presented. Corneal topographers can be divided into large- and small-cone Placido-based devices, as well as devices with color-LEDs. For corneal tomography, scanning slit or Scheimpflug imaging and optical coherence tomography may be employed. In several devices, corneal topography and tomography have been successfully combined with tear-film analysis, aberrometry, optical biometry and anterior/posterior segment optical coherence tomography. -
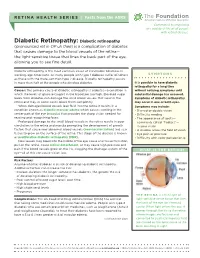
Diabetic Retinopathy
RETINA HEALTH SERIES | Facts from the ASRS The Foundation American Society of Retina Specialists Committed to improving the quality of life of all people with retinal disease. Diabetic Retinopathy: Diabetic retinopathy (pronounced ret in OP uh thee) is a complication of diabetes that causes damage to the blood vessels of the retina— the light-sensitive tissue that lines the back part of the eye, allowing you to see fine detail. Diabetic retinopathy is the most common cause of irreversible blindness in working-age Americans. As many people with type 1 diabetes suffer blindness SYMPTOMS as those with the more common type 2 disease. Diabetic retinopathy occurs in more than half of the people who develop diabetes. It is possible to have diabetic retinopathy for a long time Causes: The primary cause of diabetic retinopathy is diabetes—a condition in without noticing symptoms until which the levels of glucose (sugar) in the blood are too high. Elevated sugar substantial damage has occurred. levels from diabetes can damage the small blood vessels that nourish the Symptoms of diabetic retinopathy retina and may, in some cases, block them completely. may occur in one or both eyes. When damaged blood vessels leak fluid into the retina it results in a Symptoms may include: condition known as diabetic macular edema which causes swelling in the • Blurred or double vision center part of the eye (macula) that provides the sharp vision needed for • Difficulty reading reading and recognizing faces. • The appearance of spots— Prolonged damage to the small blood vessels in the retina results in poor commonly called “floaters”— circulation to the retina and macula prompting the development of growth in your vision factors that cause new abnormal blood vessels (neovascularization) and scar • A shadow across the field of vision tissue to grow on the surface of the retina. -

Safety and Effectiveness of the UV-X System for Corneal Collagen Cross
Evaluation of two Riboflavin Dosing Regimens for Corneal Collagen Cross-Linking in Eyes with Progressive Keratoconus or Ectasia Protocol 2010-0243, Version: 15 Protocol Date: September 16, 2016 PHYSICIAN SPONSOR: Francis W. Price, Jr. MD CONFIDENTIAL Background This clinical protocol is designed to evaluate two riboflavin-dosing regimens for treatment of patients with progressive keratoconus or corneal ectasia using investigational technology that increases the cross linking of the corneal stroma using the photochemical interaction of UVA light with the chromophore riboflavin. In this treatment, the corneal stroma is saturated with riboflavin by irrigating the surface after removal of the corneal epithelium. The riboflavin-saturated cornea is then exposed to a uniform field of UVA light with a narrow bandwidth centered at 365 nm. The light is generated by an IROC UV-X irradiation system that creates a uniform 11 mm circle of UVA light. The device has a timer that allows a precise 30-minute exposure of the corneal tissues. The irradiation field of the UVX system produces UVA light with a uniform irradiance of 3 mj/cm2 at the corneal surface. The FDA has classified this technology as a combination product with two components. First is the UV-X light source, which has an LED source and is calibrated and rendered uniform by the use of an optical homogenizer. The second component is a riboflavin ophthalmic solution. This solution is used to saturate the corneal stroma prior to its photochemical activation. This combination product has been studied in a FDA-approved, randomized, placebo- controlled, multi-center trial that has enrolled patients. -

Fact Sheet About Diabetic Macular Edema (Dme)
FACT SHEET ABOUT DIABETIC MACULAR EDEMA (DME) WHAT IS DME? Diabetic Macular Edema (DME) or "swelling of the macula" is a common complication in the eyes of patients with diabetes. It is a frequent cause of vision loss in patients with diabetes, and can eventually lead to blindness.1,2 The macula is the part of the retina responsible for central or fine vision. In DME, blood vessels in the retina are damaged by chronic high blood sugar levels. A breakdown in the blood-retinal barrier and increased vascular permeability allows fluid from blood vessels to leak into the retina, causing macular swelling.2 Fluid in the macula can cause severe vision loss or blindness.2 Vascular endothelial growth factor (VEGF), a naturally occurring family of growth factors in the body, appears to play a critical role in the development of DME.3 Increased VEGF production contributes to the vascular disruptions and leakage that characterize DME, as well as the formation of new blood vessels (a process known as angiogenesis) seen in more advanced forms of diabetic retinopathy (DR).2 DME STATISTICS According to the Centers for Disease Control and Prevention, approximately 29.1 million adults are living with diabetes (types I & II) in the U.S. 4 Of those, approximately 1.5 million people are diagnosed with DME.5 o The prevalence of DME is especially high among racial and ethnic minorities, particularly in African Americans.6 DME is the leading cause of blindness in young adults in developed countries.7 The increasing number of individuals with diabetes worldwide suggests that DME will continue to be a major contributor to vision loss and associated functional impairment. -

Refractive Surgery
I explore and get information from inside the eye, that´s my job. You can then go deeper into the diagnosis. You decide, I explore! FOR ACCURACY IN REFRACTIVE SURGERY ACE® is a technology that utilizes the power of high-resolution swept-source OCT imaging to provide the key corneal measurements. Optimizing the quality of the preoperative data provides more information to help you to improve the safety of your refractive surgery procedures.1 ACE® and the TECHNOLAS® TeneoTM 317 Model 2 offer solutions that will refine your results. Transform your daily surgical routine into an exciting day with a platform that brings together corneal topography and tomography and allowing data transfer between both devices. All corneal measurements are based on high-resolution swept-source OCT images KEY FUNCTIONS Corneal topography Corneal wavefront analysis Corneal tomography Differential maps Pachymetry Progression analysis Total corneal power Data transfer with TECHNOLAS® TENEOTM 317 Model 2 * All corneal measurements based on high- resolution swept-source OCT images 1. Muriël Doors et al. Value of optical coherence tomography for anterior segment surgery. J Cataract Refract Surg 2010; 36:1213–1229 Q 2010 ADVANCED CORNEAL EXPLORER HIGHLY CUSTOMIZABLE MAP LAYOUT Display up to 6 maps simultaneously, compare OD and OS, or perform an analysis over time. 12 different map types: Assess each patient’s corneal topography and Anterior and posterior axial or Pachymetry tomography, including tangential curvature Total corneal power curvature and elevation Anterior and posterior elevation maps of the anterior and Anterior and total corneal wavefront (best fit sphere and best fit torus) posterior surfaces. -

Dry Eye Syndrome in Type II Diabetic Patients Attending a Medical College Teaching Hospital
12 Ophthalmology and Allied Sciences Volume 4 Number 1, January - April 2018 Original Article DOI: http://dx.doi.org/10.21088/oas.2454.7816.4118.2 Dry Eye Syndrome in Type II Diabetic Patients Attending A Medical College Teaching Hospital Gnanajyothi C. Bada*, Satish S. Patil** *Assistant Professor, Department of Ophthalmology, Khaja Banda Nawaz Institute of Medical Sciences, Kalaburagi, Karnataka 585104, India. **Assistant ProfessorDepartment of Physiology, M R Medical College, Kalaburagi, Karnataka 585105, India. Abstract Introduction: Diabetes mellitus is one of the leading health problem all over the world. Dry eye syndrome (DES) is common in diabetes mellitus. The study was done to detect theprevalence of DES in type II diabetic patients and to determine the association of dry eyes with diabetic retinopathy. Methodology: Diabetic patients(n=200) attending Ophthalmology OPD at Khaja Bande Nawaz Institute of Medical Sciences (KBNIMS), Kalaburagi during the period fromApril to December 2017 were included in the study group, basedon the inclusion & exclusion criteria. Results: Our study showed that the prevalence of DES in diabetes was 51%, with higher rate in females and older age group. 33% of diabetic retinopathy patients had DES even though it was not statistically significant. Conclusion: Since there exists an association between diabetes and DES, all diabetic patients should be screened for DES to prevent ocular surface damage. Keywords: Diabetes Mellitus; Diabetic Retinopathy; Dry Eye Syndrome (DES). Introduction itchiness, redness, pain, ocular fatigue and visual disturbance [6]. DES results in corneal and conjunctival epithelial alterations such as punctate Diabetes mellitus is one of the leading health keratopathy, recurrent erosions, persistent epithelial problem all over the world [1].