A Density Analysis of Settlement and Health Facility Access in Rural and Urban Areas
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Civil Service Reforms Unit Draft Position Paper on Creation of District Service
CIVIL SERVICE REFORMS UNIT DRAFT POSITION PAPER ON CREATION OF DISTRICT SERVICE General. Reconstruction of the Civil Service is an essential prerequisite for the effective performance of core government functions at all levels. Implementation of the Devolution Plan will remain incomplete without the restructuring of Civil Services at Federal, Provincial and District levels, including Tehsil. 2. In keeping with the bottom-up approach, the CSRU envisages a two- phased project. The First Phase being focused on the creation of District Services through legislation, and Phase Two would consider the broader agenda of linkages with the Provincial government, through administrative instructions and Rules of Business. 3. The purpose of this Concept Paper is:- a. To identify the basic Strategic Direction, for the creation of district service. b. Develop recommendations that address the fundamental issues of effective devolution of administrative functions to the district and tehsil levels. c. Having created an atmosphere of acceptability, involve the Provincial governments in formulating an implementation plan for gradual introduction of the District Service in the provinces. d. An extremely important adjunct to the above steps is, a detailed analysis of existing service structures, and propose a new legal and institutional framework for District Service. 4. Consensus Building. In order to build a consensus regarding creation of a district service, it is imperative that a clear demarcation of areas of influence between various stake holders are identified. These are:- a. Provincial Governments. (1) Constitutional Right. Provinces, legally speaking, have all the constitutional right to organize and structure the District Service 1 as they want. Thus the basic structure of a district service must come from the provinces. -

Tehsil Wise Population of the District (As Per Census 2001)
Tehsil Wise Population of the District (As per Census 2001):- Tehsil Name Total SC ST Gen Rural Urban RaghurajNagar 660665 114400 72361 473904 380123 280542 Rampur Baghelan 233232 34665 30639 167928 215059 18173 Nagod 200254 44228 16253 139773 180793 19461 Unchehra 160016 25244 31324 103448 143352 16664 Amarpatan 188005 25989 25312 136704 171634 16371 RamNagar 133393 16593 33900 82900 133393 0 Maihar 294539 43098 58615 193126 260197 34342 Total of The District 1870104 304217 268104 1297783 1484551 385553 (Source - District Statistical Book 2008-2009, Satna) Subdivisions/Tehsils/RI Circles/Patwari Circles:- No. of RI Name of SubDivision Name of Tehsils No. of Patwari Circles Circles Raghuraj Nagar RaghurajNagar 8 111 Rampur Baghelan Rampur Baghelan 4 68 Nagod 3 57 Nagod Unchehra 3 40 AmarPatan 3 50 AmarPatan RamNagar 3 47 Maihar Maihar 4 65 Total 28 438 (Source - District Statistical Book 2008-2009, Satna) Demography (Census 2001):- S.No. Particulars Unit India M.P. Satna 1 Population Density Per Sq.Km. 324 196 249 2 Decade Growth rate % 21.34 24.34 27.52 3 Sex Ratio Per 1000 Male 933 920 926 4 SC to total population % 16.48 14.54 16.26 5 ST to total population % 8.08 23.27 14.23 6 Rural population % 73 74.7 79.28 (Source - District Statistical Book 2002-2003, Satna) Literacy 2001:- S.No. Particulars Unit India M.P. Satna 1 Total % 65.38 64.11 65.12 2 Male % 75.85 76.8 77.82 3 Female % 54.16 50.28 49.1 4 Rural % 59.4 58.1 61.66 5 Urban % 80.3 79.67 78.30 (Source - District Statistical Book 2002-2003, Satna) Block wise details of the District:- Weekly Name of the Area in Inhabited Village Nagar Nagar Nagar S.No. -

The Aid in Danger Monthly News Brief – April 2019 Page 1
Aid in Danger Monthly News Brief April 2019 Safety, security and access incidents Insecurity affecting aid workers and aid delivery Africa This monthly digest comprises threats and Burkina Faso incidents of violence 10 April 2019: In Dagou town, Foutouri department, Komondjari affecting the delivery of province, militants presumed to be from JNIM and/or ISGS broke into aid. the home of a municipal councillor and abducted him along with an NGO worker presumed to have been at his home. The councillor’s son It is prepared by had also been abducted three days prior. Source: ACLED1 Insecurity Insight from information available in 15 April 2019 (DOA): Update: The Burkinabe Government announced open sources. that an Italian missionary, who was abducted in September 2018 in Niger, may have since been held in Burkina Faso. No further details All decisions made, on specified. Source: AFP the basis of, or with consideration to, such Cameroon information remains 19 April 2019: In Buea town, South-West region, a national staff the responsibility of member of a local NGO was kidnapped by unidentified armed their respective militants before being released a few days later. Source: UN-OCHA organisations. Central African Republic Subscribe here to 04 April 2019: In Ouham prefecture, on the road between Batangafo receive monthly reports and Bouca, an MSF staff member who worked at Batangafo Hospital on insecurity affecting was detained by an unidentified armed group before being held the delivery of aid. captive in the bush and killed. His motorcycle was also stolen by the perpetrators. Source: ACLED1, AWSD2, MSF, and UN-OCHA Visit our website to Democratic Republic of the Congo download previous Aid Throughout April 2019: In North Kivu and Ituri provinces, mistrust of in Danger Monthly first responders and widespread misinformation propagated by News Briefs. -

Hatnoli, Tehsil- Khalapur, District- Raigad, Maharashtra, by M/S Jairamjiki Developments Ltd
Proposed Township at Village- Hatnoli, Tehsil- Khalapur, District- Raigad, Maharashtra, by M/s Jairamjiki Developments Ltd. Brief Summary The proposed “Township” located at Village- Hatnoli, Tehsil -Khalapur, District– Raigad, Maharashtra being developed by M/s Jairamjiki Developments Ltd. The company is having its registered office at Soni House, opp. Roop Talkies, Nehru Road, Santacruz East, Mumbai- 400055. The management of the company has decided to develop a Township. The company has already acquired the land measuring 101 Acres at Vill-Hatnoli, Tehsil- Khalapur, District- Raigad, Maharashtra to develop a township at the proposed site. The area is already attracted by well known builders and developers those are developing the area very fast. The site is ideal as it is far from densely populated area of Karjat and Chowk. SITE LOCATION AND SURROUNDINGS The proposed project site is located at Village- Hatnoli, Tehsil -Khalapur, District– Raigad, Maharashtra. The Coordinates of the project site are: 1. 18° 53'45.78"N & 73°15'08.56"E 2. 18° 53'34.47"N & 73°15'15.39"E 3. 18° 53'09.98"N & 73°15'02.63"E 4. 18° 53'21.87"N & 73°14'51.76"E The nearest highway is NH 48 which is approx. 50 m in North direction. The nearest railway station is Chowk Railway Station at a distance of approx. 1.29 Km. in NW direction from the proposed project site. The nearest airport is Chhatrapati Shivaji International Airport at a distance of approx. 45 km in NW direction from the project site. Figure-1: Google image showing the project site Prepared by: Vardan EnviroNet, Gurugram Proposed Township at Village- Hatnoli, Tehsil- Khalapur, District- Raigad, Maharashtra, by M/s Jairamjiki Developments Ltd. -

District Population Statistics, 22 Allahabad, Uttar Pradesh
.------·1 Census of India, 1951 I DISTRICT POPULATION STATISTICS UTTAR PRADESH 22-ALLAHABAD DISTRICT t I 315.42 ALLAHABAD: PluNnNG AND STATIONERY, UTTAR PRADESH, INDIA 1951 1953 ALL CPS Price, Re.1-S. FOREWORD THE Uttar Pradesh Government asked me in March, 1952, to supply them for the purposes of elections to local bodies population statistics with separation for scheduled castes (i) mohalla/ward -wise for urban areas, and (ii) village-wise for rural areas. The Census Tabulation Plan did not provide for sorting of scheduled castes population for areas smaller than a tehsil or urban tract and the request from the Uttar Pradesh Government came when the slip sorting had been finished and the Tabulation Offices closed. As the census slips are mixed up for the purposes of sorting in one lot for a tehsil or urban tract, collection of data regarding scheduled castes population by mohallas/wards and villages would have involved enormous labour and expense if sorting of the slips had been taken up afresh. Fortunately, however, a secondary census record, viz. the National Citizens' Register, in which each slip has been copied, was available. By singular foresight it had been pre pared mohalla/ward-wise for urban areas and village-wise for rural areas. The required information has, therefore, been extracted from this record. 2. In the above circumstances there is a slight difference in the figures of population as arrived at by an earlier sorting of the slips and as now determined by counting from the National Citizens' Register. This difference has been accen tuated by an order passed by me during the later count. -

Jammu & Kashmir Reorganisation Act 2019
jftLVªh lañ Mhñ ,yñ—(,u)04@0007@2003—19 REGISTERED NO. DL—(N)04/0007/2003—19 vlk/kkj.k EXTRAORDINARY Hkkx II — [k.M 1 PART II — Section 1 izkf/kdkj ls izdkf'kr PUBLISHED BY AUTHORITY lañ 53] ubZ fnYyh] 'kqØokj] vxLr 9] [email protected] 18] 1941 ¼'kd½ No. 53] NEW DELHI, FRIDAY, AUGUST 9, 2019/SHRAVANA 18, 1941 (SAKA) bl Hkkx esa fHkUu i`"B la[;k nh tkrh gS ftlls fd ;g vyx ladyu ds :i esa j[kk tk ldsA Separate paging is given to this Part in order that it may be filed as a separate compilation. MINISTRY OF LAW AND JUSTICE (Legislative Department) New Delhi, the 9th August, 2019/Shravana 18, 1941 (Saka) The following Act of Parliament received the assent of the President on the 9th August, 2019, and is hereby published for general information:— THE JAMMU AND KASHMIR REORGANISATION ACT, 2019 NO. 34 OF 2019 [9th August, 2019.] An Act to provide for the reorganisation of the existing State of Jammu and Kashmir and for matters connected therewith or incidental thereto. BE it enacted by Parliament in the Seventieth Year of the Republic of India as follows:— PART-I PRELIMINARY 1. This Act may be called the Jammu and Kashmir Reorganisation Act, 2019. Short title. 2. In this Act, unless the context otherwise requires,— Definitions. (a) “appointed day” means the day which the Central Government may, by notification in the Official Gazette, appoint; (b) “article” means an article of the Constitution; (c) “assembly constituency” and “parliamentary constituency” have the same 43 of 1950. -

Full Title: Adult Mortality in India: the Health–Wealth Nexus
Full Title: Adult Mortality in India: The Health–Wealth Nexus Debasis Barik Associate Fellow National Council of Applied Economic Research [email protected] Sonalde Desai Professor of Sociology, University of Maryland College Park And Senior Fellow, National Council of Applied Economic Research [email protected] Reeve Vanneman Professor of Sociology, University of Maryland College Park [email protected] February 26, 2016 India Human Development Survey was funded by grants R01HD041455 and R01HD061048 from the US National Institutes of Health and a supplementary grant from the Ford Foundation. Data analysis was the funded by the UK government as part of its Knowledge Partnership Programme (KPP). PAA 2016 | Session 58 Adult Mortality in India: The Health–Wealth Nexus Debasis Barik, Sonalde Desai, Reeve Vanneman Abstract Research on wealth and adult mortality is often stymied by the reciprocity of this relationship. While financial resources increase access to healthcare and nutrition and reduce mortality, sickness also reduces labor force participation, thereby reducing income. Without longitudinal data, it is difficult to study the linkage between economic status and mortality. Using data from a national sample of 133,379 comprising Indian adults aged 15 years and above, this paper examines their likelihood of death between wave 1 of the India Human Development Survey (IHDS), conducted in 2004-05 and wave 2, conducted in 2011- 12. The results show that mortality between the two waves is strongly linked to the economic status of the household at wave 1. Household wealth is positively associated with the manifestation of hypertension, diabetes and cardiac conditions, but wealth also reduces the likelihood of death conditional on having these diseases. -

The G.N.A. University Act, 2014
The G.N.A. University Act, 2014 Act 17 of 2014 Keyword(s): Trust, Campuses, Dean, Institution, Society, Visitor DISCLAIMER: This document is being furnished to you for your information by PRS Legislative Research (PRS). The contents of this document have been obtained from sources PRS believes to be reliable. These contents have not been independently verified, and PRS makes no representation or warranty as to the accuracy, completeness or correctness. In some cases the Principal Act and/or Amendment Act may not be available. Principal Acts may or may not include subsequent amendments. For authoritative text, please contact the relevant state department concerned or refer to the latest government publication or the gazette notification. Any person using this material should take their own professional and legal advice before acting on any information contained in this document. PRS or any persons connected with it do not accept any liability arising from the use of this document. PRS or any persons connected with it shall not be in any way responsible for any loss, damage, or distress to any person on account of any action taken or not taken on the basis of this document. PUNJAB GOVT. GAZ. (EXTRA), AUGUST 21, 2014 83 (SRVN 30, 1936 SAKA) PART I GOVERNMENT OF PUNJAB DEPARTMENT OF LEGAL AND LEGISLATIVE AFFAIRS, PUNJAB NOTIFICATION The 21st August, 2014 No. 18-Leg./2014.-The following Act of the Legislature of the State of Punjab received the assent of the Governor of Punjab on the 14th Day of August, 2014, is hereby published for general information:- THE G.N.A. -

House Number 2 Street/ Village 3 Tehsil 4 District
Ministry of Health and Family Welfare Government of India SELF REPORTING FORM to BE FILLED BY ALL INTERNATIONAL PASSENGERS (TO BE PRESENTED AT THE HEALTH/IMMIGRATION COUNTER) All persons coming to India are required to fill-up this proforma in duplicate and submit a copy each to health and immigration counter. Personal Information Contact Address in India for All Travellers: 1 Name of House Number the passenger 2 Street/ Village Seat No. 3. Flight No. 3 Tehsil 4 Passport 4 District/ City No. 5 Date of 5 State Arrival 6 Pin 6 Port of 7 Residence Number origin of Journey 8 Mobile Number 7 Port of 9 E mail ID final destination (PART-A) a. Details of the cities/ countries visited since last 28 days?________________________ b. Are you suffering from any of the following symptoms** Fever Yes No Cough Yes No Respiratory distress Yes No For persons having travel history to china, Hong Kong, Republic of Korea, Italy, Iran, Japan and other Covid-19 affected countries* or contacts with people having such history are requested to undergo mandatory thermal screening at the Health Counters Signature of the passenger *CHINA, AS NOTIFIED BY W.H.O FOR LOCAL TRANSMISSION (https://www.who.int/emergencies/diseases/novel- coronavirus- 2019/situation-reports/) **If answer to any of the above questions is “yes”, please present yourself to the Airport Health counter for preliminary screening. In case you develop symptoms such as fever and cough within 28 days of leaving this airport, restrict your outdoor movement and contact MoHFW’s 24 hours helpline number 011-23978046. -

Constitution of Pakistan Badminton Federation
CONSTITUTION OF PAKISTAN BADMINTON FEDERATION 1. TITLE: This document shall be called the Constitution of the Pakistan Badminton Federation, hereafter called PBF/ Federation. 2. JURISDICTION: i. The area of its operation shall extend to the whole of Pakistan, the acceding States and Territories under the control of Pakistan. It shall have the exclusive rights to govern Badminton for men and women in Pakistan. ii. PBF declares its opposition to any discrimination on the grounds of politics, race, sex, religion and creed. 3. DEFINITIONS: In this Constitution as well as the rules and bye-laws made under it, unless there is anything repugnant in the subject or context, the following definition are offered:- i. Clubs will be based on area basis and will form part of one Tehsil/equivalent administrative areas in the country. The criteria for registration of a club will be enunciated by PBF. It must have atleast 8 players. The club, in a Tehsil may register itself Tehsil Badminton Association and the Sports Officer of the Provincial Government deputed in Tehsil/equivalent administrative area. ii. Tehsil Badminton Association means the association formed through clubs in its administration areas and affiliated to District Badminton Association. It must have 10 active playing clubs under its jurisdiction. iii. District Badminton Association means the Sports Association of a district affiliated to Provincial Badminton Association and continuing to be so by observing all the conditions and requirements laid down by that Provincial Association. It must have atleast two active playing Tehsils under its jurisdictions. iv. “Provincial Association” means the Provincial Badminton Association. v. -
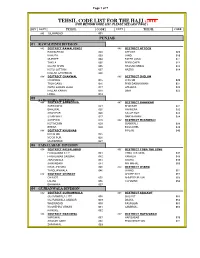
Tehsil Code List 2014
Page 1 of 7 TEHSIL CODE LIST FOR THE HAJJ -2016 (FOR MEHRAM CODE LIST, PLEASE SEE LAST PAGE ) DIV DISTT TEHSIL CODE DISTT TEHSIL CODE 001 ISLAMABAD 001 PUNJAB 01 RAWALPINDI DIVISION 002 DISTRICT RAWALPINDI 003 DISTRICT ATTOCK RAWALPINDI 002 ATTOCK 009 KAHUTA 003 JAND 010 MURREE 004 FATEH JANG 011 TAXILA 005 PINDI GHEB 012 GUJAR KHAN 006 HASSAN ABDAL 013 KOTLI SATTIAN 007 HAZRO 014 KALLAR SAYYEDAN 008 004 DISTRICT CHAKWAL 005 DISTRICT JHELUM CHAKWAL 015 JHELUM 020 TALA GANG 016 PIND DADAN KHAN 021 CHOA SAIDAN SHAH 017 SOHAWA 022 KALLAR KAHAR 018 DINA 023 LAWA 019 02 SARGODHA DIVISION 006 DISTRICT SARGODHA 007 DISTRICT BHAKKAR SARGODHA 024 BHAKKAR 031 BHALWAL 025 MANKERA 032 SHAH PUR 026 KALUR KOT 033 SILAN WALI 027 DARYA KHAN 034 SAHIEWAL 028 009 DISTRICT MIANWALI KOT MOMIN 029 MIANWALI 038 BHERA 030 ESSA KHEL 039 008 DISTRICT KHUSHAB PIPLAN 040 KHUSHAB 035 NOOR PUR 036 QUAIDABAD 037 03 FAISALABAD DIVISION 010 DISTRICT FAISALABAD 011 DISTRICT TOBA TEK SING FAISALABAD CITY 041 TOBA TEK SING 047 FAISALABAD SADDAR 042 KAMALIA 048 JARANWALA 043 GOJRA 049 SAMUNDARI 044 PIR MAHAL 050 CHAK JHUMRA 045 012 DISTRICT JHANG TANDLIANWALA 046 JHANG 051 013 DISTRICT CHINIOT SHORE KOT 052 CHINIOT 055 AHMEDPUR SIAL 053 LALIAN 056 18-HAZARI 054 BHAWANA 057 04 GUJRANWALA DIVISION 014 DISTRICT GUJRANWALA 015 DISTRICT SIALKOT GUJRANWALA CITY 058 SIALKOT 063 GUJRANWALA SADDAR 059 DASKA 064 WAZIRABAD 060 PASROOR 065 NOSHEHRA VIRKAN 061 SAMBRIAL 066 KAMOKE 062 016 DISTRICT NAROWAL 017 DISTRICT HAFIZABAD NAROWAL 067 HAFIZABAD 070 SHAKAR GARH 068 PINDI BHATTIAN -

BTS Site Tehsil District Region Code Islamabad / Rwp Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7100000 7109999 Islamabad / Rwp I
GREAT BEAR BTS Site Tehsil District Region Code Numbers Islamabad / Rwp Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7100000 7109999 Islamabad / Rwp Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7110000 7119999 London Shopping center G-9 Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7120000 7120999 Al Farooq plaza G-10 Markaz Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7121000 7121999 Sardar arcade F-11 Markaz Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7122000 7122999 Plot 247 sector I-9/2 Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7123000 7123999 Mandeer palace I-10 Markaz Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7124000 7124999 Laraib plaza I-8 Markaz Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7125000 7125999 Al hayat plaza, 12-B Rawalpindi Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7126000 7126999 Al badar hotel, plot 12 Rawalpindi. Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7127000 7127999 Kiyani plaza scheme 3 rawalpindi Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7128000 7128999 Zaki plaza Rawalpindi-II Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7129000 7129999 Hasnain plaza Islamabad Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7130000 7130999 Khan plaza peshawar road Rawalpindi. Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7131000 7131999 B-335, bakra mandi Rawalpindi cantt. Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7132000 7132999 Al shifa plaza 6th road Rawaplindi. Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7133000 7133999 NTC exchange Pirwadhi Islamabad / Rwp Islamabad/ Rwp ITR/RTR 51 7134000 7134999 Chaudhri Mohammad colony Rawalpindi Islamabad / Rwp