Shoulder Pain Review of Physical Exam and an Approach to the Differential Diagnosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Sprain a Sprain Is a Stretch And/Or Tear of a Ligament, a Strong Band of Connective Tissue That Connect the End of One Bone with Another
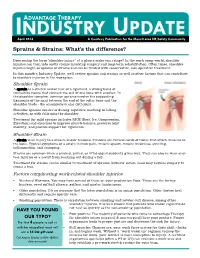
INDUSTRYADVANTAGE THERAPY UPDATE April 2016 A Courtesy Publication for the Monett area HR/Safety Community Sprains & Strains: What’s the difference? Does seeing the term “shoulder injury” at a glance make you cringe? In the work comp world, shoulder injuries can turn into costly claims involving surgery and long-term rehabilitation. Often times, shoulder injuries begin as sprains or strains and can be treated with conservative, non-operative treatment. In this month’s Industry Update, we’ll review sprains and strains as well as other factors that can contribute to shoulder injuries in the workplace. Shoulder Sprain A sprain is a stretch and/or tear of a ligament, a strong band of connective tissue that connect the end of one bone with another. In the shoulder complex, common sprains involve the supporting ligaments of the joint between the end of the collar bone and the shoulder blade - the acromioclavicular (AC) joint. Shoulder sprains can occur during repetitive reaching or lifting activities, or with falls onto the shoulder. Treatment for mild sprains includes RICE (Rest, Ice, Compression, Elevation) and exercises to improve muscle balance, preserve joint mobility, and provide support for ligaments. Shoulder Strain A strain is an injury to a muscle and/or tendons. Tendons are fibrous cords of tissue that attach muscles to the bone. Typical symptoms of a strain include pain, muscle spasm, muscle weakness, swelling, inflammation, and cramping. Strains are common when a pushed, pulled, or lifted object suddenly gives way. They can also be wear-and- tear injuries or a result from reaching out during a fall. -

Wrist Fracture – Advice Following Removal of Your Cast
Wrist Fracture – advice following removal of your cast A plaster cast usually prevents a fracture from moving, but allows your fingers to move. The cast also reduces pain. What to expect It usually takes four to six weeks for new bone to form to heal your fracture. When the cast is removed most people find that their wrist is stiff, weak and uncomfortable to start with. It may also be prone to swelling and the skin dry or flaky, this is quite normal. It is normal to get some pain after your fracture. If you need painkillers you should take them as prescribed as this will allow you to do your exercises and use your wrist for light activities. You can ask a Pharmacist about over the counter painkillers. If your pain is severe, continuous or excessive you should contact your GP. The new bone gradually matures and becomes stronger over the next few months. It is likely to be tender and may hurt if you bang it. The muscles will be weak initially, but they should gradually build up as you start to use your hand and wrist. When can I start to use my hand and wrist? It is important to try and use your hand and wrist as normally as possible. Start with light activities like fastening buttons, washing your face, eating, turning the pages of books over etc. Build up as pain allows. Avoid lifting a kettle for 4 weeks If I have been given a Wrist splint You may have been given a wrist splint to wear. -

Juvenile Spondyloarthropathies: Inflammation in Disguise
PP.qxd:06/15-2 Ped Perspectives 7/25/08 10:49 AM Page 2 APEDIATRIC Volume 17, Number 2 2008 Juvenile Spondyloarthropathieserspective Inflammation in DisguiseP by Evren Akin, M.D. The spondyloarthropathies are a group of inflammatory conditions that involve the spine (sacroiliitis and spondylitis), joints (asymmetric peripheral Case Study arthropathy) and tendons (enthesopathy). The clinical subsets of spondyloarthropathies constitute a wide spectrum, including: • Ankylosing spondylitis What does spondyloarthropathy • Psoriatic arthritis look like in a child? • Reactive arthritis • Inflammatory bowel disease associated with arthritis A 12-year-old boy is actively involved in sports. • Undifferentiated sacroiliitis When his right toe starts to hurt, overuse injury is Depending on the subtype, extra-articular manifestations might involve the eyes, thought to be the cause. The right toe eventually skin, lungs, gastrointestinal tract and heart. The most commonly accepted swells up, and he is referred to a rheumatologist to classification criteria for spondyloarthropathies are from the European evaluate for possible gout. Over the next few Spondyloarthropathy Study Group (ESSG). See Table 1. weeks, his right knee begins hurting as well. At the rheumatologist’s office, arthritis of the right second The juvenile spondyloarthropathies — which are the focus of this article — toe and the right knee is noted. Family history is might be defined as any spondyloarthropathy subtype that is diagnosed before remarkable for back stiffness in the father, which is age 17. It should be noted, however, that adult and juvenile spondyloar- reported as “due to sports participation.” thropathies exist on a continuum. In other words, many children diagnosed with a type of juvenile spondyloarthropathy will eventually fulfill criteria for Antinuclear antibody (ANA) and rheumatoid factor adult spondyloarthropathy. -
The 7 Step Shin Splints Treatment System
The Step SShhiinn SSpplliinnttss Treatment System By Brad Walker TM The 7 Step Shin Splints Treatment System Fix Your Shin Splints Once and For All and get back to Pain Free Running Quickly and Safely. Walker, Bradley E., 1971 7 Step Shin Splints Treatment System™ Copyright © 2012 The Stretching Institute™ All rights reserved. Except under conditions described in the copyright act, no part of this publication may in any form or by any means (electronic, mechanical, micro copying, photocopying, recording or otherwise) be reproduced, stored in a retrieval system or transmitted without prior written permission from the copyright owner. Inquires should be addressed to the publisher. Disclaimers The exercises presented in this publication are intended as an educational resource and are not intended as a substitute for proper medical advice. Please consult your physician, physical therapist or sports coach before performing any of the exercises described in this publication, particularly if you are pregnant, elderly or have any chronic or recurring muscle or joint pain. Discontinue any exercise that causes you pain or severe discomfort and consult a medical expert. Cover picture/s supplied by iStockphoto. The Stretching Institute has purchased the non-exclusive, non-transferable, non-sub licensable right to reproduce the cover picture/s an unlimited number of times in online and electronic publications, and web advertisements. Exercise graphics used with permission from the Physigraphe V2 Pro Clip Art CD-ROM available at ExRx.net. Copyright -
Shoulder Instability, Impingement, and the Rotator Cuff
Shoulder Instability, Impingement, and the Rotator Cuff TOM BUSH DNP, FNP-BC, FAANP CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL SCHOOLS OF NURSING AND MEDICINE Objectives • Recognize signs and symptoms of common shoulder disorders • Demonstrate provocative maneuvers for diagnosis of specific conditions • Formulate management strategies for common disorders • Identify conditions that require collaboration and consultation Orthopedics and Sports Medicine Bush Stock Photo Orthopedics and Sports Medicine Bush Stock Photo Sherman, 2016 Sherman, 2016 Sherman, 2016 Shoulder Overview •Chronicity (acute injury Vs insidious onset) •Chief complaint (pain/motion/instability) •Patient age •Age and chief complaint are most valuable predictors in primary care setting •Most disorders can be diagnosed by history, exam and plain radiographs Age Is Key Variable •Younger than 30 likely to report symptoms of instability from dislocation/subluxation of glenohumeral joint or AC joint •Middle-aged (30-50) more commonly report impingement. Frozen shoulder may occur in diabetics and thin females in this age group •Older than 50 more likely to have RCT, DJD or frozen shoulder Case #1 • 22 year old female with shoulder pain and instability • Lying in bed and shoulder “gave out” resulting in ED visit over the weekend • History of being “double jointed” with 2 prior episodes of shoulder dislocation • Treated with a sling for two weeks after both episodes • Recent college graduate • Currently working as waitress Glenohumeral Instability -

Musculoskeletal Ultrasound Technical Guidelines II. Elbow
European Society of MusculoSkeletal Radiology Musculoskeletal Ultrasound Technical Guidelines II. Elbow Ian Beggs, UK Stefano Bianchi, Switzerland Angel Bueno, Spain Michel Cohen, France Michel Court-Payen, Denmark Andrew Grainger, UK Franz Kainberger, Austria Andrea Klauser, Austria Carlo Martinoli, Italy Eugene McNally, UK Philip J. O’Connor, UK Philippe Peetrons, Belgium Monique Reijnierse, The Netherlands Philipp Remplik, Germany Enzo Silvestri, Italy Elbow Note The systematic scanning technique described below is only theoretical, considering the fact that the examination of the elbow is, for the most, focused to one quadrant only of the joint based on clinical findings. 1 ANTERIOR ELBOW For examination of the anterior elbow, the patient is seated facing the examiner with the elbow in an extension position over the table. The patient is asked to extend the elbow and supinate the fore- arm. A slight bending of the patient’s body toward the examined side makes full supination and as- sessment of the anterior compartment easier. Full elbow extension can be obtained by placing a pillow under the joint. Transverse US images are first obtained by sweeping the probe from approximately 5cm above to 5cm below the trochlea-ulna joint, a Pr perpendicular to the humeral shaft. Cranial US images of the supracondylar region reveal the superficial biceps and the deep brachialis mu- Br scles. Alongside and medial to these muscles, follow the brachial artery and the median nerve: * the nerve lies medially to the artery. * Legend: a, brachial artery; arrow, median nerve; arrowheads, distal biceps tendon; asterisks, articular cartilage of the Humerus humeral trochlea; Br, brachialis muscle; Pr, pronator muscle 2 distal biceps tendon: technique The distal biceps tendon is examined while keeping the patient’s forearm in maximal supination to bring the tendon insertion on the radial tuberosity into view. -

Complex Regional Pain Syndrome Type I (Shoulder-Hand Syndrome) in an Elderly Patient After Open Cardiac Surgical Intervention; a Case Report
Eastern Journal of Medicine 16 (2011) 56-58 L. Ediz et al / CRPS type I after open cardiac Surgery Case Report Complex regional pain syndrome type I (shoulder-hand syndrome) in an elderly patient after open cardiac surgical intervention; a case report Levent Ediza*, Mehmet Fethi Ceylanb , Özcan Hıza, İbrahim Tekeoğlu c a Department of Physical Medicine and Rehabilitation, Yüzüncü Yıl University Medical Faculty, Van, Turkey b Department of Orthopaedics and Traumatology,Yüzüncü Yıl University Medical Faculty, Van, Turkey c Department of Rheumatology, Yüzüncü Yıl University Medical Faculty, Van, Turkey Abstract. We described the first case report in the literature who developed Complex Regional Pain Syndrome (CRPS type I) symptoms in his right shoulder and right hand within 15 days after open cardiac surgery and discussed shoulder-hand syndrome (CRPS type I) and frozen shoulder diagnosis along with the reasons of no report of CRPS type I in these patients. We also speculated whether frozen shoulder seen in postthoracotomy and postcardiac surgery patients might be CRPS type I in fact. Key words: Complex regional pain syndrome, cardiac surgery, frozen shoulder 1. Introduction Improper patient positioning, muscle division, perioperative nerve injury, rib spreading, and Complex Regional Pain Syndrome (CRPS) is consequent postoperative pain influence the complication of injuries which is seen at the patient's postoperative shoulder function and distal end of the affected area characterized by quality of life (5). In a study Tuten HR et al pain, allodyni, hyperalgesia, edema, abnormal retrospectively evaluated for the incidence of vasomotor and sudomotor activity, movement adhesive capsulitis of the shoulder of two disorders, joint stiffness, regional osteopenia, and hundred fourteen consecutive male cardiac dystrophic changes in soft tissue (1,2). -

Bursae Around the Knee Joints Priyank S Chatra Department of Radiology, Yenepoya Medical College, Mangalore, Karnataka, India
MUSCULOSKELETAL RADIOLOGY Bursae around the knee joints Priyank S Chatra Department of Radiology, Yenepoya Medical College, Mangalore, Karnataka, India Correspondence: Dr. Priyank S. Chatra, Department of Radiology, Yenepoya Medical College, Deralakatte, Mangalore – 575 018, Karnataka, India. E-mail: [email protected] Abstract A bursa is a fluid-filled structure that is present between the skin and tendon or tendon and bone. The main function of a bursa is to reduce friction between adjacent moving structures. Bursae around the knee can be classified as those around the patella and those that occur elsewhere. In this pictorial essay we describe the most commonly encountered lesions and their MRI appearance. Key words: Iliotibial bursa; infrapatellar bursa; pes anserine bursa Introduction and the gastrocnemius-semimembranosus bursa. On MRI imaging, bursitis appears as an oblong fluid collection in A bursa is a fluid-filled structure that is present between its expected anatomical location. the skin and tendon or tendon and bone. The main function of a bursa is to reduce friction between adjacent Prepatellar Bursitis moving structures. Typically, bursae are located around large joints such as the shoulder, knee, hip, and elbow.[1] The prepatellar bursa is located between the patella and the Inflammation of this fluid-filled structure is called bursitis. overlying subcutaneous tissue. Chronic trauma in the form Trauma, infection, overuse, and hemorrhage are some of prolonged or repeated kneeling leads to inflammation of the common -

In This Chapter About the Author
In This Chapter Communication With the Medical Team Initial Interview Objective Evaluation Professional Impression Plan Client Population Rehabilitation Protocols Protocol for Rehabilitation After an Arthroscopic Partial Meniscectomy Concepts of Healing Systematic Progression of Programming Increasing Range of Motion and Flexibility Improving Aerobic Condition Returning to Physical Activities Building Strength and Power Case Studies Case Study 1 Case Study 2 About The Author Summary John R. Martínez, P.T., M.P.T., is the owner and president of Executive Operations Management, L.L.C., a medical consulting firm, and Physical Therapy Experts, P.L.L.C., a private medical practice, both in New York City. He is a teacher of neurology, anatomy, and physiology to undergraduate students in Manhattan. Martinez received his Bachelor of Arts and teaching certification in 1988 from Swarthmore College and has taught elementary through graduate school students and a variety of topics in science, recreation, wellness, and exercise. In 1997, Martinez received his Bachelor of Science and Master of Physical Therapy degrees from the Philadelphia College of Pharmacy and Science. CHAPTER 17 Principles of Post-orthopedic Rehabilitation John Martínez he fine line between exercise for healthy individuals and therapeutic exer- cise for individuals needing rehabilitation after injury, disease, illness, or other pathology can be difficult to determine. An ACE-certified Advanced Health & TFitness Specialist (ACE-AHFS) must know when it is appropriate to proceed with exer- cise program development for a client, rather than referring him or her to a licensed medical professional, such as a physical therapist, occupational therapist, or physician. Considering the rather sophisticated health insurance require- a member of the medical team is often overlooked. -

'Dialysis Related Arthropathy': a Survey of 95 Patients Receiving Chronic Haemodialysis with Special Reference to 132 Microglobulin Related Amyloidosis
Ann Rheum Dis: first published as 10.1136/ard.48.5.409 on 1 May 1989. Downloaded from Annals of the Rheumatic Diseases, 1989; 48, 409-420 'Dialysis related arthropathy': a survey of 95 patients receiving chronic haemodialysis with special reference to 132 microglobulin related amyloidosis N P HURST,' R VAN DEN BERG,' A DISNEY,2 M ALCOCK,3 L ALBERTYN,3 M GREEN,' AND V PASCOE4 From the 'Rheumatology Unit, the 2Renal Unit, the 3Department of Radiology, and the 4Department of Pathology, The Queen Elizabeth Hospital, Woodville, South Australia SUMMARY Ninety five patients receiving chronic haemodialysis (CHD) were surveyed to determine the prevalence of rheumatic disease and, where possible, its aetiology. At least three distinct rheumatic syndromes were identified-a group of patients with a syndrome consisting of large and medium joint synovial swelling, restricted hips and shoulders, tenosynovitis, carpal tunnel syndrome, and bone cysts due to deposition of 132 microglobulin related amyloid (AMP2m); a second group with erosive azotaemic osteoarthropathy; and a third group with age related degenerative disease of small, large, and axial joints. The data presented suggest that in patients receiving CHD (a) the prevalence of AM2i2m deposition and the associated syndrome increases with duration of dialysis, but in patients who have been dialysed for more than 10 years the risk of developing AM2n2m is related to age; (b) AM2i2m deposition in subchondral cysts, but not synovium, causes joint destruction; also, AMp2m may be more prone to deposition in synovium of joints already damaged by other processes; (c) in the absence of synovial iron deposition synovial AM2n2m is not associated with an inflammatory infiltrate; (d) hyperparathyroidism and perhaps other factors such as synovial iron deposition are probably more important than AMgi2m as causes http://ard.bmj.com/ of peripheral joint degeneration and destructive spondyloarthropathy in patients receiving CHD. -

Wrist Fracture
Hand Conditions: WRIST FRACTURE A wrist fracture is a break in one or more of the bones in the wrist. The wrist is made up of the two bones in the forearm called the radius and the ulna. It also includes eight carpal bones. The carpal bones lie between the end of the forearm bones and the bases of the fi ngers. The most commonly fractured carpal bone is called the scaphoid or navicular bone. This fact sheet will focus on fractures of the carpal bones of the wrist. Causes A wrist fracture is caused by trauma to the bones in the wrist. Trauma may be caused by: • Falling on an outstretched arm • Direct blow to the wrist • Severe twist of the wrist Risk Factors Factors that increase your chance of developing a wrist fracture include: • Participating in contact sports, such as football or soccer • Participating in activities such as in-line skating, skateboarding, or bike riding • Participating in any activity which could cause you to fall on your outstretched hand • Violence or high-velocity trauma, such as an automobile accident Symptoms If you have any of these symptoms, do not assume they are due to a wrist fracture. Symptoms of a wrist fracture include. • Pain • Swelling and tenderness around the wrist • Bruising around the wrist • Limited range of wrist or thumb motion • Visible deformity in the wrist For more information visit us online at www.ptandme.com Hand Conditions: WRIST FRACTURE Diagnosis Your doctor will ask about your symptoms, physical activity, and how the injury occurred. The injured area will be examined. -

Extended Insertion of Teres Minor Muscle: a Rare Case Report
Eur J Anat, 16 (3): 224-225 (2012) CASE REPORT Extended insertion of teres minor muscle: a rare case report Monica Jain, Lovesh Shukla, Dalbir Kaur Maharaja Agrasen Medical College, Agroha-125047, Hisar, Haryana, India SUMMARY upwards and laterally, and gets inserted on the lowest of the three impressions on the greater Teres minor is one of the muscles of the shoul- tubercle of the humerus and fuses with the der joint along with subscapularis, supraspina- capsule of the shoulder joint along with other tus and infraspinatus forming rotator cuff. muscles forming the rotator cuff. It is inner- Variations of teres minor are relatively uncom- vated by the posterior branch of the axillary mon. A unique and extended insertion of this nerve. It stabilizes the humerus by holding muscle is being reported in the present case. the humeral head in the glenoid cavity of the Knowledge of the anatomy of this muscle is scapula, a and causes lateral rotation of the important to avoid injury to the axillary nerve arm (Johnson, 2008). Variations of teres and posterior circumflex humeral vessels while minor are relatively uncommon and have been surgically approaching the shoulder joint and occasionally reported by various authors inserting portals of the arthroscope in a poste- (Bergman et al., 2006). rior approach to the shoulder joint. Key words: Teres minor – Rotator cuff – CASE REPORT Shoulder joint – Capsule of shoulder joint – Humerus – Surgical neck of humerus During routine dissection of the shoulder region of upper limb of an approximately 50 year-old male cadaver for undergraduate teach- INTRODUCTION ing and training, a unique and extended inser- tion of the teres minor muscle was found on the Teres minor is a one of the short scapular right side.