Anterior Transorbital Meningoencephaloceles: a Defect in the Pars Orbitalis of the Frontal Bone
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Decompressive Craniectomy Following Severe Traumatic Brain Injury with an Initial Glasgow Coma Scale Score of 3 Or 4
Case Report Clinics in Surgery Published: 03 Jul, 2019 Decompressive Craniectomy Following Severe Traumatic Brain Injury with an Initial Glasgow Coma Scale Score of 3 or 4 Afif AFIF* Department of Neurosurgery and Anatomy, Pierre Wertheimer Hospital, France Abstract Background: Decompressive craniectomy is a surgical management option for severe Traumatic Brain Injury (TBI). However, few studies have followed patients with TBI who have a Glasgow Coma Scale (GCS) score of 3 or 4 (out of 15). Decompressive craniectomy has been avoided in such patients owing to poor outcomes and poor functional recoveries in previous cases of treatment using this method. Clinical Presentation: Two patients are presented in our case series. The first suffered severe TBI following an aggression, with a GCS score of 3 and bilaterally dilated unreactive pupils. Brains CT scan showed right frontal fracture, bifrontal hematoma contusion, a fronto-temporo-parietal acute Subdural Hematoma (SDH) with a thickness of 14 mm on the right side, traumatic subarachnoid hemorrhage, with 20 mm of midline shift to the left side, and diffuses brain edema. The second presented with severe TBI following an automobile accident, with a GCS score of 4 and iso- reactive pupils. A brain CT scan showed bilateral fronto-temporal fracture, diffuse brain hematoma contusion, traumatic subarachnoid hemorrhage, right Extradural Hematoma (EDH) and bilateral fronto-temporo-parietal acute SDH that was more pronounced on the right side. Conclusion: Follow-up after the operations showed an Extended Glasgow Outcome Scale (EGOS) score of 8 and a very good functional recovery for both patients. Our case series suggests that in patients with severe TBI and a GCS score of 3 or 4; decompressive craniectomy can be performed OPEN ACCESS with good long-term neurological outcomes. -

Cranioplasty: Indications, Procedures, and Outcome – an Institutional Experience Syed M
OPEN ACCESS Editor: James I. Ausman, MD, PhD For entire Editorial Board visit : University of California, Los http://www.surgicalneurologyint.com Angeles, CA, USA SNI: General Neurosurgery Original Article Cranioplasty: Indications, procedures, and outcome – An institutional experience Syed M. Andrabi, Arif H. Sarmast, Altaf R. Kirmani, Abdul R. Bhat Department of Neurosurgery, Sher I Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir, India E‑mail: Syed M. Andrabi ‑ [email protected]; *Arif H. Sarmast ‑ [email protected]; Altaf R. Kirmani ‑ [email protected]; Abdul R. Bhat ‑ [email protected] *Corresponding author Received: 27 January 17 Accepted: 16 March 17 Published: 26 May 17 Abstract Background: Cranioplasty, the repair of a skull vault defect by insertion of an object (bone or nonbiological materials such as metal or plastic plates), is a well‑known procedure in modern neurosurgery. Brain protection and cosmetic aspects are the major indications of cranioplasty. A retroprospective study was conducted for evaluating the indications, materials used, complications, and outcome of cranioplasty. Methods: This study was prospective from August 2013 to September 2015 and retrospective from August 2010 to July 2013. In the retrospective study, patients files were retrieved from the mentioned date (August 2010 to July 2013) from the medical records and the findings were recorded. Abstracted data included age at the time of cranioplasty (years), sex (male or female), medical comorbidities (hypertension, -

Case Series Sinking Skin Flap Syndrome Following Posttraumatic Hydrocephalus
Hindawi Case Reports in Neurological Medicine Volume 2021, Article ID 6682310, 8 pages https://doi.org/10.1155/2021/6682310 Case Series Sinking Skin Flap Syndrome following Posttraumatic Hydrocephalus Ashish Chugh, Prashant Punia , and Sarang Gotecha Dr. D. Y. Patil Medical College and Hospital, Pimpri, Pune, Maharashtra, India Correspondence should be addressed to Prashant Punia; [email protected] Received 21 November 2020; Revised 8 January 2021; Accepted 11 January 2021; Published 9 February 2021 Academic Editor: Tapas Kumar Banerjee Copyright © 2021 Ashish Chugh et al. (is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Introduction. Complications following craniotomy are not uncommon and Sinking Skin Flap Syndrome (SSFS) constitutes a rare entity that may present after a large Decompressive Craniectomy. Although the entity is widely reported, the literature mostly consists of case reports. Authors present a case series of three patients with review of literature highlighting the various factors which can prove therapeutic and can help in avoidance of complications. Materials and Methods. (e study was conducted over a period of 3 years, from 2016 to 2019, and included 212 patients who underwent unilateral Decompressive Craniectomy (DC) for trauma in our institute. All 212 patients underwent a similar DC following a strict institutional protocol and the craniectomies were performed by the same surgical team. At total of 160 patients survived and elective cranioplasty was planned at a 3-month interval. Out of a total of 160 patients who survived, 38 developed hydrocephalus, 3 patients presented with hydrocephalus acutely and had to be shunted before cranioplasty and underwent ventriculoperitoneal (VP) shunting on the opposite side of craniectomy. -

Cosmetic Outcome of Cranioplasty After Decompressive Craniectomy—An Overlooked Aspect
Original Article Cosmetic Outcome of Cranioplasty After Decompressive Craniectomy—An Overlooked Aspect Diptiranjan Satapathy1, Mohammed Nadeem1, Dhaval P. Shukla2, A.R. Prabhuraj1, Bhagavatula Indira Devi2 - BACKGROUND: Cranioplasty (CP) is an obligatory surgery INTRODUCTION after decompressive craniectomy (DC). The primary objective ecompressive craniectomy (DC) is a rescue measure for is to protect the brain from external injury and prevent syn- treatment of raised intracranial pressure resulting from drome of trephined. In a government hospital, such cases D malignant cerebral edema due to acquired brain injury.1,2 pose a significant burden to a trauma center. Because of this DC is a life-saving surgery, and survivors require a cranioplasty reason, cosmetic outcome is never taken into account for the (CP) to cover the defect produced by the DC. The CP is an CP. We present results of CP performed at our hospital. obligatory surgery after DC. The indications of CP are recon- struction and protection, cosmesis, prevention and treatment of - METHODS: This is a retrospective review of the cases of the syndrome of trephined, and possible neurologic recovery.3 CP performed over the past 3 years at our hospital. The Major concerns before considering CP are residual brain cosmetic outcome was divided into 3 grades: 1—good sym- swelling, risk of infection, and hydrocephalus.4,5 In a metrical, 2—irregularities, 2a—elevated and 2b depressed, high-volume government hospital, such cases pose a burden on and 3—bad cosmetic outcome requiring reoperation. the existing waiting list of patients who require surgery for life-threatening neurosurgical disorders. Because of this reason, - RESULTS: A total of 133 patients with acute brain injury cosmetic outcome after the CP was formerly of minor concern. -

Gross and Micro-Anatomical Study of the Cavernous Segment of the Abducens Nerve and Its Relationships to Internal Carotid Plexus: Application to Skull Base Surgery
brain sciences Article Gross and Micro-Anatomical Study of the Cavernous Segment of the Abducens Nerve and Its Relationships to Internal Carotid Plexus: Application to Skull Base Surgery Grzegorz Wysiadecki 1,* , Maciej Radek 2 , R. Shane Tubbs 3,4,5,6,7 , Joe Iwanaga 3,5,8 , Jerzy Walocha 9 , Piotr Brzezi ´nski 10 and Michał Polguj 1 1 Department of Normal and Clinical Anatomy, Chair of Anatomy and Histology, Medical University of Lodz, ul. Zeligowskiego˙ 7/9, 90-752 Łód´z,Poland; [email protected] 2 Department of Neurosurgery, Spine and Peripheral Nerve Surgery, Medical University of Lodz, University Hospital WAM-CSW, 90-549 Łód´z,Poland; [email protected] 3 Department of Neurosurgery, Tulane Center for Clinical Neurosciences, Tulane University School of Medicine, New Orleans, LA 70112, USA; [email protected] (R.S.T.); [email protected] (J.I.) 4 Department of Neurosurgery and Ochsner Neuroscience Institute, Ochsner Health System, New Orleans, LA 70433, USA 5 Department of Neurology, Tulane Center for Clinical Neurosciences, Tulane University School of Medicine, New Orleans, LA 70112, USA 6 Department of Anatomical Sciences, St. George’s University, Grenada FZ 818, West Indies 7 Department of Surgery, Tulane University School of Medicine, New Orleans, LA 70112, USA 8 Department of Anatomy, Kurume University School of Medicine, 67 Asahi-machi, Kurume, Fukuoka 830-0011, Japan Citation: Wysiadecki, G.; Radek, M.; 9 Department of Anatomy, Jagiellonian University Medical College, 33-332 Kraków, Poland; Tubbs, R.S.; Iwanaga, J.; Walocha, J.; [email protected] Brzezi´nski,P.; Polguj, M. -

Entrapment Neuropathy of the Central Nervous System. Part II. Cranial
Entrapment neuropathy of the Cranial nerves central nervous system. Part II. Cranial nerves 1-IV, VI-VIII, XII HAROLD I. MAGOUN, D.O., F.A.A.O. Denver, Colorado This article, the second in a series, significance because of possible embarrassment considers specific examples of by adjacent structures in that area. The same entrapment neuropathy. It discusses entrapment can occur en route to their desti- nation. sources of malfunction of the olfactory nerves ranging from the The first cranial nerve relatively rare anosmia to the common The olfactory nerves (I) arise from the nasal chronic nasal drip. The frequency of mucosa and send about twenty central proces- ocular defects in the population today ses through the cribriform plate of the ethmoid bone to the inferior surface of the olfactory attests to the vulnerability of the optic bulb. They are concerned only with the sense nerves. Certain areas traversed by of smell. Many normal people have difficulty in each oculomotor nerve are pointed out identifying definite odors although they can as potential trouble spots. It is seen perceive them. This is not of real concern. The how the trochlear nerves are subject total loss of smell, or anosmia, is the significant to tension, pressure, or stress from abnormality. It may be due to a considerable variety of causes from arteriosclerosis to tu- trauma to various bony components morous growths but there is another cause of the skull. Finally, structural which is not usually considered. influences on the abducens, facial, The cribriform plate fits within the ethmoid acoustic, and hypoglossal nerves notch between the orbital plates of the frontal are explored. -
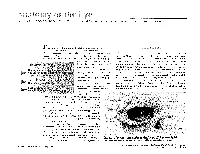
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain. -

98796-Anatomy of the Orbit
Anatomy of the orbit Prof. Pia C Sundgren MD, PhD Department of Diagnostic Radiology, Clinical Sciences, Lund University, Sweden Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lay-out • brief overview of the basic anatomy of the orbit and its structures • the orbit is a complicated structure due to its embryological composition • high number of entities, and diseases due to its composition of ectoderm, surface ectoderm and mesoderm Recommend you to read for more details Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 3 x 3 Imaging technique 3 layers: - neuroectoderm (retina, iris, optic nerve) - surface ectoderm (lens) • CT and / or MR - mesoderm (vascular structures, sclera, choroid) •IOM plane 3 spaces: - pre-septal •thin slices extraconal - post-septal • axial and coronal projections intraconal • CT: soft tissue and bone windows 3 motor nerves: - occulomotor (III) • MR: T1 pre and post, T2, STIR, fat suppression, DWI (?) - trochlear (IV) - abducens (VI) Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Superior orbital fissure • cranial nerves (CN) III, IV, and VI • lacrimal nerve • frontal nerve • nasociliary nerve • orbital branch of middle meningeal artery • recurrent branch of lacrimal artery • superior orbital vein • superior ophthalmic vein Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. -

The Proceedings of the World Neurosurgery Webinar Conference 2020
The Proceedings of the World Neurosurgery Webinar Conference 2020 Editor G Narenthiran FRCS(SN) Neurosurgery Research Listserv The Proceedings of the World Neurosurgery Webinar Conference Abstract 1 [Poster] Xanthogranuloma in the suprasellar region: a case report Mechergui H, Kermani N, Jemel N, Slimen A, Abdelrahmen K, Kallel J Neurosurgical department, National Institute of Neurology of Tunis Contact: [email protected]; Tunisia Conict of interests: none Objective: Xanthogranuloma, also known as cholesterol granuloma, is extremely rare. It represents approximately 1.9% of tumours in the sellar and parasellar region with 83 cases recognised in the literature. The preoperative diagnosis is dicult due to the lack of clinical and radiological specicities. Through this work, we report the third case of xanthogranuloma in the sellar region described in Tunisia. The Proceedings of the World Neurosurgery Webinar Conference Page 1 The Proceedings of the World Neurosurgery Webinar Conference Method: We report the case of 29-year-old girl who was followed up since 2012 for delayed puberty. The patient presented with a 1-year history of decreased visual acuity on the right side. On ophthalmological examination her visual acuity was rated 1/10 with right optic atrophy. Biochemical studies revealed ante-pituitary insuciency. The MRI demonstrated a sellar and suprasellar lesion with solid and cystic components associated with calcication evoking in the rst instance a craniopharyngioma. She underwent a total resection of the tumour by a pterional approach. Result: The anatomopathological examination concluded the lesion to be an intrasellar Xanthogranuloma. Conclusion: Sellar xanthogranuloma is a rare entity that is dicult to diagnose preoperatively due to its similarities with other cystic lesions of the sellar region, especially craniopharyngioma. -

From Decompressive Craniectomy to Cranioplasty and Beyond—A Pediatric Neurosurgery Perspective
Child's Nervous System (2019) 35:1517–1524 https://doi.org/10.1007/s00381-019-04303-z ORIGINAL ARTICLE From decompressive craniectomy to cranioplasty and beyond—a pediatric neurosurgery perspective Thomas Beez1 & Christopher Munoz-Bendix 1 & Sebastian Alexander Ahmadi1 & Hans-Jakob Steiger1 & Kerim Beseoglu1 Received: 23 May 2019 /Accepted: 8 July 2019 /Published online: 20 July 2019 # Springer-Verlag GmbH Germany, part of Springer Nature 2019 Abstract Purpose Decompressive craniectomy (DC) is an established neurosurgical emergency technique. Patient selection, optimal timing, and technical aspects related to DC and subsequent cranioplasty remain subjects of debate. For children, the overall degree of evidence is low, compared with randomized controlled trials (RCTs) in adults. Methods Here, we present a detailed retrospective analysis of pediatric DC, covering the primary procedure and cranioplasty. Results are analyzed and discussed in the light of modern scientific evidence, and conclusions are drawn to stimulate future research. Results The main indication for DC in children is traumatic brain injury (TBI). Primary and secondary DC is performed with similar frequency. Outcome appears to be better than that in adults, although long-term complications (especially bone flap resorption after autologous cranioplasty) are more common in children. Overt clinical signs of cerebral herniation prior to DC are predictors of poor outcome. Conclusions We conclude that DC is an important option in the armamentarium to treat life-threatening intracranial hypertension, but further research is warranted, preferentially in a multicenter prospective registry. Keywords Intracranial hypertension . Cranial reconstruction . Bone flap resorption Background compared with conservative management [4]. Another RCT (DECRA) had a lower ICP threshold (> 20 mmHg) and dem- The appeal of decompressive craniectomy (DC) as a universal onstrated lower mortality but more unfavorable outcomes af- treatment of severely raised intracranial pressure (ICP) is con- ter DC [5].