Coding, Documentation, Reimbursement & Compliance Issues for Physician Practices & Ascs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anterior Reconstruction Techniques for Cervical Spine Deformity
Neurospine 2020;17(3):534-542. Neurospine https://doi.org/10.14245/ns.2040380.190 pISSN 2586-6583 eISSN 2586-6591 Review Article Anterior Reconstruction Techniques Corresponding Author for Cervical Spine Deformity Samuel K. Cho 1,2 1 1 1 https://orcid.org/0000-0001-7511-2486 Murray Echt , Christopher Mikhail , Steven J. Girdler , Samuel K. Cho 1Department of Orthopedics, Icahn School of Medicine at Mount Sinai, New York, NY, USA Department of Orthopaedics, Icahn 2 Department of Neurological Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, School of Medicine at Mount Sinai, 425 NY, USA West 59th Street, 5th Floor, New York, NY, USA E-mail: [email protected] Cervical spine deformity is an uncommon yet severely debilitating condition marked by its heterogeneity. Anterior reconstruction techniques represent a familiar approach with a range Received: June 24, 2020 of invasiveness and correction potential—including global or focal realignment in the sagit- Revised: August 5, 2020 tal and coronal planes. Meticulous preoperative planning is required to improve or prevent Accepted: August 17, 2020 neurologic deterioration and obtain satisfactory global spinal harmony. The ability to per- form anterior only reconstruction requires mobility of the opposite column to achieve cor- rection, unless a combined approach is planned. Anterior cervical discectomy and fusion has limited focal correction, but when applied over multiple levels there is a cumulative ef- fect with a correction of approximately 6° per level. Partial or complete corpectomy has the ability to correct sagittal deformity as well as decompress the spinal canal when there is an- terior compression behind the vertebral body. -

Spinal Interventional Pain Management and Lumbar Spine Surgery
Spinal Interventional Pain Management and Lumbar Spine Surgery Policy Number: Original Effective Date: MM.06.024 01/01/2014 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/15/2017 Section: Surgery; Medicine Place(s) of Service: Office; Outpatient; Inpatient I. Description The following spinal interventional pain management and lumbar spine surgery procedures require precertification through Magellan Hawaii, formally known as National Imaging Associates, Inc. (NIA): A. Spinal Epidural Injections B. Paravertebral Facet Joint Denervation (radiofrequency neurolysis) C. Paravertebral Facet Joint Injections or Blocks D. Sacroiliac joint injections E. Lumbar Spinal Fusion Surgery II. Administrative Guidelines A. The ordering physician can obtain precertification or consult with Magellan Hawaii by accessing their website at http://www.radmd.com/ or by calling 1 (866) 306-9729, from 6 a.m. to 6 p.m., weekdays, Hawaii Time. Refer to the e-library for instructions on navigating the radmd.com website (RadMD Get Started) and requesting precertification/checking the status of a request (RadMD QuickStart). B. For access to the latest clinical guidelines used for precertification, go to www.radmd.com and click on the link entitled View Clinical Guidelines. C. For interventional pain management procedures (epidural injections, facet joint denervation neurolysis, facet joint injections and sacroiliac joint injections), if more than one procedure is planned, a separate precertification number must be obtained for each procedure planned. D. For spinal surgeries (lumbar fusions, lumbar decompressions, and lumbar microdiscectomy), one precertification number should be obtained for the most invasive surgery to be performed. E. Precertification requirements for injection procedures apply only to office and outpatient services (POS 11, 22, or 24). -

Managing and Recognizing Complications After Treatment of Acromioclavicular Joint Repair Or Reconstruction
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/272096166 Managing and recognizing complications after treatment of acromioclavicular joint repair or reconstruction Article in Current Reviews in Musculoskeletal Medicine · February 2015 DOI: 10.1007/s12178-014-9255-6 · Source: PubMed CITATION READS 1 182 6 authors, including: Patrick A Smith Matthew J Smith University of Missouri University of Missouri 28 PUBLICATIONS 255 CITATIONS 16 PUBLICATIONS 115 CITATIONS SEE PROFILE SEE PROFILE Seth L Sherman David L Flood University of Missouri University of Missouri 69 PUBLICATIONS 1,378 CITATIONS 3 PUBLICATIONS 21 CITATIONS SEE PROFILE SEE PROFILE Some of the authors of this publication are also working on these related projects: Commentary & Perspective Total Hip Arthroplasty View project Drug Reaction with Eosinophilia and Systemic Symptoms Associated with a Vancomycin-Impregnated Spacer View project All content following this page was uploaded by Xinning Li on 15 February 2015. The user has requested enhancement of the downloaded file. Curr Rev Musculoskelet Med DOI 10.1007/s12178-014-9255-6 SHOULDER SURGERY: COMPLICATIONS (X LI, SECTION EDITOR) Managing and recognizing complications after treatment of acromioclavicular joint repair or reconstruction Richard Ma & Patrick A. Smith & Matthew J. Smith & Seth L. Sherman & David Flood & Xinning Li # Springer Science+Business Media New York 2015 Abstract Complications of the acromioclavicular joint inju- Introduction ries can occur as a result of the injury itself, conservative management, or surgical treatment. Fortunately, the majority Injuries to the acromioclavicular (AC) joint are common, par- of acromioclavicular surgeries utilizing modern techniques ticularly among the young and active population. -

Functional Outcome Oxford Shoulder Score After Modified Weaver Dunn Technique Reconstruction in Patients with Acromioclavicular Injuries
International Journal of PharmTech Research CODEN (USA): IJPRIF, ISSN: 0974-4304, ISSN(Online): 2455-9563 Vol.12, No.03, pp 71-74, 2019 Functional Outcome Oxford Shoulder Score after Modified Weaver Dunn Technique Reconstruction in Patients with Acromioclavicular Injuries Hendra1*, Nino Nasution2, Andriandi3, Asnan Lelo4 1Resident of Orthopaedic and Traumatology, Faculty of Medicine University of Sumatera Utara/ Haji Adam Malik Hospital-Medan, Indonesia 2Consultant of Orthopaedic and Traumatology, Faculty of Medicine University of Sumatera Utara/ Haji Adam Malik Hospital-Medan, Indonesia 3Consultant of Orthopaedic and Traumatology, Faculty of Medicine University of Sumatera Utara/ Haji Adam Malik Hospital-Medan, Indonesia 4Statistic Consultant of Orthopaedic and Traumatology, Faculty of Medicine University of Sumatera Utara/ Haji Adam Malik Hospital-Medan, Indonesia Abstract : Objective : The aim of this study was to compare the clinical outcome of Oxford Shoulder Score in patients with acromioclavicular injuries that were operated with Modified Weaver Dunn Technique Reconstruction compared with the healthy side. Material And Methods : A total of 8 patients with acromioclavicular injuries from 2011 until 2019 that were included into the study that were treated with Modified Weaver Dunn Technique. Age, gender, range of motion and OSS score that was followed for minimum 6 months after surgery (Oxford Shoulder Score [OSS]) were recorded. Results : Patients' gender characteristics totalled three females (3) and five males (5). There weren’t -

Distinguished Lecture
Past Present and Future of Joint Manipulation Stanley V. Paris PT., PhD, FAPTA N.Z.S.P., F.N.Z.S.P.(Hon Fellow & Life).,, N.Z.M.T.A.,(Hon Life)., I.F.O.M.P.T.,(Hon Life)., F.A.A.O.M.P.T., M.C.S.P., B.I.M. Abstract: Presented as the first Distinguished Lecturers Award, of the American Academy of Orthopaedic Manipulative Physical Therapists October 2011, the paper begins by addressing the richness of manipulative experience that caused the Founding Fellows to create the Academy. Speaking to his concerns that this richness seems to be forgotten by many practitioners he reviewed also the known effects of manipulation before then evaluating the evidence based literature criticizing much of it for being too basic and taking the profession back to where we were some fifty years ago before specific manipulative techniques were in vogue. Thus the current research is largely on non- specific regional techniques done for effect rather than for pathoanatomical and mechanical consideration. Many of the techniques being studied and promoted as manipulations ion the current literature do not justify to be called “manipulations” lacking as they do “skilled passive movements to a joint.” The paper argues for remembering that published literature is only one leg of the three legged stool of evidenced based practice, the other legs being patients wishes and culture, and the third being individual therapists expertise. Given the quality of much current physical therapy evidenced based literature Dr. Paris did not think that it was of sufficient scope and quality on which to base our practice. -

Effectiveness of the Muscle Energy Technique Versus Osteopathic
International Journal of Environmental Research and Public Health Article Effectiveness of the Muscle Energy Technique versus Osteopathic Manipulation in the Treatment of Sacroiliac Joint Dysfunction in Athletes Urko José García-Peñalver 1, María Victoria Palop-Montoro 1 and David Manzano-Sánchez 2,* 1 Facultad de Fisioterapia, Universidad Católica de San Antonio (UCAM), Av. de los Jerónimos, 135, 30107 Murcia, Spain; [email protected] (U.J.G.-P.); [email protected] (M.V.P.-M.) 2 Facultad de Ciencias del Deporte, Universidad de Murcia, Calle Argentina, 19, 30720 San Javier, Murcia, Spain * Correspondence: [email protected]; Tel.: +34-693-35-33-97 Received: 21 May 2020; Accepted: 15 June 2020; Published: 22 June 2020 Abstract: Background: The study of injuries stemming from sacroiliac dysfunction in athletes has been discussed in many papers. However, the treatment of this issue through thrust and muscle-energy techniques has hardly been researched. The objective of our research is to compare the effectiveness of thrust technique to that of energy muscle techniques in the resolution of sacroiliac joint blockage or dysfunction in middle-distance running athletes. Methods: A quasi-experimental design with three measures in time (pre-intervention, intervention 1, final intervention after one month from the first intervention) was made. The sample consisted of 60 adult athletes from an Athletic club, who were dealing with sacroiliac joint dysfunction. The sample was randomly divided into three groups of 20 participants (43 men and 17 women). One intervention group was treated with the thrust technique, another intervention group was treated with the muscle–energy technique, and the control group received treatment by means of a simulated technique. -

Synovial Fluidfluid 11
LWBK461-c11_p253-262.qxd 11/18/09 6:04 PM Page 253 Aptara Inc CHAPTER SynovialSynovial FluidFluid 11 Key Terms ANTINUCLEAR ANTIBODY ARTHROCENTESIS BULGE TEST CRYSTAL-INDUCED ARTHRITIS GROUND PEPPER HYALURONATE MUCIN OCHRONOTIC SHARDS RHEUMATOID ARTHRITIS (RA) RHEUMATOID FACTOR (RF) RICE BODIES ROPE’S TEST SEPTIC ARTHRITIS Learning Objectives SYNOVIAL SYSTEMIC LUPUS ERYTHEMATOSUS 1. Define synovial. VISCOSITY 2. Describe the formation and function of synovial fluid. 3. Explain the collection and handling of synovial fluid. 4. Describe the appearance of normal and abnormal synovial fluids. 5. Correlate the appearance of synovial fluid with possible cause. 6. Interpret laboratory tests on synovial fluid. 7. Suggest further testing for synovial fluid, based on preliminary results. 8. List the four classes or categories of joint disease. 9. Correlate synovial fluid analyses with their representative disease classification. 253 LWBK461-c11_p253-262.qxd 11/18/09 6:04 PM Page 254 Aptara Inc 254 Graff’s Textbook of Routine Urinalysis and Body Fluids oint fluid is called synovial fluid because of its resem- blance to egg white. It is a viscous, mucinous substance Jthat lubricates most joints. Analysis of synovial fluid is important in the diagnosis of joint disease. Aspiration of joint fluid is indicated for any patient with a joint effusion or inflamed joints. Aspiration of asymptomatic joints is beneficial for patients with gout and pseudogout as these fluids may still contain crystals.1 Evaluation of physical, chemical, and microscopic characteristics of synovial fluid comprise routine analysis. This chapter includes an overview of the composition and function of synovial fluid, and laboratory procedures and their interpretations. -
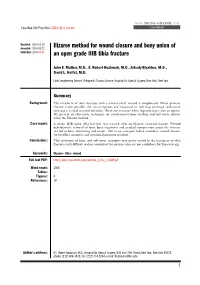
Ilizarov Method for Wound Closure and Bony Union of an Open Grade IIIB
WWW.CRCPR-ONLINE.COM Case Rep Clin Pract Rev, 2004; 5(1): xxx-xxx Case Report Received: 2003.01.10 Accepted: 2003.05.22 Ilizarov method for wound closure and bony union of Published: 2004.00.00 an open grade IIIB tibia fracture John E. Mullen, M.D., S. Robert Rozbruch, M.D., Arkady Blyakher, M.D., David L. Helfet, M.D. Limb Lengthening Service, Orthopedic Trauma Service, Hospital for Special Surgery, New York, New York Summary Background: The treatment of tibia fractures with a critical sized wound is complicated. When primary closure is not possible, the classic options are rotational or free flap coverage. Soft-tissue coverage is critical to avoid infection. There are instances when flap coverage is not an option. We present an alternative technique for simultaneous bone healing and soft tissue closure using the Ilizarov method. Case report: A grade IIIB open tibia fracture was treated with an Ilizarov external fixator. Wound debridement, removal of loose bone fragments and gradual compression across the fracture site led to bony shortening and union. Soft tissue transport led to secondary wound closure. An excellent anatomic and functional outcome resulted. Conclusions: This technique of bone and soft-tissue transport may prove useful in the treatment of tibia fractures with difficult to close wounds or for patients who are not candidates for flap coverage. Key words: Ilizarov•tibia•wound Full-text PDF: http://www.crcpr-online.com/pub/vol_5/no_1/3389.pdf Word count: 1506 Tables: - Figures: 8 References: 19 Author’s address: GS. Robert Rozbruch, M.D., Hospital for Special Surgery, 535 East 70th Street, New York, New York 10021, phone: (212) 606-1415, fax: (212) 774-2744, e-mail: [email protected] 1 Case Report BACKGROUND Open fractures of the tibial shaft are both common and may be fraught with complications. -
Validation of a Clinical Prediction Rule for the Differentiation Between Septic Arthritis and Transient Synovitis of the Hip in Children by MININDER S
COPYRIGHT © 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED Validation of a Clinical Prediction Rule for the Differentiation Between Septic Arthritis and Transient Synovitis of the Hip in Children BY MININDER S. KOCHER, MD, MPH, RAHUL MANDIGA, BS, DAVID ZURAKOWSKI, PHD, CAROL BARNEWOLT, MD, AND JAMES R. KASSER, MD Investigation performed at the Departments of Orthopaedic Surgery, Biostatistics, and Radiology, Children’s Hospital, Boston, Massachusetts Background: The differentiation between septic arthritis and transient synovitis of the hip in children can be difficult. The purpose of the present study was to validate a previously published clinical prediction rule for this differentiation in a new patient population. Methods: We prospectively studied children who presented to a major children’s hospital between 1997 and 2002 with an acutely irritable hip. As in the previous study, diagnoses of septic arthritis (fifty-one patients) and transient synovitis (103 patients) were operationally defined on the basis of the white blood-cell count in the joint fluid, the re- sults of cultures of joint fluid and blood, and the clinical course. Univariate analysis and multiple logistic regression were used to compare the two groups. The predicted probability of septic arthritis of the hip from the prediction rule was compared with actual distributions in the current patient population. The area under the receiver operating char- acteristic curve was determined. Results: The same four independent predictors of septic arthritis of the hip (a history of fever, non-weight-bearing, an erythrocyte sedimentation rate of 40 mm/hr, and a serum white blood-cell count of >12,000 cells/mm3 (>12.0 × 109/L)) were identified in the current patient population. -

Lumbar Laminectomy Or Laminotomy
Patient Instructions: Lumbar Laminectomy or Laminotomy Surgical Technique A lumbar laminectomy or laminotomy is a surgical approach performed from the back of the lumbar spine. It is usually done through an incision in the middle of the back. Using minimally invasive techniques a small window of bone is drilled in the lamina to allow the surgeon to unpinch the underlying nerves (laminotomy), or in more severe cases the bone is removed completely on both sides to allow nerves on both sides of the spinal canal to be decompressed (laminectomy). It is done using an operating microscope and microsurgical technique. It is used to treat spinal stenosis or lateral recess stenosis and alleviate the pain and/or numbness that occurs in a patients lower back or legs. It can many times be performed on an outpatient basis without the need for an overnight stay in a hospital. Before Surgery • Seven days prior to surgery, please do not take any anti-inflammatory NSAID medications (Celebrex, Ibuprofen, Aleve, Naprosyn, Advil, etc.) as this could prolong your bleeding time during surgery. • Do not eat or drink anything after midnight the day before surgery. This means nothing to drink the morning of surgery except you may take your normal medication with a sip of water if needed. This includes your blood pressure medicine, which in general should be taken. Consult your surgeon or primary care doctor regarding insulin if you take it. • Please do not be late to check in on the day of surgery or it may be cancelled. • Please bring your preoperative folder with you to the surgery and have it when you check in. -

3Rd Quarter 2001 Bulletin
In This Issue... Promoting Colorectal Cancer Screening Important Information and Documentaion on Promoting the Prevention of Colorectal Cancer ....................................................................................................... 9 Intestinal and Multi-Visceral Transplantation Coverage Guidelines and Requirements for Approval of Transplantation Facilities12 Expanded Coverage of Positron Emission Tomography Scans New HCPCS Codes and Coverage Guidelines Effective July 1, 2001 ..................... 14 Skilled Nursing Facility Consolidated Billing Clarification on HCPCS Coding Update and Part B Fee Schedule Services .......... 22 Final Medical Review Policies 29540, 33282, 67221, 70450, 76090, 76092, 82947, 86353, 93922, C1300, C1305, J0207, and J9293 ......................................................................................... 31 Outpatient Prospective Payment System Bulletin Devices Eligible for Transitional Pass-Through Payments, New Categories and Crosswalk C-codes to Be Used in Coding Devices Eligible for Transitional Pass-Through Payments ............................................................................................ 68 Features From the Medical Director 3 he Medicare A Bulletin Administrative 4 Tshould be shared with all General Information 5 health care practitioners and managerial members of the General Coverage 12 provider/supplier staff. Hospital Services 17 Publications issued after End Stage Renal Disease 19 October 1, 1997, are available at no-cost from our provider Skilled Nursing Facility -
Exploring Vigilance Notification for Organs
NOTIFY - E xploring V igilanc E n otification for o rgans , t issu E s and c E lls NOTIFY Exploring VigilancE notification for organs, tissuEs and cElls A Global Consultation e 10,00 Organised by CNT with the co-sponsorship of WHO and the participation of the EU-funded SOHO V&S Project February 7-9, 2011 NOTIFY Exploring VigilancE notification for organs, tissuEs and cElls A Global Consultation Organised by CNT with the co-sponsorship of WHO and the participation of the EU-funded SOHO V&S Project February 7-9, 2011 Cover Bologna, piazza del Nettuno (photo © giulianax – Fotolia.com) © Testi Centro Nazionale Trapianti © 2011 EDITRICE COMPOSITORI Via Stalingrado 97/2 - 40128 Bologna Tel. 051/3540111 - Fax 051/327877 [email protected] www.editricecompositori.it ISBN 978-88-7794-758-1 Index Part A Bologna Consultation Report ............................................................................................................................................7 Part B Working Group Didactic Papers ......................................................................................................................................57 (i) The Transmission of Infections ..........................................................................................................................59 (ii) The Transmission of Malignancies ....................................................................................................................79 (iii) Adverse Outcomes Associated with Characteristics, Handling and Clinical Errors