Physiotherapy Self-Referral
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
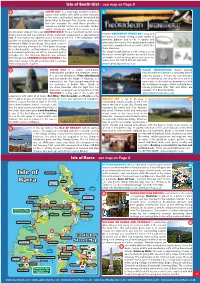
-

Iona, Harris and Govan in Scotland Alastair Mcintosh
Offprint of chapter by Alastair Mclntosh - The 'Sacredness' of Natural Sites and Their Recovery: lona, Harris and Govan in Scotland, 2012 (full reference on final page). The full text of this book can be downloaded free from: IUCN www.iucn.org/dbtw-wpd/edocs/2012-006.pdf METSAHALLITUS ^WCPA ~~ WORLD COMMISSION ON PROTECTED AREAS The ‘sacredness’ of natural sites and their recovery: Iona, Harris and Govan in Scotland Alastair McIntosh Science and the sacred: with which science can, and even a necessary dichotomy? should, meaningfully engage? It is a pleasing irony that sacred natural In addressing these questions science sites (SNSs), once the preserve of reli- most hold fast to its own sacred value – gion, are now drawing increasing rec- integrity in the pursuit of truth. One ap- ognition from biological scientists (Ver- proach is to say that science and the schuuren et al., 2010). At a basic level sacred cannot connect because the for- this is utilitarian. SNSs frequently com- mer is based on reason while the latter prise rare remaining ecological ‘is- is irrational. But this argument invariably lands’ of biodiversity. But the very exist- overlooks the question of premises. ence of SNSs is also a challenge to sci- Those who level it make the presump- ence. It poses at least two questions. tion that the basis of reality is materialis- Does the reputed ‘sacredness’ of these tic alone. The religious, by contrast, ar- sites have any significance for science gue that the basis of reality, including beyond the mere utility by which they material reality, is fundamentally spiritu- happen to conserve ecosystems? And al. -

Towards a Sonic Methodology Cathy
Island Studies Journal , Vol. 11, No. 2, 2016, pp. 343-358 Mapping the Outer Hebrides in sound: towards a sonic methodology Cathy Lane University of the Arts London, United Kingdom [email protected] ABSTRACT: Scottish Gaelic is still widely spoken in the Outer Hebrides, remote islands off the West Coast of Scotland, and the islands have a rich and distinctive cultural identity, as well as a complex history of settlement and migrations. Almost every geographical feature on the islands has a name which reflects this history and culture. This paper discusses research which uses sound and listening to investigate the relationship of the islands’ inhabitants, young and old, to placenames and the resonant histories which are enshrined in them and reveals them, in their spoken form, as dynamic mnemonics for complex webs of memories. I speculate on why this ‘place-speech’ might have arisen from specific aspects of Hebridean history and culture and how sound can offer a new way of understanding the relationship between people and island toponymies. Keywords: Gaelic, island, landscape, memory, Outer Hebrides, place-speech, sound © 2016 – Institute of Island Studies, University of Prince Edward Island, Canada Introduction I am a composer, sound artist and academic. In my creative practice I compose concert works and gallery installations. My current practice focuses around sound-based investigations of a place or theme and uses a mixture of field recording, interview, spoken text and existing oral history archive recordings as material. I am interested in the semantic and the abstract sonic qualities of all this material and I use it to construct “docu-music” (Lane, 2006). -

Sport & Activity Directory Uist 2019
Uist’s Sport & Activity Directory *DRAFT COPY* 2 Foreword 2 Welcome to the Sport & Activity Directory for Uist! This booklet was produced by NHS Western Isles and supported by the sports division of Comhairle nan Eilean Siar and wider organisations. The purpose of creating this directory is to enable you to find sports and activities and other useful organisations in Uist which promote sport and leisure. We intend to continue to update the directory, so please let us know of any additions, mistakes or changes. To our knowledge the details listed are correct at the time of printing. The most up to date version will be found online at: www.promotionswi.scot.nhs.uk To be added to the directory or to update any details contact: : Alison MacDonald Senior Health Promotion Officer NHS Western Isles 42 Winfield Way, Balivanich Isle of Benbecula HS7 5LH Tel No: 01870 602588 Email: [email protected] . 2 2 CONTENTS 3 Tai Chi 7 Page Uist Riding Club 7 Foreword 2 Uist Volleyball Club 8 Western Isles Sports Organisations Walk Football (40+) 8 Uist & Barra Sports Council 4 W.I. Company 1 Highland Cadets 8 Uist & Barra Sports Hub 4 Yoga for Life 8 Zumba Uibhist 8 Western Isles Island Games Association 4 Other Contacts Uist & Barra Sports Council Members Ceolas Button and Bow Club 8 Askernish Golf Course 5 Cluich @ CKC 8 Benbecula Clay Pigeon Club 5 Coisir Ghaidhlig Uibhist 8 Benbecula Golf Club 5 Sgioba Drama Uibhist 8 Benbecula Runs 5 Traditional Spinning 8 Berneray Coastal Rowing 5 Taigh Chearsabhagh Art Classes 8 Berneray Community Association -
Isle of Barra - See Map on Page 8
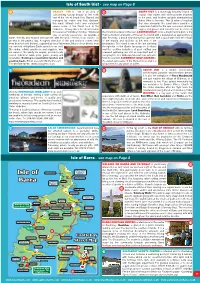
Isle of South Uist - see map on Page 8 65 SOUTH UIST is a stunningly beautiful island of 68 crystal clear waters with white powder beaches to the west, and heather uplands dominated by Beinn Mhor to the east. The 20 miles of machair that runs alongside the sand dunes provides a marvellous habitat for the rare corncrake. Golden eagles, red grouse and red deer can be seen on the mountain slopes to the east. LOCHBOISDALE, once a major herring port, is the main settlement and ferry terminal on the island with a population of approximately Visit the HEBRIDEAN JEWELLERY shop and 300. A new marina has opened, and is located at the end of the breakwater with workshop at Iochdar, selling a wide variety of facilities for visiting yachts. Also newly opened Visitor jewellery, giftware and books of quality and Information Offi ce in the village. The island is one of good value for money. This quality hand crafted the last surviving strongholds of the Gaelic language jewellery is manufactured on South Uist in the in Scotland and the crofting industries of peat cutting Outer Hebrides. and seaweed gathering are still an important part of The shop in South Uist has a coffee shop close by everyday life. The Kildonan Museum has artefacts the beach, where light snacks are served. If you from this period. ASKERNISH GOLF COURSE is the are unable to visit our shop, please visit us on our oldest golf course in the Western Isles and is a unique online store. Tel: 01870 610288. HS8 5QX. -

ON ISLAY PLACE-NAMES. by CAPT. F. W. L. THOMAS, R.N., F.S.A. Soot
I. ON ISLAY PLACE-NAMES CAPTy B . W.F . L. THOMAS, R.N., F.S.A. Soot. Whe examinatioe nth e Lewith f no s Place-Names—wit e vieth hf wo ascertaining to what extent the Scandinavian influence had been im- pressed there—was finished, it seemed very desirable that the name- system of the Southern Hebrides, particularly Tslay, should be inquired intoj for comparison with that of Lewis; but having no local acquaint- ance with the island d onlan ,y ver e d mapsb y ba e attemp o t th , d ha t postponed. But having lately the offer of assistance from Mr. Hector Maclean of Ballygrant, Islay, who, besides having a critical knowledge of Gaelic, is thoroughly acquainted with the topography of Islay, it was considered safe to proceed, but without his co-operation this account of Islay Place-Names coul t havdno e been written. This paper must be considered complementary to that on Lewis Place- Names, to which the reader is referred for many remarks bearing on the present subject t whichbu , avoio t , d repetition omittee ar , d here,. formee th n I r pape methoe th r s detailedi whicy db namee hth s them- selves were determined and their analysis performed,—and the same system has been followed in this. To prevent any unconscious selection, and as affordin faia g r exampl e name-systeth f eo mIslayn i lise farmf o th ,t n i s the Valuation Rol f Argyllshiro l s takea basis wa es a n . These names VOL. -

34 MYRIAPODS on the OUTER HEBRIDES Gordon B Corbet Little
BULLETIN OF THE BRITISH MYRIAPOD AND ISOPOD GROUP Volume 20 2004 MYRIAPODS ON THE OUTER HEBRIDES Gordon B Corbet Little Dumbarnie, Upper Largo, Leven, Fife, KY8 6JG. INTRODUCTION Published records of myriapods from the Outer Hebrides are scanty and are summarised in three sources. Waterston (1981) recorded 15 species, with a list of islands from which each had been recorded. This incorporated records from Barra in 1935 reported by Waterston (1936). The provisional atlases (British Myriapod Group, 1988 for millipedes, Barber & Keay, 1988 for centipedes) recorded seven species, adding two to the total, but did not claim to be comprehensive with regard to earlier published records. In addition there are unpublished records of millipedes rising from a survey of invertebrates conducted in 1976 by the Institute of Terrestrial Ecology (ITE, 1979). This included pitfall-trapping at 18 sites on Lewis/Harris, North Uist, Benbecula and South Uist, but produced only Cylindroiulus latestriatus (at every site), plus a single Polydesmus inconstans on North Uist. I visited the Outer Hebrides from 3rd to 13th June 2003 and recorded myriapods on the following islands: Lewis/Harris, Great Bernera (bridged), Scalpay (bridged), South Uist, Eriskay (bridged), Barra and Vatersay (bridged). Recording was solely by hand searching in leaf-litter and under stones, wood and refuse. The general impression was that myriapods were scarce, with a large proportion of turned stones revealing nothing. In contrast earwigs, Forficula auricularia were unusually abundant. MILLIPEDES Waterston (1981) recorded six species, including one, Cylindroiulus britannicus, from St Kilda only. The provisional atlas recorded four species post-1970 adding Ophyiulus pilosus. -
Isle of Barra - See Map on Page 8
Isle of South Uist - see map on Page 8 63 ORASAY INN is set in an area of 66 SOUTH UIST is a stunningly beautiful island of outstanding natural beauty at the north crystal clear waters with white powder beaches end of the Isle of South Uist. Owned and to the west, and heather uplands dominated by managed by Isobel and Alan Graham, Beinn Mhor to the east. The 20 miles of machair this small, intimate hotel and restaurant that runs alongside the sand dunes provides a serves some of the fi nest food in the marvellous habitat for the rare corncrake. Golden Hebrides. Orasay Inn is the ideal location eagles, red grouse and red deer can be seen on for a special Hebridean holiday. Whatever the mountain slopes to the east. LOCHBOISDALE, once a major herring port, is the type of activity you prefer, we provide a main settlement and ferry terminal on the island with a population of approximately warm, friendly and relaxed atmosphere, with the best of fresh, local cuisine, as 300. Recently, a brand new marina has opened, with a good walk from the village an end to the perfect day. A superb selection of fi sh and seafood comes fresh to the marina and facilities at the end of the from boat to hotel kitchen, supplied by local fi shermen. Much of our beef is from breakwater. The island is one of the last surviving our own fold of Highland Cattle, raised on our croft. strongholds of the Gaelic language in Scotland Discerning, reliable producers and suppliers, who and the crofting industries of peat cutting and are aware of the quality we require, provide locally seaweed gathering are still an important part of reared Hebridean lamb, pork, game, poultry and everyday life. -

The Western Isles of Lewis, Harris, Uists, Benbecula and Barra
The Western Isles of Lewis, Harris, Uists, Benbecula and Barra 1 SEATREK is based in Uig on 5 UIG SANDS RESTAURANT is a newly Let the adventure begin! Lewis, one of the most beautiful opened licensed restaurant with spectacular locations in Britain. We offer views across the beach. Open for lunches unforgettable boat trips around and evening meals. Booking essential. the Hebrides. All welcome, relaxed atmosphere and family Try any of our trips for a great friendly. Timsgarry, Isle of Lewis HS2 9ET. family experience with the Tel: 01851 672334. opportunity of seeing seals, Email: [email protected] basking sharks, dolphins and www.uigsands.co.uk many species of birds. DOUNE BRAES HOTEL: A warm welcome awaits you. We especially 6 Leaving from Miavaig Seatrek RIB Short Trips cater for ‘The Hebridean Way’ for cyclists, walkers and motorcyclists. Harbour, Uig, Isle of Lewis. We have safe overnight storage for bicycles. We offer comfortable Tel: 01851 672469. Sea Eagles & Lagoon Trip .............................. 2 hours accommodation, light meals served through the day and our full www.seatrek.co.uk Island Excursion ................................................. 3 hours evening menu in the evening. Locally sourced produce including Email: [email protected] Customised Trips ............................................... 4 hours our own beef raised on our croft, shellfi sh and local lamb. There’s a Fishing Trip ........................................................... 2 hours Gallan Head Trip ................................................. 2 hours good selection of Malt Whiskies in the Lounge Bar or coffees to go Sea Stacks Trip ................................................... 2 hours whilst you explore the West Side of the Island. Tel: 01851 643252. Email: [email protected] www.doune-braes.co.uk 2 SEA LEWIS BOAT TRIPS: Explore the 7 BLUE PIG CREATIVE SPACE: coastline North and South of Stornoway Carloway’s unique working studio and in our 8.5m Rib. -

Outer Hebrides Island Hopscotch
OUTER HEBRIDES ISLAND HOPSCOTCH SELF DRIVE WALKING HOLIDAY EXPLORE THE OUTER HEBRIDES - SELF DRIVE AND WALKING HOLIDAY A relaxed self guided walking and driving holiday through spectacular scenery of Barra, the Uists, SUMMARY Harris and Lewis. Enjoy the mixture of the varied landscapes on the Western Isles of Scotland. On this self guided walking and driving holiday explore the 130 mile chain of Islands that stretch along the North Western Coast of Scotland and enjoy the almost tangible qualities of remoteness and beauty. Follow the route by car and ferry with daily walks through a mosaic of differing landscapes. The trip comprises 6 full days and 7 nights travelling from rugged compact Barra in the far South through to the exposed ’Butt of Lewis’ jutting out into the North Atlantic. There is no set itinerary, you may choose where and when you walk, but we provide you with suggested options for each day. This trip is suitable for those with use of a car as there is little public transport and many of the walks are remote. You will pass through changing scenery as you move through the islands and each day allows you to enjoy the indigenous flora and fauna perfectly adapted to this wild and beautiful region of Scotland. Glorious white sand beaches border the dramatic hills and moorlands providing the ultimate in solitude and tranquillity for the discerning walker. This natural splendour is in perfect harmony with the ancient historical wonders that adorn the islands, affording opportunities to explore the awe inspiring heritage that abounds The trip includes your ferry crossings from Oban on the Scottish mainland to the Isle of Barra, your ferries Tour: Outer Hebrides Hopscotch as per itinerary through the Islands to Lewis and also back to Ullapool on the mainland. -

HIAL Annual Report and Accounts
Annual Report and Accounts to 31 March 2020 About us Sumburgh Highlands and Islands Airports Limited (HIAL) is a private limited company wholly owned by the Kirkwall Scottish Ministers and is Wick John O’Groats responsible for the management Stornoway and operation of 11 airports. Benbecula Our airports are located at: Barra, Benbecula, Inverness Campbeltown, Dundee, Inverness, Islay, Kirkwall, Stornoway, Sumburgh, Tiree and Wick John Barra O'Groats. Working with our partners and stakeholders, Tiree Dundee we are committed to supporting the essential socio-economic role of aviation in Scotland by maintaining and developing our airports and the vital lifeline services and connections they provide Islay for some of our country’s more remote communities. Campbeltown Contents 1 Chair’s statement 23 Group statement of comprehensive income 2 Managing director’s statement 23 Company statement of comprehensive income 5 Strategic report 24 Group statement of changes in equity 13 Directors’ report 24 Company statement of changes in equity 14 Governance statement 25 Group balance sheet 18 Statement of directors’ responsibilities 26 Company balance sheet 19 Independent auditor’s report 27 Group cash flow statement 22 Group income statement 28 Notes to the financial statements Chair’s Statement It is during unprecedented times that I introduce We are committed to innovation and providing HIAL’s Report and Accounts for 2019/20. As I write sustainable aviation services for the future and will my introduction we are still operating within the continue with our drive for environmental excellence necessary restrictions introduced to combat and and progress key innovative programmes such as our contain the Coronavirus pandemic. -

W Alking the Hebridean W Ay
In brief Total Distance: 156 miles (252km) the Hebridean Way Walking 6 Distance by Islands: 1 Vatersay and Barra: 15 miles (24km) Category: Moderate Sound of Barra Ferry Journey Time: 40 mins 2 Eriskay and South Uist: 35 miles (57km) 5 Category: Easy / Moderate 3 Benbecula and Grimsay: 16 miles (26km) Category: Moderate 4 The Hebridean Way is a 4 North Uist and Berneray: 22 miles (36km) long-distance walking route Category: Moderate 3 through the Outer Hebrides. It links some of the best places in Scotland to explore Sound of Harris Ferry Journey Time: 1 hour and admire the spectacular 2 natural environment. You can 5 Harris: 38 miles (61km) also cycle the Hebridean Way following the National Cycling Category: Difficult Route (NCN 780). Find out more on the website below. 1 6 Lewis: 30 miles (48km) 156 Miles Category: Moderate / Difficult 10 Islands #HebWay 6 Causeways www.hebrideanway.co.uk 2 Ferries www.visitouterhebrides.co.uk/apps The Route Suggested schedules Outdoor Safety To enable you to easily plan your walk, we’ve split the path into 12 Staying safe whilst walking is mostly a matter of common sense: The Hebridean Way offers one of the finest sections as listed A - L below. Each of these sections cover a typical • Check the weather forecast before you set out. walking experiences in Europe. Nowhere else day’s walk. (Note: Distances are approximate and do not include additional distances to the accommodation). • Take appropriate clothing – this walk covers some rough, offers such a rich combination of attractions: wet ground, so wear your boots. -

Outer Hebrides Outer Hebrides
Scottish Natural Heritage Explore for a day Outer Hebrides Outer Hebrides Itinerary 1 Itinerary 2 Itinerary 3 Itinerary 4 Itinerary 5 Words will not do justice to the spectacular beauty, stunning wildlife and fascinating history of the Outer Hebrides. Explore the land of the machair – the low-lying fertile plain that fringes the west of these islands and is maintained by traditional crofting Symbol Key practices – providing some of the world’s finest flower-rich meadows, busy with wading birds. Parking Information Centre Cliffs covered in noisy seabirds, majestic eagles soaring high overhead and otters along the seaweed-fringed shore make your visit here special and memorable. Add to this mix, the vast peatlands of Lewis, the Paths Disabled Access presence of the sea in all its moods, the rocky coasts, stunning beaches of white sand and scattered crofting settlements strung out through Toilets Wildlife watching these islands and you have an unforgettable place. Find out more about the mysterious monuments of first settlers and the Refreshments Picnic Area traces of early Christianity in these isles. Encounter more modern stories of powerful clans, emigration, land struggles, the emergence of whaling, fishing and tweed industries and ships full of whisky running aground! Admission free unless otherwise stated. This leaflet gives you a flavour of the journey through the whole island chain from Barra to the Butt of Lewis and suggest places to visit along the way that will help you discover a little of what these islands at the very This leaflet was prepared with the assistance edge of Europe have to offer.