Glomerular Endothelial Cells Impairs Activation of Protein C in Human
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WO 2016/147053 Al 22 September 2016 (22.09.2016) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2016/147053 Al 22 September 2016 (22.09.2016) P O P C T (51) International Patent Classification: (71) Applicant: RESVERLOGIX CORP. [CA/CA]; 300, A61K 31/551 (2006.01) A61P 37/02 (2006.01) 4820 Richard Road Sw, Calgary, AB, T3E 6L1 (CA). A61K 31/517 (2006.01) C07D 239/91 (2006.01) (72) Inventors: WASIAK, Sylwia; 431 Whispering Water (21) International Application Number: Trail, Calgary, AB, T3Z 3V1 (CA). KULIKOWSKI, PCT/IB20 16/000443 Ewelina, B.; 31100 Swift Creek Terrace, Calgary, AB, T3Z 0B7 (CA). HALLIDAY, Christopher, R.A.; 403 (22) International Filing Date: 138-18th Avenue SE, Calgary, AB, T2G 5P9 (CA). GIL- 10 March 2016 (10.03.2016) HAM, Dean; 249 Scenic View Close NW, Calgary, AB, (25) Filing Language: English T3L 1Y5 (CA). (26) Publication Language: English (81) Designated States (unless otherwise indicated, for every kind of national protection available): AE, AG, AL, AM, (30) Priority Data: AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, 62/132,572 13 March 2015 (13.03.2015) US BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, 62/264,768 8 December 2015 (08. 12.2015) US DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, [Continued on nextpage] (54) Title: COMPOSITIONS AND THERAPEUTIC METHODS FOR THE TREATMENT OF COMPLEMENT-ASSOCIATED DISEASES (57) Abstract: The invention comprises methods of modulating the complement cascade in a mammal and for treating and/or preventing diseases and disorders as sociated with the complement pathway by administering a compound of Formula I or Formula II, such as, for example, 2-(4-(2-hydroxyethoxy)-3,5-dimethylphenyl)- 5,7-dimethoxyquinazolin-4(3H)-one or a pharmaceutically acceptable salt thereof. -

Clinical Study High Complement Factor I Activity in the Plasma of Children with Autism Spectrum Disorders
Hindawi Publishing Corporation Autism Research and Treatment Volume 2012, Article ID 868576, 6 pages doi:10.1155/2012/868576 Clinical Study High Complement Factor I Activity in the Plasma of Children with Autism Spectrum Disorders Naghi Momeni,1 Lars Brudin,2 Fatemeh Behnia,3 Berit Nordstrom,¨ 4 Ali Yosefi-Oudarji,5 Bengt Sivberg,4 Mohammad T. Joghataei,5 and Bengt L. Persson1 1 School of Natural Sciences, Linnaeus University, 39182 Kalmar, Sweden 2 Department of Clinical Physiology, Kalmar County Hospital, 39185 Kalmar, Sweden 3 Department of Occupational Therapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran 4 Department of Health Sciences, Autism Research, Faculty of Medicine, Lund University, Box 157, 22100 Lund, Sweden 5 Cellular and Molecular Research Centre, Tehran University of Medical Sciences (TUMS), Tehran, Iran Correspondence should be addressed to Bengt Sivberg, [email protected] Received 17 June 2011; Revised 22 August 2011; Accepted 22 August 2011 Academic Editor: Judy Van de Water Copyright © 2012 Naghi Momeni et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Autism spectrum disorders (ASDs) are neurodevelopmental and behavioural syndromes affecting social orientation, behaviour, and communication that can be classified as developmental disorders. ASD is also associated with immune system abnormality. Im- mune system abnormalities may be caused partly by complement system factor I deficiency. Complement factor I is a serine pro- tease present in human plasma that is involved in the degradation of complement protein C3b, which is a major opsonin of the complement system. -

Advances in Hematology
ADVANCES IN HEMATOLOGY Current Developments in the Management of Hematologic Disorders Hematology Section Editor: Craig M. Kessler, MD Atypical Hemolytic Uremic Syndrome: The Role of Complement Pathway Gene Mutation Analysis Ilene C. Weitz, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC Los Angeles, California H&O What causes atypical hemolytic uremic H&O Which mutations in complement alternative syndrome (aHUS)? pathway genes are linked to aHUS? IW We think that most people with aHUS have problems IW Multiple genetic mutations have been linked to with regulation of complement. As a result of excess com- aHUS, especially those involved in the complement plement, endothelial and organ damage occur. We know alternative pathway. These include mutations in comple- that mutations in the genes of complement regulatory pro- ment factor H, complement factor I, membrane cofactor teins are associated with aHUS. In addition, factors other protein, complement factor B, and C3 nephritic factor. than underlying mutations may play a role in increasing Mutations may cause the protein to be normal but low in activation and the expression of the clinical syndrome. quantity, or normal in quantity but abnormal in function; the degree of the abnormality may depend on whether the H&O How is the complement system activated patient is heterozygous or homozygous. and regulated? In addition, other factors such as thrombomodulin have been described that work through other enzymes. IW The complement system is a part of the innate Thrombomodulin is involved in complement regulation immune system that is necessary for fighting infections by activating thrombin activatable fibrinolytic inhibitor and aberrant immunologic stimuli. -

367.Full.Pdf
Human Complement Factor I Does Not Require Cofactors for Cleavage of Synthetic Substrates This information is current as Stefanos A. Tsiftsoglou and Robert B. Sim of October 2, 2021. J Immunol 2004; 173:367-375; ; doi: 10.4049/jimmunol.173.1.367 http://www.jimmunol.org/content/173/1/367 Downloaded from References This article cites 41 articles, 17 of which you can access for free at: http://www.jimmunol.org/content/173/1/367.full#ref-list-1 Why The JI? Submit online. http://www.jimmunol.org/ • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average by guest on October 2, 2021 Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2004 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Human Complement Factor I Does Not Require Cofactors for Cleavage of Synthetic Substrates1 Stefanos A. Tsiftsoglou2 and Robert B. Sim Complement factor I (fI) plays a major role in the regulation of the complement system. It circulates in an active form and has very restricted specificity, cleaving only C3b or C4b in the presence of a cofactor such as factor H (fH), complement receptor type 1, membrane cofactor protein, or C4-binding protein. -

Crystal Structure of Prethrombin-1
Crystal structure of prethrombin-1 Zhiwei Chen, Leslie A. Pelc, and Enrico Di Cera1 Department of Biochemistry and Molecular Biology, Saint Louis University School of Medicine, Saint Louis, MO 63104 Edited by Robert M. Stroud, University of California, San Francisco, CA, and approved September 24, 2010 (received for review July 14, 2010) Prothrombin is the zymogen precursor of the clotting enzyme thrombin, which is generated by two sequential cleavages at R271 and R320 by the prothrombinase complex. The structure of prothrombin is currently unknown. Prethrombin-1 differs from pro- thrombin for the absence of 155 residues in the N-terminal domain and is composed of a single polypeptide chain containing fragment 2 (residues 156–271), A chain (residues 272–320), and B chain (re- sidues 321–579). The X-ray crystal structure of prethrombin-1 solved at 2.2-Å resolution shows an overall conformation signifi- cantly different (rmsd ¼ 3.6 Å) from that of its active form meizo- thrombin desF1 carrying a cleavage at R320. Fragment 2 is rotated around the y axis by 29° and makes only few contacts with the B chain. In the B chain, the oxyanion hole is disrupted due to absence of the I16-D194 ion pair and the Naþ binding site and adjacent primary specificity pocket are highly perturbed. A remarkable feature of the structure is that the autolysis loop assumes a helical conformation enabling W148 and W215, located 17 Å apart in mei- zothrombin desF1, to come within 3.3 Å of each other and comple- tely occlude access to the active site. -

Factor B, the Complement Alternative Pathway Serine Proteinase, Is a Major Constitutive Protein Synthesized and Secreted by Resident and Elicited Mouse Macrophages
FACTOR B, THE COMPLEMENT ALTERNATIVE PATHWAY SERINE PROTEINASE, IS A MAJOR CONSTITUTIVE PROTEIN SYNTHESIZED AND SECRETED BY RESIDENT AND ELICITED MOUSE MACROPHAGES BY JOHN S. SUNDSMO, JENNIE R. CHIN,* RUTH A. PAPIN, DARYL S. FAIR, AND ZENA WERB* From the Department of Molecular Immunology, Scripps Clinic and Research Foundation, La Jolla, California 92037; and the *Laboratory of Radiobiology and Environmental Health, and Department of Anatomy, University of California, San Francisco, California 94143 Mononuclear phagocytes have been increasingly recognized as a source of many of the complement proteins (1, 2). Activities constituting the intact com- plement alternative pathway in serum (factor B, factor D, C3, and properdin) (3-8), as well as the regulatory proteins, factors H and I (5, 8), are produced by mouse peritoneal macrophages and human peripheral blood monocytes. Factors C2 and C4 are also synthesized by mononuclear phagocytes (1, 2, 5, 9-11). Factor B, a glycoprotein of Mr ~0.3,000 that plays a central role in the alternative pathway of complement activation (12, 13), is closely associated with the immune response as a class III gene product of the major histocompatibility complex in mice (14, 15), guinea pigs (16), and humans (17). Activated factor B (Bb, Mr ~60,000) serves as a migration inhibiting factor (18), inducing macro- phage and monocyte spreading (19, 20) and possibly stimulating cytotoxic (21, 22) and bacteriocidai activities (23, 24) of monocytes in vitro. The hemolytic activity of factor B produced by resident mouse peritoneal macrophages (3, 6) increases linearly during 72-96 h in culture, and its synthesis is regulated by lipopolysaccharide (LPS) 1 (24). -

Factor B Catalog Number
Name: Factor B Catalog Number: A135 Sizes Available: 250 µg/vial Concentration: 1.0 mg/mL (see Certificate of Analysis for actual concentration) Form: Frozen liquid Activity: >90% versus normal human serum standard. Purity: >95% by SDS-PAGE Buffer: 10 mM Sodium phosphate, 145 mM NaCl, pH 7.2 Molecular weight: 93,000 Da (single chain) Extinction Coeff.: A280 nm = 1.27 at 1.0 mg/mL Preservative: None, 0.22 µm filtered Storage: -70oC or below. Avoid repeated freeze/thaw. Source: Normal human serum (shown by certified tests to be negative for HBsAg and for antibodies to HCV, HIV-1 and HIV-II). Precautions: Use normal precautions for handling human blood products. Origin: Manufactured in the USA. General Description Complement factor B (fB) is purified from normal human serum. Complement factor B is a glycosylated protein composed of a single 93,000 Da polypeptide chain. It is an essential component of the alternative pathway of complement activation and is found in plasma at approximately 200 µg/mL. In the presence of Mg++ factor B binds to C3b and the C3b,B complex can be activated by factor D, a serine protease that circulates as an active trypsin-like serine protease. Cleavage of factor B by factor D causes the release of the Ba fragment (33,000 Da) and leaves the 60,000 Bb fragment bound to C3b. This Bb subunit is a serine protease. C3b,Bb is called a C3 and a C5 convertase because it converts both of these proteins to their active forms by cleaving off the small peptides C3a and C5a, respectively (Morikis, D. -

Development and Validation of a Protein-Based Risk Score for Cardiovascular Outcomes Among Patients with Stable Coronary Heart Disease
Supplementary Online Content Ganz P, Heidecker B, Hveem K, et al. Development and validation of a protein-based risk score for cardiovascular outcomes among patients with stable coronary heart disease. JAMA. doi: 10.1001/jama.2016.5951 eTable 1. List of 1130 Proteins Measured by Somalogic’s Modified Aptamer-Based Proteomic Assay eTable 2. Coefficients for Weibull Recalibration Model Applied to 9-Protein Model eFigure 1. Median Protein Levels in Derivation and Validation Cohort eTable 3. Coefficients for the Recalibration Model Applied to Refit Framingham eFigure 2. Calibration Plots for the Refit Framingham Model eTable 4. List of 200 Proteins Associated With the Risk of MI, Stroke, Heart Failure, and Death eFigure 3. Hazard Ratios of Lasso Selected Proteins for Primary End Point of MI, Stroke, Heart Failure, and Death eFigure 4. 9-Protein Prognostic Model Hazard Ratios Adjusted for Framingham Variables eFigure 5. 9-Protein Risk Scores by Event Type This supplementary material has been provided by the authors to give readers additional information about their work. Downloaded From: https://jamanetwork.com/ on 10/02/2021 Supplemental Material Table of Contents 1 Study Design and Data Processing ......................................................................................................... 3 2 Table of 1130 Proteins Measured .......................................................................................................... 4 3 Variable Selection and Statistical Modeling ........................................................................................ -

Structural and Functional Analysis of Complement Factor H: a Crucial Protein in Several Disorders
UNIVERSITÀ DEGLI STUDI DI MILANO SCUOLA DI DOTTORATO IN MEDICINA MOLECOLARE CICLO XXVII Anno Accademico 2013/2014 TESI DI DOTTORATO DI RICERCA settore scientifico disciplinare: BIO13 STRUCTURAL AND FUNCTIONAL ANALYSIS OF COMPLEMENT FACTOR H: A CRUCIAL PROTEIN IN SEVERAL DISORDERS Dottorando : Silvia BERRA Matricola N° R09657 TUTORE: Prof. Alberto CLIVIO COORDINATORE DEL DOTTORATO: Prof. Mario CLERICI Sommario Il Fattore H del complemento (FH) è un importante regolatore della via alternativa del complemento: protegge infatti le cellule dell’ospite dall’attacco del sistema del complemento e carenze di FH sia qualitative e quantitative dovute a mutazioni nel gene CFH sono spesso associate ad una serie di malattie umane, come la glomerulonefrite membranoproliferativa (MPGN), la sindrome emolitico-uremica atipica (aHUS) e la degenerazione maculare della retina legata all’età (AMD). Mentre esiste una caratterizzazione genetica per tutte queste malattie, i dati funzionali a livello di proteine sono spesso carenti. Inoltre, il FH gioca un ruolo significativo nelle malattie infettive: molti agenti patogeni sono infatti in grado di reclutare il FH sulla loro superficie sfruttandolo per proteggersi dagli attacchi del complemento. Mentre per alcuni agenti patogeni l'interazione con il FH è stata ben descritta, per gli altri gli "interattori" diretti sono ancora sconosciuti. Tuttavia, lo studio del FH è complicato dalla presenza di proteine FH-related (FHRs) che posseggono un elevato grado di somiglianza con il FH e ne rendono quindi difficile la purificazione e la analisi diretta. Il primo obiettivo di questo progetto è stato lo sviluppo di saggi quantitativi e funzionali FH-specifici, utilizzando un anticorpo monoclonale (Mab 5H5) prodotto nel nostro laboratorio, che si è dimostrato essere specifico per FH. -

Factor D Catalog Number
Name: Factor D Catalog Number: A136 Sizes Available: 25 µg/vial Concentration: 0.1 mg/mL (see Certificate of Analysis for actual concentration) Form: Frozen liquid Activity: >95% versus normal human serum standard Purity: >95% by SDS-PAGE Buffer: 10 mM sodium phosphate, 145 mM NaCl, pH 7.3 Extinction Coeff.: A280 nm = 1.1 at 1.0 mg/mL Molecular weight: 24,000 Da (single chain) Preservative: None, 0.22 µm filtered Storage: -70oC or below. Avoid freeze/thaw. Source: Normal human serum (shown by certified tests to be negative for HBsAg and for antibodies to HCV, HIV-1 and HIV-II). Precautions: Use normal precautions for handling human blood products. Origin: Manufactured in the USA. General Description Factor D is a glycosylated protein composed of a single 24,000 Da polypeptide chain. It is an essential component of the alternative pathway of complement activation. Its only known function is to cleave and activate factor B when factor B is bound to C3b or a C3b-like protein such as C3(H2O) or CVF. Factor D is a serine protease that circulates as a mature protease, but it exhibits a highly restricted specificity and it appears to be substrate activated. Factor D cleaves factor B bound to C3b between Arg233 and Lys234 causing the release of the Ba fragment (33,000 Da) and leaving the 60,000 Bb fragment bound to C3b. The C3b,Bb complex is called a C3 or C5 convertase because it converts these proteins to their active forms by cleaving off the small peptides C3a and C5a, respectively (Law, S.K.A. -
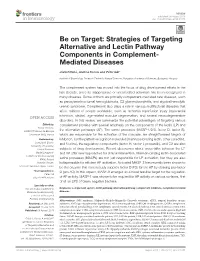
Strategies of Targeting Alternative and Lectin Pathway Components in Complement- Mediated Diseases
REVIEW published: 08 August 2018 doi: 10.3389/fimmu.2018.01851 Be on Target: Strategies of Targeting Alternative and Lectin Pathway Components in Complement- Mediated Diseases József Dobó, Andrea Kocsis and Péter Gál* Institute of Enzymology, Research Centre for Natural Sciences, Hungarian Academy of Sciences, Budapest, Hungary The complement system has moved into the focus of drug development efforts in the last decade, since its inappropriate or uncontrolled activation has been recognized in many diseases. Some of them are primarily complement-mediated rare diseases, such as paroxysmal nocturnal hemoglobinuria, C3 glomerulonephritis, and atypical hemolytic uremic syndrome. Complement also plays a role in various multifactorial diseases that affect millions of people worldwide, such as ischemia reperfusion injury (myocardial infarction, stroke), age-related macular degeneration, and several neurodegenerative disorders. In this review, we summarize the potential advantages of targeting various Edited by: complement proteins with special emphasis on the components of the lectin (LP) and Nicole Thielens, UMR5075 Institut de Biologie the alternative pathways (AP). The serine proteases (MASP-1/2/3, factor D, factor B), Structurale (IBS), France which are responsible for the activation of the cascade, are straightforward targets of Reviewed by: inhibition, but the pattern recognition molecules (mannose-binding lectin, other collectins, Cordula M. Stover, and ficolins), the regulatory components (factor H, factor I, properdin), and C3 are also University of Leicester, United Kingdom subjects of drug development. Recent discoveries about cross-talks between the LP Maciej Cedzynski, and AP offer new approaches for clinical intervention. Mannan-binding lectin-associated Institute for Medical Biology (PAN), Poland serine proteases (MASPs) are not just responsible for LP activation, but they are also Christian Drouet, indispensable for efficient AP activation. -
Role of Complement in Diabetes
This is a repository copy of Role of complement in diabetes. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/151783/ Version: Accepted Version Article: Ajjan, RA and Schroeder, V (2019) Role of complement in diabetes. Molecular Immunology, 114. pp. 270-277. ISSN 0161-5890 https://doi.org/10.1016/j.molimm.2019.07.031 (c) 2019, Elsevier Ltd. This manuscript version is made available under the CC-BY-NC-ND 4.0 license https://creativecommons.org/licenses/by-nc-nd/4.0/ Reuse This article is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs (CC BY-NC-ND) licence. This licence only allows you to download this work and share it with others as long as you credit the authors, but you can’t change the article in any way or use it commercially. More information and the full terms of the licence here: https://creativecommons.org/licenses/ Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Molecular Immunology, Special Issue EMCHD 2019 Review Article Role of Complement in Diabetes Ramzi A. Ajjan a, Verena Schroeder b* a Leeds Institute for Cardiovascular and Metabolic Medicine, School of Medicine, University of Leeds, Leeds, United Kingdom b Experimental Haemostasis Group, Department for BioMedical Research (DBMR), University of Bern, Bern, Switzerland * Corresponding author: Verena Schroeder Experimental Haemostasis Group Department for BioMedical Research (DBMR) University of Bern Murtenstrasse 40 3008 Bern Switzerland Tel.: +41 31 632 9618 E-mail: [email protected] 1 Abstract Accumulating evidence suggests a role for the complement system in the pathogenesis of diabetes and the vascular complications that characterise this condition.