7Th CRM Karnataka State Debreifing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

13Th FINANCE BASIC GRANTS 2Nd INSTALLMENT 2014-15 RDP 14
13th FINANCE BASIC GRANTS 2nd INSTALLMENT 2014-15 RDP 14 GPS 2015, Dt: 27-03-2015 HAVERI-–ಾೇ District Name Taluk Name GP Code GP Name GP Name Bank Details Branch Name IFSC Code Bank Account GP (Kannada) Number Share (In Rs.) HAVERI- BYADGI-ಾÎಡ 1517001013 BANNIHATTI ಬಹ Karnataka Byadgi KVGB0007001 17196082826 –ಾೇ Vikasa Grameena Bank 392187 HAVERI- BYADGI-ಾÎಡ 1517001012 BISALHALLI ಸಲಹ Karnataka Byadgi KVGB0007001 17196082871 –ಾೇ Vikasa Grameena Bank 476862 HAVERI- BYADGI-ಾÎಡ 1517001020 BUDAPANAHALLI ಬುಡಪನಹ Karnataka Byadgi KVGB0007001 17196082859 –ಾೇ Vikasa Grameena Bank 456346 HAVERI- BYADGI-ಾÎಡ 1517001002 CHIKKABASUR ಕ“ಾಸೂರು Karnataka Chikkabasur KVGB0007002 17069072744 –ಾೇ Vikasa Grameena Bank 389353 HAVERI- BYADGI-ಾÎಡ 1517001003 GHALAPUJI ಳಪ§ Karnataka Chikkabasur KVGB0007002 17069072755 –ಾೇ Vikasa Grameena Bank 309676 HAVERI- BYADGI-ಾÎಡ 1517001018 GUNDENAHALLI ಗುಂೇನಹ Karnataka Motebennur KVGB0007005 17082057140 –ಾೇ Vikasa Grameena Bank 312213 HAVERI- BYADGI-ಾÎಡ 1517001009 HEDIGGONDA ೆ!"ೊಂಡ Karnataka Kaginele KVGB0007004 17077570794 –ಾೇ Vikasa Grameena Bank 316465 HAVERI- BYADGI-ಾÎಡ 1517001004 HIREANAJI $ೕ%ೆಅಣ State Bank of Sudambi SBMY0040505 64062057889 –ಾೇ Mysore 403303 HAVERI- BYADGI-ಾÎಡ 1517001007 HIREHALLI $%ೇಹ Karnataka Chikkabasur KVGB0007002 17069072766 –ಾೇ Vikasa Grameena Bank 337280 HAVERI- BYADGI-ಾÎಡ 1517001014 KADARAMANDALAGI ಕದರಮುಂಡಲ* Karnataka Kadaramandalgi KVGB0007003 17077054226 –ಾೇ Vikasa Grameena Bank 433070 HAVERI- BYADGI-ಾÎಡ 1517001008 KAGINELE +ಾ*,ೆ ೆ Karnataka Kaginele KVGB0007004 17077570783 –ಾೇ Vikasa Grameena -
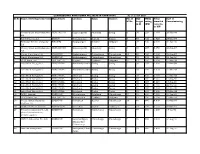
Sl No Name of Developer/Investor Manufcturer Location Taluk District Nos of Wtgs Hub Height in M Wegs Rating (KW) Total Installe
COMMISSIONED WIND POWER PROJECTS IN KARNATAKA As on 31.07.2021 Sl No Name of Developer/Investor Manufcturer Location Taluk District Nos of Hub WEGs Total Date of WTGs height rating installed Commissioning in M (KW) capacity in MW 1 Victory Glass And Industries NEPC-MICON Kappatagudda Mundargi Gadag 6 30 225 1.350 28-Mar-96 Ltd 2 R P G Telecom Ltd BONUS Hanumasagar Kustagi Koppal 6 40 320 1.920 27-Mar-97 3 Kirloskar Electric Company WEG(UK) Hargapurgad Hukkeri Belgaum 5 35 400 2.000 00-Jan-00 Ltd 4 Victory Glass And Industries NEPC-MICON Kappatagudda Mundargi Gadag 2 30 225 0.450 28-Sep-97 Ltd 5 Jindal Aluminium Ltd ENERCON Madakaripura Chitradurga Chitradurga 10 50 230 2.300 28-Sep-97 6 Jindal Aluminium Ltd ENERCON Madakaripura Chitradurga Chitradurga 8 50 230 1.840 09-Jan-98 7 ICICI Bank Ltd RES-AWT-27 Girgoan Chikkodi Belgaum 12 43 250 3.000 31-Mar-98 8 Indo Wind Energy Ltd NEPC-INDIA Mallasamudraum Gadag Gadag 8 30 225 1.800 31-Mar-98 9 Indo Wind Energy Ltd NEPC-INDIA Mallasamudraum Gadag Gadag 1 30 250 0.250 31-Mar-98 10 Indo Wind Energy Ltd NEPC-INDIA Belathadi Gadag Gadag 1 35 400 0.400 31-Mar-98 11 Indo Wind Energy Ltd NEPC-INDIA Belathadi Gadag Gadag 1 30 225 0.225 11-Sep-98 12 Indo Wind Energy Ltd NEPC-INDIA Belathadi Gadag Gadag 1 30 225 0.225 18-Sep-98 13 Indo Wind Energy Ltd NEPC-INDIA Belathadi Gadag Gadag 1 35 400 0.400 26-Nov-98 14 Indo Wind Energy Ltd NEPC-INDIA Belathadi Gadag Gadag 1 35 400 0.400 10-Dec-98 15 Indo Wind Energy Ltd. -

All India Veerashavia Mahasabha (R.), Bangalore Pratibha Puraskara-2018-19(Sslc) Haveri Dist
ALL INDIA VEERASHAVIA MAHASABHA (R.), BANGALORE PRATIBHA PURASKARA-2018-19(SSLC) HAVERI DIST Sl No Name & Address Contact No. Total Scored % Remarks 1 SINDHU BASAVARAJ HAVERI D/O BASAVARAJ 9916530552 625 617 98.72 HAVERI AT.HONKAN POST.SHESHAGIRI TQ.HANGAL DIST.HAVERI PIN.581102 2 DHANALAXMI MALLIKARJUNAPPA 6363056405 625 616 98.56 HUNASIKATTIPLOT ROAD AT YALLUR POST KARAGUDRI TQ HANGAL DIST HAVERI 3 Puneet S HiremathHiremath oni Shiggaon - 9113681395 625 616 98.56 581205 4 Srusti j KabbinakantimathDaneshwari Nagar 4th 9986232853 625 610 97.60 cross Heggeri road Haveri 5 MALLIKARJUNA KAREGOUDARAATPO KADUER 9964323637 625 609 97.44 TQ RATTIHALLI DIST HAVERI 6 SINDHU JAYAPPA NADAGOUDRAD/O JAYAPPA 8971934872 625 609 97.44 NADAGOUDRA HOSANAGAR 4TH CROSS HAVERI NEAR MASUTI HAVERI TQ-DIST HAVERI 581110 7 Bhoomika.V.aTilavalli Pincode:581120 8197857051 625 608 97.28 8 CHETAN G MUNDASAD1ST MAIN 1ST CROSS 9108740905 625 607 97.12 VIKAS NAGAR RANEBENNUR TQ RANEBENNUR DIST HAVERI 9 NIRANJAN PATILRudrugouda S Patil At 7899275613 625 605 96.80 Angaragatti, post Hosakatti Talluk Hirekerur, distic Haveri Pin code 581210 10 Spandana M MJ-3/2 Grasim Staff colony 9448319084 500 484 96.80 Kumarapatnam Ranebennur 11 AISHWARYA R SHIRSANGISIDDADEVAPURA 9035480250 625 604 96.64 PURADA ONI HAVERI TQ-DIST HAVERI 581110 12 Ananya Halappa GalapujiHalappa B Galapuji 9741858532 625 603 96.48 Post Gondi. TQ hanagal. 13 RANJITA U KUMMUR Ranjita U Kummur D /o 8722351297 625 603 96.48 Umesh kummur At /po Kabbur 581110 HAVERI 14 CHIDANANDA HANUMAGOUDA 7760250759 625 602 96.32 BEVINAHALLIAT.POST:ANAJI TQ:RATTIHALLI DI:HAVERI PIN:581111 15 KAVYA BASAVARAJ DEVAGIRI KAVYA. -

Karnataka Budget 2010-2011 Highlights
KARNATAKA BUDGET 2010-2011 HIGHLIGHTS Overview of Budget 2010-2011 (Rs. in Crores) • Total Receipts : 68,564 Revenue Receipts : 53,639 Capital Receipts : 14,925 • Total Expenditure : 70,063 Revenue Expenditure : 53,138 Capital Expenditure : 16,925 • Fiscal Deficit : 9708 (2.96 percent of GSDP) • Revenue Surplus : 500 (0.15 percent of GSDP) Allocations from Budget • The allocation for plan and non-plan expenditure of various departments from the State Budget is as follows: Agriculture & Horticulture Rs.2094 Crore Education & Higher Education Rs.10505 Crore Urban Development Rs. 5883 Crore Energy Rs.3547 Crore Irrigation Rs.5180 Crore RD&PR Rs.3442 Crore Public Works Rs.2909 Crore Revenue Rs.2764 Crore Health & Medical Education Rs.2673 Crore Home Rs.2345 Crore Social Welfare Rs.2671 Crore Women & Child Development Rs.1832 Crore Housing Rs. 928 Crore • High priority for social sector. o Education budget increased by Rs 1605 crore o Health budget up by Rs 384 crore. • Social services constitute 38 per cent of total expenditure while economic services will take 32 %. The balance will be used for general services and grant-in-aid to the local bodies. 1 State Plan Size • State Plan Size has been increased by 19 percent to Rs 31000 crore. It is among the largest plan size in per capita terms for the States. Major Sectors Agriculture and Allied Sectors • Support to farmers o Rs 2500 crore provided for supplying free electricity to irrigation pump sets and Bhagyajyothi/ Kuteerjyothi o Rs 320 crores provided for facilitating farmers to get subsidised loans from commercial banks and cooperative institutions o Scheme for special assistance of Rs 2 per litre of milk collected through cooperative institutions to be continued o Rs 100 crore for promoting organic farming o Rs 40 crore provided to continue Yashaswini scheme o Quantity of sales tax free diesel being provided to fishermen of coastal areas will be increased from 75000 to 85000 KL. -

HŒ臬 A„簧綟糜恥sµ, Vw笑n® 22.12.2019 Š U拳 W
||Om Shri Manjunathaya Namah || Shri Kshethra Dhamasthala Rural Development Project B.C. Trust ® Head Office Dharmasthala HŒ¯å A„®ãtÁS®¢Sµ, vw¯ºN® 22.12.2019 Š®0u®± w®lµu® îµ±°ªæX¯Š®N®/ N®Zµ°‹ š®œ¯‡®±N®/w®S®u®± š®œ¯‡®±N® œ®±uµÛ‡®± wµ°Š® wµ°î®±N¯r‡®± ªRq® y®‹°£µ‡®± y®ªq¯ºý® D Nµ¡®w®ºruµ. Cu®Š®ªå 50 î®±q®±Ù 50 Oʺq® œµX®±Ï AºN® y®lµu®î®Š®w®±Ý (¬šµ¶g¬w®ªå r¢›Š®±î®ºqµ N®Zµ°‹/w®S®u®± š®œ¯‡®±N® œ®±uµÛSµ N®xÇ®Õ ïu¯ãœ®Áqµ y®u®ï î®±q®±Ù ®±š®±é 01.12.2019 NµÊ Aw®æ‡®±î¯S®±î®ºqµ 25 î®Ç®Á ï±°Š®u®ºqµ î®±q®±Ù îµ±ªæX¯Š®N® œ®±uµÛSµ N®xÇ®Õ Hš¬.Hš¬.HŒ¬.› /z.‡®±±.› ïu¯ãœ®Áqµ‡µ²ºvSµ 3 î®Ç®Áu® Nµ©š®u® Aw®±„Â®î® î®±q®±Ù ®±š®±é 01.12.2019 NµÊ Aw®æ‡®±î¯S®±î®ºqµ 30 î®Ç®Á ï±°Š®u®ºqµ ) î®±±ºvw® œ®ºq®u® š®ºu®ý®Áw®NµÊ B‡µ±Ê ¯l®Œ¯S®±î®¼u®±. š®ºu®ý®Áw®u® š®Ú¡® î®±q®±Ù vw¯ºN®î®w®±Ý y®äqµã°N®î¯T Hš¬.Hº.Hš¬ î®±²©N® ¯Ÿr x°l®Œ¯S®±î®¼u®±. œ¯cŠ¯u® HŒ¯å A„®ãtÁS®¢Sµ A†Ãw®ºu®wµS®¡®±. Written test Sl No Name Address Taluk District mark Exam Centre out off 100 11 th ward near police station 1 A Ashwini Hospete Bellary 33 Bellary kampli 2 Abbana Durugappa Nanyapura HB hally Bellary 53 Bellary 'Sri Devi Krupa ' B.S.N.L 2nd 3 Abha Shrutee stage, Near RTO, Satyamangala, Hassan Hassan 42 Hassan Hassan. -

Hirekerur Bar Association : Hirekerur Taluk : Hirekerur District : Haveri
3/17/2018 KARNATAKA STATE BAR COUNCIL, OLD KGID BUILDING, BENGALURU VOTER LIST POLING BOOTH/PLACE OF VOTING : HIREKERUR BAR ASSOCIATION : HIREKERUR TALUK : HIREKERUR DISTRICT : HAVERI SL.NO. NAME SIGNATURE BANAKAR BASAVANNEPPA GADLAPPA MYS/55/58 1 S/O GADLAPPA BANAKAR HIREKERUR AT & PO HIREKERUR HIREKERUR HAVERI 581 111 TAMBAKAD JAGADISH BASAVENNAPPA KAR/78/77 2 S/O OPP: A OFFICE . DHARWAD . HIREKERUR HAVERI PALAXAPPA BASALINGAPPA BHOGAVI KAR/244/77 3 S/O BASALINGAPPA BHOGAVI AT PO: HUNSBHAVI , DHARWAD HIREKERUR HAVERI KABBINAKANTIMATH KARABASAYYA SIDDAPPAYYA KAR/334/77 4 S/O AT: CHAPPARADAHALLI P.O: HIREMORAB DHARWAD . HIREKERUR HAVERI 1/25 3/17/2018 SALI D.M. KAR/264/78 5 S/O MALLAPPA SALI JAWARAGI ,DHARWAD HIREKERUR HAVERI SUNAGAR BASAVARAJ KARIYAPPA KAR/404/78 6 S/O KARIYAPPA SUNAGAR RATIHALLI HIREKEHUR HIREKERUR HAVERI 581118 HOLIYAPPANAVAR BASAVARAJ MALLESHAPPA KAR/123/79 S/O MALLESHAPPA BASALINGAPPA 7 HOLIYAPPANAVR BASAVESWARA NAGAR ,3 RD CROSS, HIREKERUR HAVERI 581111 DUDIHALLI MAHANTESHAPPA BASAPPA KAR/64/81 S/O DUDIHALLI BASAPPA MALLAPPA 8 SOMANAHALLI TOVARAGI HIREKERUR DT DHARWAR HAVERI HAVERI KADEMANI NABISAHEB HUSENA SAHEB KAR/495/81 9 S/O HUSENASAHED KADEMANI BASAVESHWAR NAGAR HIREKERUR HAVERI 581111 2/25 3/17/2018 BANAKAR VJANESHWAR BASAVANNAPPA KAR/334/84 10 S/O BASAVANNAPPA C/O. BANAKAR B G MLS, DT DHARWAR HIREKERUR HAVERI 581 111 BANAKAR BASAVARAJ NAGAPPA KAR/311/85 S/O NAGAPPA GURULINGAPPA BANAKAR 11 B.N. BANAKAR ADVOCATE RAGHAVENDRA COLONY VIDYANAGAR HIREKERUR HAVERI 581 111 KARIYANNANAVAR SIDDALINGAPPA KARIYAPPA KAR/315/85 12 S/O KARIYANNANAVAR KHB COLONY , NAVANAGAR HIREKERUR HAVERI 581111 TIPPANNANAVAR SUBHAS KAR/457/85 13 S/O BASANAGOUDA VIDYANAGAR HIREKERUR HAVERI MALLIKARJUNAPPA P Y KAR/595/85 S/O SANNAYARAGUNTAPPA 14 NO.69, SREERAMAPRAKASH NILAYA, KUVEMPU NAGAR, HIIRIYUR TOWN , CHITRADURGA HIRIYUR CHITRADURGA 577598 3/25 3/17/2018 BASAVARAJ.N. -

KARNATAKA.Pdf
NATIONAL FEDERATION OF THE BLIND Plot No.-21,Sec-VI,M.B.Road,Pushp Vihar,New Delhi-110017 Membership List: KARNATAKA District: RACHUR S.N. I-Card No. Name & Address Disability Date of Renewal M.Type Membership Date 1 KA-H-059 (HANUMANTHA) HANAMANT BLIND 03/16/2018 07/25/2020 ORDINARY S/O SANNA RAMAYYA Age Renewal DOB GILLESUGAR GUNJAHALI RAICHUR Receipt No. KARNATAKA 584140 21 73882 2 KA-A-017 A GOPAL BLIND 03/14/2009 07/25/2020 ORDINARY S/O SH ANKAIAH Age Renewal DOB # 288 7th CROSS CHANMUNDI NAGAR HOSKERAHALLI BANASHANKARI 3RD Receipt No. STAGE BANGALORE - 56085 73102 3 KA-A-100 A N NAGESH BLIND 01/01/1970 07/25/2020 ORDINARY S/O A S NAGARAJ SHETTY Age Renewal DOB 6/1, SHESHA MALLIKA, 9 CROSS 4 MAIN OPPOSITE RENAISSANCE, POLASHA Receipt No. 01/01/1970 BANGALORE - 560003 74431 4 KA-A-041 A SANTOSH BLIND 05/10/2010 07/25/2020 ORDINARY S/O GURU MURTHY Age Renewal DOB OPP SHREE SHARDA DEVI ANDARA SCHOOL GOPALA POST SHIMONGA Receipt No. 73103 5 KA-A-086 A.M. THIRTHESHA BLIND 03/16/2018 07/25/2020 ORDINARY S/O A B MANJAPPA Age Renewal DOB #1044 6th Cross Hasanraste Balabaga Receipt No. Arsikere hassan Karatake 573103 38 73846 6 KA-A-099 ABDUL JAMEER BLIND 03/25/2019 07/25/2020 ORDINARY S/O ABDUL KARIM Age Renewal DOB DODDABELAVAGALA, BANGALORE, RIVAL, KARNATAKA - 561704 Receipt No. 01/01/1977 73847 7 KA-A-030 ABDUL RAHAMAN BLIND 03/10/2010 07/25/2020 ORDINARY S/O MOONDHANMIPPA Age Renewal DOB PERUGIDAD BHASPETHGALI LINDI TALUK BIJAPUR KARNATAKA Receipt No. -

Monthly Multidisciplinary Research Journal
Vol 5 Issue 10 July 2016 ISSN No : 2249-894X ORIGINAL ARTICLE Monthly Multidisciplinary Research Journal Review Of Research Journal Chief Editors Ashok Yakkaldevi Ecaterina Patrascu A R Burla College, India Spiru Haret University, Bucharest Kamani Perera Regional Centre For Strategic Studies, Sri Lanka Welcome to Review Of Research RNI MAHMUL/2011/38595 ISSN No.2249-894X Review Of Research Journal is a multidisciplinary research journal, published monthly in English, Hindi & Marathi Language. All research papers submitted to the journal will be double - blind peer reviewed referred by members of the editorial Board readers will include investigator in universities, research institutes government and industry with research interest in the general subjects. Regional Editor Manichander Thammishetty Ph.d Research Scholar, Faculty of Education IASE, Osmania University, Hyderabad. Advisory Board Kamani Perera Delia Serbescu Mabel Miao Regional Centre For Strategic Studies, Sri Spiru Haret University, Bucharest, Romania Center for China and Globalization, China Lanka Xiaohua Yang Ruth Wolf Ecaterina Patrascu University of San Francisco, San Francisco University Walla, Israel Spiru Haret University, Bucharest Karina Xavier Jie Hao Fabricio Moraes de AlmeidaFederal Massachusetts Institute of Technology (MIT), University of Sydney, Australia University of Rondonia, Brazil USA Pei-Shan Kao Andrea Anna Maria Constantinovici May Hongmei Gao University of Essex, United Kingdom AL. I. Cuza University, Romania Kennesaw State University, USA Romona Mihaila Marc Fetscherin Loredana Bosca Spiru Haret University, Romania Rollins College, USA Spiru Haret University, Romania Liu Chen Beijing Foreign Studies University, China Ilie Pintea Spiru Haret University, Romania Mahdi Moharrampour Nimita Khanna Govind P. Shinde Islamic Azad University buinzahra Director, Isara Institute of Management, New Bharati Vidyapeeth School of Distance Branch, Qazvin, Iran Delhi Education Center, Navi Mumbai Titus Pop Salve R. -

1 : in the High Court of Karnataka Dharwad Bench
: 1 : IN THE HIGH COURT OF KARNATAKA DHARWAD BENCH DATED THIS THE 28 TH DAY OF JANUARY 2015 BEFORE THE HON’BLE MR.JUSTICE A.N.VENUGOPALA GOWDA WRIT PETITION No.2918/2008 [L.A.RES] BETWEEN 1. KRISHNACHAR S/O.NARASIMHACHAR ADAVANI, AGED 78 YEARS,OCC:AGRICULTURE, R/O.RATTIHALLI,HIREKERUR TALUK, HAVERI DISTRICT. 2. N S PATIL, AGED 56 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI,HIREKERUR TALUK, HAVERI DISTRICT. 3. H R DODDAMANI URF PINJAR AGED 70 YEARS, OCC:AGRICULTURE, R/O.SHIRAGAMBI,HIREKERUR TALUK, HAVERI DISTRICT. 4. M PINJAR, AGED 72 YEARS, OCC:AGRICULTURE, R/O.SHIRAGAMBI,HIREKERUR TALUK, HAVERI DISTRICT. 5. SMT L R MADIVALAR AGED 60 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI,HIREKERUR TALUK, HAVERI DISTRICT. : 2 : 6. S S BASARIHALLI AGED 65 YEARS, OCC:AGRICULTURE, R/O.SHIRAGUMBI,HIREKERUR TALUK, HAVERI DISTRICT. 7. M S BASARIHALLI AGED 72 YEARS, OCC:AGRICULTURE, R/O.SHIRAGUMBI,HIREKERUR TALUK, HAVERI DISTRICT. 8. R S BASARIHALLI AGED 70 YEARS, OCC:AGRICULTURE, R/O.SHIRAGUMBI, HIREKERUR TALUK, HAVEREI DISTRICT. 9. S M HOLIJOGI AGED 55 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI, HIREKERUR TALUK, HAVEREI DISTRICT. 10. K S HOLIJOGI URF CHADDER AGED 60 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI, HIREKERUR TALUK, HAVEREI DISTRICT. 11. B M HOLIJOGI AGED 60 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI, HIREKERUR TALUK, HAVEREI DISTRICT. : 3 : 12. K S BANAKAR AGED 45 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI, HIREKERUR TALUK, HAVEREI DISTRICT. 13. R I GONEPPANAVAR AGED 33 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI, HIREKERUR TALUK, HAVEREI DISTRICT. 14. S P GONEPPANAVAR AGED 53 YEARS, OCC:AGRICULTURE, R/O.RATTIHALLI, HIREKERUR TALUK, HAVEREI DISTRICT. -

Haveri Dist.Xlsx
All India Veerashaiva Mahasabha (R.) Bangalore Haveri Dist Voters List S.No Reg No/MEM No Name & Address 1 2277 Siddalingappa AraniShivappa Akkipet, Haveri Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:9448823126 2 3284 Eshwaraiah ShivaputhrayyaShidaganti No.10, A Block, 11th Cross, Basaveshwaranagar Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:9448086895 3 5086 Basavaraj MallappaBaradur Yalakki Oni, Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:9449925290 4 6188 RudrappaNagappaAraganji Rajendranagar Haveri Taluk:Haveri District:Haveri State:Karnataka-500030 Mobile:8105743609 5 6933 Basavaraj B.Nadavalamani Basaveshwara Nagar, B Block, 11th Cross, Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:7019190991 6 6934 Geetha B.Nadavalamani Basaveshwaranagar, B Block, 11th Corss, Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:8310691577 7 6936 Sujatha H.Holalada Basaveshwaranagar, 9th Cross, A Block, Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:9448065401 8 6937 Akshatha B. Holalada Basaveshwaranagar, 9th Cross, A Block, Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:7829650733 9 6938 Sujatha C.Maragur Basaveshwaranagar, 9th Cross, A Block, Haveri Taluk:Haveri District:Haveri State:Karnataka-581110 Mobile:9886556547 10 6944 Jagadish Ankalakoti Post-Guttal, SMS Maha Vidyalaya, Shivayogishwara Nagar Guttal Taluk:Haveri District:Haveri State:Karnataka-581108 Mobile:9535479417 11 6945 Anupama Ankalakoti Post-Guttal, -

Role of Haveri District Leaders in the National Movement – a Case Study
© 2019 JETIR June 2019, Volume 6, Issue 6 www.jetir.org (ISSN-2349-5162) Role of Haveri District Leaders in the National Movement – A case study * Mamata Sawakar, Asst Professor, Dept of Political Science, Govt First Grade College,Ranebennur **Dr.Prasannakumar.K, Asst Professor, Dept of Political Science, Sahyadri Arts & Commerce College, Shimoga. Abstract Haveri district is exactly in the center of Karnataka with equal distance from Bidar in the far north to Kollegal in the far south. It is also known as the gateway district to the northern districts of Karnataka. Haveri district has a very rich culture and tradition. The district is proud to be the birth place of Santa Shishunala Sharif, great saint Kanakadasaru, Sarvagnya, Hanagal Kumara Shivayogigalu, Wagish Panditaru, Writer Galaganatharu, Ganayogi Panchakshari Gavayigalu, Gnyana Peetha Awardee Dr.V.K.Gokak and many more. The freedom fighter Mailara Mahadevappa, who resisted British rule, is from Motebennur in Haveri District. Another freedom fighter Gudleppa Hallikere a native of Hosaritti is also from this district. He started a residential school Gandhi Grameen Gurukul in Hosaritti. During the Quit India Movement, Gandhiji gave the clarion call ‘Do or die’. A great movement to oust the British was unleashed. Mahadevappa lead the movement of South division of Dharwad. He started Kara Nirakarane i.e. refusal to pay land revenue movement. He encouraged farmers not to pay land revenue to the Government. This movement spread like wild fire. The lands of those peasants who did not pay taxes were confiscated. Meanwhile, some peasants joined hands with the British and purchased those confiscated lands. -

Department of Animal Husbandry and Veterinary Services
Department of Animal Husbandry and Veterinary services Details of Hospital Co-ordinates to be submitted to AH&VS Helpline District name : Haveri Name of the SL.NO Taluk Name Name of the Hospital (VH, VD, PVC) Contact Number Doctor Dr.Santosh 1 Hangal V D Kusanur 7411108998 Malagund https://goo.gl/maps/SSRQUc5a4Fa32Ypt9 Dr.Santosh 2 Hangal V D Belagalpet Malagund 7411108998 (incharge) https://goo.gl/maps/Z3oGx9cUdvNu1sLD9 Dr.Suresh 3 Hangal V D Adur Magod 9986546509 (incharge) https://goo.gl/maps/BbohjuLagXxXYYyV9 Dr.Suresh 4 Hangal V D Shiragod Magod 9986546509 (incharge) https://goo.gl/maps/dqzRRQdjJ2tCg51h9 Dr.Santosh 5 Hangal V D Araleshwara Malagund 7411108998 (incharge) https://goo.gl/maps/AGCX4yiNNnn3HfQi7 Dr.Santosh 6 Hangal V D Shyadaguppi Malagund 7411108998 (incharge) https://goo.gl/maps/nNupo8wQ6eWzcAwo7 Dr.Santosh 7 Hangal V D Kanchinegalur Malagund 7411108998 (incharge) https://goo.gl/maps/pdghFsE5bzH26nhX6 Dr.Suresh 8 Hangal V D Herur Magod 9986546509 (incharge) https://goo.gl/maps/XZctoC8JocdSowHx9 Dr.Girish 9 Hangal PVC Somasagar Radder 9901118508 (incharge) https://goo.gl/maps/z3uuMLCrzqXyMXpr8 Dr.Santosh 10 Hangal V H Bommanahalli Malagund 7411108998 (incharge) https://goo.gl/maps/i3naV4Pwm21RLxzM9 Dr.Girish 11 Hangal V H Hangal Radder 9901118508 (incharge) https://goo.gl/maps/VNK31yw7afHPygJFA Dr.Girish 12 Hangal V D Akkivalli 9901118508 Radder https://goo.gl/maps/dx4JTzoLAF4Vy3Vt8 Dr.Suresh 13 Hangal V D Chikkoushihosur Magod 9986546509 (incharge) https://goo.gl/maps/U9eHgBGrFZA2q7qm6 Dr.Suresh 14 Hangal V D Hirehullal