Reimagining the 1918 Pandemic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1918/19: 100 Years On
ESSAYS Ewald Frie 1918/19: 100 YEARS ON Open Futures 1918/19 – War and victory, collapse and defeat, revolution and reform, peace and re- organisation, civil war and violence, famine and Spanish flu and much else. The elements can be separated analytically, and many of them have been analysed individually in a historical context. They have been interpreted and incorporated into the narratives of revolution research, the history of warfare and violence, peace research, the history of diseases and epidemics. But the historical dynamics of 1918/19 resulted from the interplay of the various elements in very different constellations. 1918/19 is therefore a challeng- ing anniversary for a historical scholarship that is exploring new conceptual territory: – spatially: leaving the construct of the nation state and instead ›playing with scales‹1 from the local to the global; – temporally: departing from era- and progress-based master narratives and instead ›zooming in and out‹ and playing with temporal perspectives;2 – conceptually: departing from conceptual constructs due to the blurring of categories like ›crisis‹3 or ›revolution‹4 and instead focusing on a broad range of phenomena of social transformation on the premise of ›multidimensional understandings of emergence and destabilization‹.5 1 E.g. James Retallack (ed.), Imperial Germany 1871–1918, Oxford 2008. 2 E.g. Emily S. Rosenberg (ed.), A World Connecting. 1870–1945, Cambridge 2012 (A History of the World, ed. by Akira Iriye and Jürgen Osterhammel). 3 Cf. Thomas Mergel (ed.), Krisen verstehen. Historische und kulturwissenschaftliche Annäherungen, Frankfurt a.M. 2012, pp. 9-22, and the Leibniz Research Alliance ›Crises in a Globalised World‹: <http://www.leibniz-krisen.de/en/start/>. -
FEATURE the Forgotten Chinese Army in WWI Or Centuries, the Roots of Cheng Ling’S Populations Were Depleted
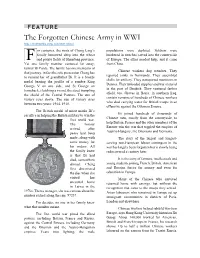
FEATURE The Forgotten Chinese Army in WWI http://multimedia.scmp.com/ww1-china/ or centuries, the roots of Cheng Ling’s populations were depleted. Soldiers were family burrowed deep into the wheat hunkered in trenches carved into the countryside F and potato fields of Shandong province. of Europe. The allies needed help, and it came Yet one family member ventured far away, from China. farmer Bi Cuide. The family has one memento of Chinese workers dug trenches. They that journey, in fact the sole possession Cheng has repaired tanks in Normandy. They assembled to remind her of grandfather Bi. It is a bronze shells for artillery. They transported munitions in medal bearing the profile of a sombre King Dannes. They unloaded supplies and war material George V on one side, and St George on in the port of Dunkirk. They ventured farther horseback, clutching a sword, the steed trampling afield, too. Graves in Basra, in southern Iraq, the shield of the Central Powers. The sun of contain remains of hundreds of Chinese workers victory rises above. The sun of victory rises who died carrying water for British troops in an between two years: 1914, 1918. offensive against the Ottoman Empire. The British medal of merit marks Bi’s Bi joined hundreds of thousands of sacrifice in helping the British military to win the Chinese men, mostly from the countryside, to first world war. help Britain, France and the other members of the The honour Entente win the war that toppled the empires of arrived after Austria-Hungary, the Ottomans and Germany. -

The Forgotten Fronts the First World War Battlefield Guide: World War Battlefield First the the Forgotten Fronts Forgotten The
Ed 1 Nov 2016 1 Nov Ed The First World War Battlefield Guide: Volume 2 The Forgotten Fronts The First Battlefield War World Guide: The Forgotten Fronts Creative Media Design ADR005472 Edition 1 November 2016 THE FORGOTTEN FRONTS | i The First World War Battlefield Guide: Volume 2 The British Army Campaign Guide to the Forgotten Fronts of the First World War 1st Edition November 2016 Acknowledgement The publisher wishes to acknowledge the assistance of the following organisations in providing text, images, multimedia links and sketch maps for this volume: Defence Geographic Centre, Imperial War Museum, Army Historical Branch, Air Historical Branch, Army Records Society,National Portrait Gallery, Tank Museum, National Army Museum, Royal Green Jackets Museum,Shepard Trust, Royal Australian Navy, Australian Defence, Royal Artillery Historical Trust, National Archive, Canadian War Museum, National Archives of Canada, The Times, RAF Museum, Wikimedia Commons, USAF, US Library of Congress. The Cover Images Front Cover: (1) Wounded soldier of the 10th Battalion, Black Watch being carried out of a communication trench on the ‘Birdcage’ Line near Salonika, February 1916 © IWM; (2) The advance through Palestine and the Battle of Megiddo: A sergeant directs orders whilst standing on one of the wooden saddles of the Camel Transport Corps © IWM (3) Soldiers of the Royal Army Service Corps outside a Field Ambulance Station. © IWM Inside Front Cover: Helles Memorial, Gallipoli © Barbara Taylor Back Cover: ‘Blood Swept Lands and Seas of Red’ at the Tower of London © Julia Gavin ii | THE FORGOTTEN FRONTS THE FORGOTTEN FRONTS | iii ISBN: 978-1-874346-46-3 First published in November 2016 by Creative Media Designs, Army Headquarters, Andover. -

The Spanish Flu
through electron microscopes, would that actually than normal for the elderly. The common have empowered them to halt the pandemic? explanation is that this strain of influenza was so There was no cure for the disease then, or now. new that it startled its victims' immune systems Vaccines? Another generation would pass before into overreaction, and the more vigorous the even partially effective vaccines against victim, the greater and deadlier the overreaction. influenza were developed. Even if all the The defensive swelling of membranes and knowledge and technology to produce flu increased secretion of fluids of the respiratory vaccine had been at hand in 1918, would it have system went to extremes in young adults, filling been possible to produce it in sufficient quantity their lungs with liquid until they drowned. and to distribute it across oceans and continents Overstimulation of the immune system is a in time to stop the swiftly spreading breath- plausible theory, but we could subject it to borne pandemic? Even today, when similar rigorous testing only if something like the 19 18 questions are asked each time a new virus returned. strain of the virus appears, the answer falls short of This distinctive influenza epidemic swept over being a confident "yes.” the world in three major waves during 1918 and 1919. We cannot be sure where and when the The influenza of the 1900s is still something of an initial wave in the spring of 1918 started, but the enigma, but the influenza that was sweeping around earliest scientific and statistical evidence points the world at the time of the Armistice ending to the United States in March 1918. -

The Role of Pawnshops in Risk Coping in Early Twentieth-Century Japan∗ Tatsuki Inoue†
The role of pawnshops in risk coping in early twentieth-century Japan∗ Tatsuki Inoue† Abstract This study examines the role of pawnshops as a risk-coping device in prewar Japan. Using data on pawnshop loans for more than 250 municipalities and exploiting the 1918–1920 influenza pandemic as a natural experiment, we find that the adverse health shock increased the total amount of loans from pawnshops. This is because those who regularly relied on pawnshops borrowed more money from them than usual to cope with the adverse health shock, and not because the number of people who used pawnshops increased. Keywords: Pawnshop; Risk-coping strategy; Borrowing; Influenza pandemic; Prewar Japan ∗ I would like to express my gratitude to Tetsuji Okazaki, Kota Ogasawara, and participants at the Economic History Society Annual Conference 2019 at Queen’s University Belfast and 2019 Japanese Economic Association Spring Meeting at Musashi University for their helpful comments. This work was supported by Grant-in-Aid for JSPS Fellows (Grant Number: 17J03825). Any errors are my own. † Graduate School of Economics, The University of Tokyo, Akamon General Research Building, 3F 353, 7-3-1, Hongo, Bunkyo-ku, Tokyo 113-0033, Japan. E-mail: inoue- [email protected]. 1 Introduction Most industrialized countries were characterized by huge income inequality before World War II (Piketty 2014). Since formal systems of social insurance were underdeveloped, the poor were more vulnerable to unforeseen accidents such as illness than today’s poor people in developed countries. Furthermore, an increase in migration removed people from the traditional informal social insurance systems provided by their local communities (Gorsky 1998). -

The Spanish Flu and the First World War: a Historical Analysis of the Pandemic’S Impact on the Conduct of War and Its Lessons for the British Army of 2020
CHACR IN DEPTH BRIEFING CIRCULATION: PUBLIC 6 MAY 2020 The Spanish Flu and the First World War: A Historical Analysis of the Pandemic’s Impact on the Conduct of War and its Lessons for the British Army of 2020 Soldiers from Fort Riley, Kansas, ill with Spanish flu at a hospital ward at Camp Funston . From Otis Historical Archives, National Museum of Health and Medicine The influenza pandemic, also known as the Spanish Flu, which hit the World the 1918 and last- ed until 1920, was the deadliest outbreak of disease in the 20th century. The aim of this study is to analyse the impact that the pandemic had on the belligerent nations of the First World War and, in particular, their armies. How were the armies affected, what impact did the pan- demic have on the ability to fight, and what measures did the armies take to contain the vi- rus? Last, but not least, the study will offer some possible consequences and lessons for the British Army of today. Considering that CHACR supports the British Army, it is fitting that the emphasis lies on the UK experience of the Spanish Flu; however, other armies and nations are also taken into consideration to present a more all-encompassing picture of the situation and challenges that the Spanish Flu presented at the end of the First World War. IN DEPTH BRIEFING Page 2 In order to answer the questions above, the study is divided into three parts. Part one presents an overview of the Spanish Flu pandemic and thus provides the context for the following parts. -

Trench Art and the Story of the Chinese Labour Corps in the Great
© James Gordon-Cumming 2020 All rights reserved. First published on the occasion of the exhibition Western Front – Eastern Promises Photography, trench art and iconography of the Chinese Labour Corps in the Great War hosted at The Brunei Gallery, SOAS University of London 1st October to 12th December 2020 No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the permission of the publisher, James Gordon-Cumming. Front cover: Collecting stores for the long journey ahead © WJ Hawkings Collection, courtesy John de Lucy 2 Page Contents A New Republic ..................................................................................................................... 5 A War Like No Other ........................................................................................................... 7 The Chinese Solution ......................................................................................................... 9 The Journey to Europe .................................................................................................... 10 Across Canada ..................................................................................................................... 13 In support of the war machine ..................................................................................... 14 From Labourer to Engineer ........................................................................................... -

Synopsis for Wei Hai Wei, China, 1895-1949
Synopsis for Wei Hai Wei, China, 1895-1949 Mission: The postal history of Wei Hai Wei (WHW) and the island of Liu Kung Tau (LKT) for the period 1895-1949 is shown in this exhibit. Treatment: The exhibit starts with forerunners before the first Japanese Occupation in 1895-98 and ends at the formation of the Peoples Republic of China in October 1949. Grouped by different post offices, yet sometimes operating in parallel, and its markings and/or usages, the exhibit is presented in chronological order within the chapters. A chapter has been included under the British PO for the correspondence of the High Commissioner of WHW, Sir James Stewart Lockhart, with his daughter, plus other covers that were addressed to him. Chapters for special historical events, like the Boxer Rebellion, Chinese Labour Corps, both Japanese Occupation were also included, closing with the Communist taking over after WWII and ending with the formation of the Peoples Republic of China. This is a well-balanced exhibit covering every time period of WHW’s postal history and history, with in-depth examples shown for each period. The examples shown are selected for its rarity and its significance to postal history and history. Importance: In a political sense, WHW was the most important stronghold of Britain in Northern China and only second to Hong Kong for all of China. In a philatelic sense, its postal history included many “China’s one-of”. For example, the only Courier Post in China, the Chinese Labour Corps of WWI, the only Chinese city that has been invaded and occupied by the Japanese ‘twice’ in its history, i.e. -

“Pandemic 1918” Study Guide Questions
“Pandemic 1918” Study Guide Questions “Pandemic 1918!” is an article about the experiences of King County residents during the influenza pandemic of 1918-1919. The virus, nicknamed the Spanish Flu, arrived just as the First World War was ending. It is thought to have infected over 500 million people worldwide. This activity is designed for readers in 7th grade and above. Questions can be used for discussion or as writing prompts. You can find the original article from December 2014 on Renton History Museum’s Newsletters Page. 1. Today’s scientists and historians are not sure where the Spanish Flu originated, but it is unlikely that it actually began in Spain. Why was the epidemic called the Spanish Flu? 2. How did health officials in the state of Washington prepare for the arrival of the Spanish Flu? 3. Jessie Tulloch observed firsthand how Seattle adapted to the flu. How did everyday life in Seattle change? 4. On November 11, 1918, the Allied Powers and Germany signed a treaty that officially brought World War I to a close. This day was called Armistice Day, and in modern times it is celebrated as Veteran’s Day in the United States. Why was the first Armistice Day a concern for public health officials? 1 5. According to health officials at the time, the best place for treating the Spanish Flu was at home. Patients were treated in their homes with the aid of family members and traveling nurses and doctors. However, some of the infected individuals had to go to Renton Hospital for treatment. -

China in the First World War: a Forgotten Army in Search of International Recognition
Contemporary Chinese Political Economy and Strategic Relations: An International Journal Vol. 3, No. 3, Dec. 2017, pp. 1237-1269 __________________________________________________________ China in the First World War: A Forgotten Army in Search of International Recognition Roy Anthony Rogers* University of Malaya Nur Rafeeda Daut** Kansai Gaidai University Abstract The First World War (1914-1918) has been widely considered as a European conflict and a struggle for dominance among the European empires. However, it is important to note that non-European communities from various parts of the world such as the Chinese, Indians, Egyptians and Fijians also played significant roles in the war. This paper intends to provide an analysis of the involvement of China in the First World War. During the outbreak of the war in 1914, the newly established Republic of China (1912) encountered numerous problems and uncertainties. However, in 1917 the Republic of China entered the First World War, supporting the Allied Forces, with the aim of elevating its international position. This paper focuses on the treatment that China had received from the international community such as Britain, the United States, France and Japan after the war. Specifically, this paper 1237 1238 Roy Anthony Rogers and Nur Rafeeda Daut argues that the betrayal towards China by the Western powers during the Paris Peace Conference and the May Fourth Movement served as an intellectual turning point for China. It had triggered the radicalization of Chinese intellectual thoughts. In addition, China’s socialization during the Paris Peace Conference had been crucial to the conception of the West’s negative identity in the eyes of the Chinese that has remained in the minds of its future leaders. -

Thesis FINAL VERSION Main Body
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ScholarBank@NUS A PLAGUE O’ BOTH YOUR HOUSES: MEDICINE, POWER, AND THE GREAT FLU OF 1918-1919 IN BRITAIN AND SINGAPORE LEE NURENEE (B.A. (Hons.), NUS A THESIS SUBMITTED FOR THE DEGREE OF MASTER OF ARTS DEPARTMENT OF HISTORY NATIONAL UNIVERSITY OF SINGAPORE 2011 Acknowledgements * To A/P Tim Barnard, for agreeing to supervise me and for giving me the latitude to grow as a researcher as well as the guidance to develop as a historian. I am grateful for his insights into the field of environmental history, and for his timely and useful feedback. This venture into the morbid stuff of the past would not have been possible without his support. To all my professors, who have taught and mentored me towards becoming a better student, historian, researcher, and tutor. The work done at the graduate level can be intense and isolating, but a few people really helped me make sense of the whole process. For their constructive criticism, advice, words of encouragement, and suggestions on various potentialities of research, I have Prof. Merle Ricklefs, Dr. Mark Emmanuel, Dr. Quek Ser Hwee, and Dr. Susan Ang to thank. To my fellow denizens of the History grad room – purveyors of fine humour and junk food (and oftentimes junk humour and fine food) – I owe many thanks for making my M.A. experience such a warm and memorable one. Your friendship kept me going. Especial thanks must go to Suhaili, Meifeng, Brendon, and Siang who helped me immensely and saw me through the harder moments. -

Fleas, Faith and Politics: Anatomy of an Indian Epidemic, 1890-1925
FLEAS, FAITH AND POLITICS: ANATOMY OF AN INDIAN EPIDEMIC, 1890-1925. NATASHA SARKAR (M.A.), Bombay University A THESIS SUBMITTED FOR THE DEGREE OF DOCTOR OF PHILOSOPHY DEPARTMENT OF HISTORY NATIONAL UNIVERSITY OF SINGAPORE 2011 ACKNOWLEDGEMENTS It is a pleasure to thank those who have made this thesis possible. First, I would like to thank my supervisor Prof.Gregory Clancey for his contribution in time, ideas and support in making this journey productive and stimulating. Through his personal conduct, I have learned so much about what makes for a brilliant teacher. His invaluable suggestions helped develop my understanding of how one should approach research and academic writing. I appreciate his patience in granting me much latitude in working in my own way. It has indeed been an honour to be his PhD student. In fact, I could not have wished for a better PhD team. Prof.John DiMoia‘s enthusiasm and joy for teaching and research has been motivational. I thank him for his prompt and very useful feedback despite his incredibly busy schedule. Prof.Medha Kudaisya, in being compassionate, has been instrumental in easing the many anxieties that plague the mind while undertaking research. I thank her for her unstinting encouragement. Time spent at NUS was made enjoyable, in great measure, to the many friends who became an integral part of my life; providing a fun environment in which to learn and grow. I am grateful for time spent at the tennis courts, table-tennis hall and endless conversation over food and drinks. I would like to especially thank Shreya, Hussain and Bingbing, for their warmth, support and strength.