The Significance of Core Temperature – Pathophysiology and Measurement Methods the SIGNIFICANCE of CORE TEMPERATURE | TABLE of CONTENTS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How the Skin Thickness and Thermal Contact Resistance Influence
micromachines Article How the Skin Thickness and Thermal Contact Resistance Influence Thermal Tactile Perception Congyan Chen * and Shichen Ding School of Automation, Southeast University, Nanjing 210096, China; [email protected] * Correspondence: [email protected]; Tel.: +86-138-1588-0379 Received: 25 December 2018; Accepted: 24 January 2019; Published: 25 January 2019 Abstract: A few experimental studies on thermal tactile perception have shown the influence of the thermal contact resistance which relates to contact surface roughness and pressure. In this paper, the theoretical influence of the skin thickness and the thermal contact resistance is studied on the thermal model describing the temperature evolution in skin and materials when they come in contact. The thermal theoretical profile for reproducing a thermal cue for given contact thermal resistance is also presented. Compared to existing models of thermal simulation, the method proposed here has the advantage that the parameters of skin structure and thermal contact resistance in target temperature profiles can be adjusted in thermal perception simulation according to different skin features or surface roughness if necessary. The experimental results of surface roughness recognition were also presented. Keywords: thermal tactile perception; surface roughness; skin thickness; thermal perception reproduction 1. Introduction Thermal perception is a rich, emotive, and entirely silent information source. For example, when our hands touch objects, thermal perceptions can provide information about their thermal characteristics, and help us recognize materials [1]. More, it could be used as an alternative mobile feedback channel when required, as it is silent for quiet environments, especially in electromagnetic interference case where monitors or headsets cannot work normally. -

Support and Movement
UNIT Support and II Movement The Integumentary System 6 Bone Tissues and the Skeletal System 7 Articulations 8 9 The Muscular System © Mopic/Shutterstock 9781284057874_CH06_105_127.indd 105 23/12/14 4:07 PM 9781284057874_CH06_105_127.indd 106 23/12/14 4:07 PM CHAPTER © drxy/iStockphoto.com 6 OUTLINE Integumentary System ■ Overview ■ Skin Epidermis OBJECTIVES Dermis ■ Accessory Structures After studying this chapter, readers should be able to Nails 1. Explain the structure of the dermis and epidermis. Hairs 2. Describe the normal and pathological colors skin can have. 3. List the functions of the skin. Glands in the Skin 4. Describe the structure of nails. ■ Functions of the 5. Discuss the various kinds of glands in the skin and the secretions of each. Integumentary System 6. Explain how the sweat glands play a major role in regulating body temperature. ■ Response of the Integument 7. Describe the three most common forms of skin cancer. to Injuries and Wounds 8. Describe the location and function of sebaceous and ceruminous glands. 9. Explain the anatomic parts of a hair. ■ Effects of Aging on the 10. Describe the effects of aging on the integumentary system. Integumentary System ■ Skin Cancer ■ Burns ■ Summary ■ Key Terms ■ Learning Goals ■ Critical Thinking Questions ■ Review Questions ■ Essay Questions 107 9781284057874_CH06_105_127.indd 107 23/12/14 4:07 PM depending on which part of the body it covers. The two main Overview layers of skin are the epidermis and dermis. The epidermis, The integumentary system, which consists of the skin the outer layer, is made up of keratinized stratified squa- (cutaneous membrane) and accessory structures, accounts mous epithelium (FIGURE 6-1). -

Thermal Imaging & Body Temperature
Thermal Imaging & Body Temperature Thermal Imaging is the process to create an image using Infrared Radiation. Most things emit some form of Infrared Radiation, including humans and animals. Infrared Radiation is directly affected by temperature, e.g. the higher Thermal the temperature the more Infrared Radiation is Imaging emitted, and the inverse is also true. Explained Using a Microbolometer, a thermal camera is capable of generating a Thermal Image by applying a colour palette to the different intensities of Infrared Radiation. Body Temperature refers to the temperature of the body’s core where your internal organs and bodily systems function at an optimal level. Body Temperature tends to maintain a constant temperature and is not as easily affected by variables from the environment such as Body temperature, relative humidity, wind velocity, Temperature and radiation. Explained Normal Body Temperature tends to be 36.5– 37.5 °C (97.7–99.5 °F). Skin temperature refers to the temperature of the body skin which is the largest organ in the human body. Skin Temperature can vary between 33.5 and 36.9 C (92.3 and 98.4F) Skin Temperature tends to be affected by environmental factors more easily than body temperature as it is the Skin outermost area of the body. Temperature When reading skin temperature it is important to take in Explained environmental variables such as temperature, relative humidity, wind velocity, and radiation. In outdoor environments it is important to consider solar loading, as this also has an impact on temperature readings. Skin Offset (Correction) The software settings used to estimate this difference is called skin offset. -

TIDA-00824 Human Skin Temperature Sensing for Wearable Applications Reference Design
TIDA-00824 Human Skin Temperature Sensing for Wearable Applications Reference Design Abstract This TI Design report will show how to use the LMT70 temperature sensor to measure human skin temperature in a wearable device such as a smart watch or a fitness tracker (not as a diagnostic or therapeutic use). The wearable design covers both electrical and mechanical design to optimize performance of the LMT70 sensor’s ability to accurately measure skin temperature. Test data such as accuracy and thermal response is also discussed in this document. Document History Version Date Author Notes 1.0 September 2015 Michael Wong First Release TIDA-00824 Contents 1. OBJECTIVE ......................................................................................................................................................... 3 2. WEARABLE DESIGN .......................................................................................................................................... 3 2.1. ELECTRICAL DESIGN ........................................................................................................................................ 3 2.1.1. SIGNAL PATH...................................................................................................................................................... 3 2.1.2. MAIN PCB ............................................................................................................................................................ 4 2.1.3. REMOTE PCB..................................................................................................................................................... -

Mod. 3 Vital Signs
Mod. 3 Vital Signs 1. What is most important to assess during secondary assessment? a. Airway b. Pulse c. Respiration d. Chief complaint 2. The first set of vital sign measurements obtained are often referred to as which of the following? a. Baseline vital signs b. Normal vital signs c. Standard vital signs d. None of the above 3. A patient with a pulse rate of 120 beats per minute is considered which of the following? a. Dyscardic b. Normocardic c. Tachycardic d. Bradycardic 4. Where do baseline vital signs fit into the sequence of patient assessment? a. Ongoing assessment b. At primary assessment c. At secondary assessment d. At the patient's side 5. In a conscious adult patient, which of the following pulses should be assessed initially? a. Brachial b. Radial c. Carotid d. Pedal 6. You are assessing a 55-year-old male complaining of chest pain and have determined that his radial pulse is barely palpable. You also determine that there were 20 pulsations over a span of 30 seconds. Based on this, how would you report this patient's pulse? a. Pulse 20, weak, and regular b. Pulse 20 and weak c. Pulse 40 and weak d. Pulse 40, weak, and irregular 7. Which of the following are the vital signs that need to be recorded? a. Pulse, respiration, skin color, skin temperature and condition b. Pulse, respiration, skin color, skin temperature and condition, pupils, blood pressure, and bowel sounds c. Pulse, respiration, skin color, skin temperature and condition, pupils, and blood pressure d. Pulse, respiration, skin color, skin temperature, pupils, and blood pressure 8. -

The Skin's Role in Human Thermoregulation and Comfort
Center for the Built Environment UC Berkeley Peer Reviewed Title: The skin's role in human thermoregulation and comfort Book Title: from Thermal and Moisture Transport in Fibrous Materials Author: Arens, Edward A, Center for the Built Environment, University of California, Berkeley Zhang, H., Center for the Built Environment, University of California, Berkeley Publication Date: 2006 Series: Indoor Environmental Quality (IEQ) Permalink: http://escholarship.org/uc/item/3f4599hx Additional Info: ORIGINAL CITATION: Arens, E. and H. Zhang 2006. The Skin's Role in Human Thermoregulation and Comfort. Thermal and Moisture Transport in Fibrous Materials, eds N. Pan and P. Gibson, Woodhead Publishing Ltd, pp 560-602. Copyright Information: All rights reserved unless otherwise indicated. Contact the author or original publisher for any necessary permissions. eScholarship is not the copyright owner for deposited works. Learn more at http://www.escholarship.org/help_copyright.html#reuse eScholarship provides open access, scholarly publishing services to the University of California and delivers a dynamic research platform to scholars worldwide. 16 The skin’s role in human thermoregulation and comfort E. ARENS and H. ZHANG, University of California, Berkeley, USA 16.1 Introduction This chapter is intended to explain those aspects of human thermal physiology, heat and moisture transfer from the skin surface, and human thermal comfort, that could be useful for designing clothing and other types of skin covering. Humans maintain their core temperatures within a small range, between 36 and 38°C. The skin is the major organ that controls heat and moisture flow to and from the surrounding environment. The human environment occurs naturally across very wide range of temperatures (100K) and water vapor pressures (4.7 kPa), and in addition to this, solar radiation may impose heat loads of as much as 0.8kW per square meter of exposed skin surface. -
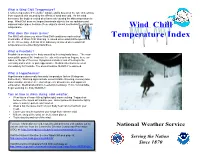
Wind Chill Temperature? It Is the Temperature It “Feels Like” Outside and Is Based on the Rate of Heat Loss from Exposed Skin Caused by the Effects of Wind and Cold
What is Wind Chill Temperature? It is the temperature it “feels like” outside and is based on the rate of heat loss from exposed skin caused by the effects of wind and cold. As the wind increases, the body is cooled at a faster rate causing the skin temperature to drop. Wind Chill does not impact inanimate objects like car radiators and exposed water pipes, because these objects cannot cool below the actual air temperature. Wind Chill What does this mean to me? The NWS will inform you when Wind Chill conditions reach critical Temperature Index thresholds. A Wind Chill Warning is issued when wind chill temperatures are life threatening. A Wind Chill Advisory is issued when wind chill temperatures are potentially hazardous. What is Frostbite? Frostbite is an injury to the body caused by freezing body tissue. The most susceptible parts of the body are the extremities such as fingers, toes, ear lobes, or the tip of the nose Symptoms include a loss of feeling in the extremity and a white or pale appearance. Medical attention is needed immediately for frostbite. The area should be SLOWLY re-warmed. What is Hypothermia? Hypothermia is abnormally low body temperature (below 95 degrees Fahrenheit). Warning signs include uncontrollable shivering, memory loss, disorientation, incoherence, slurred speech, drowsiness, and apparent exhaustion. Medical attention is needed immediately. If it is not available, begin warming the body SLOWLY. Tips on how to dress during cold weather. Wear layers of loose-fitting, lightweight, warm clothing. Trapped air between the layers will insulate you. Outer garments should be tightly woven, water repellent, and hooded. -

Impact of Hair Coat Differences on Rectal Temperature, Skin Temperature, and Respiration Rate of Holstein X Senepol Crosses in Florida
Senepol Symposium, St. Croix, USVI November 8-10, 2002 Impact of Hair Coat Differences on Rectal Temperature, Skin Temperature, and Respiration Rate of Holstein X Senepol Crosses in Florida T.A. Olson*,a, M. Avila-Chytil*, C.C. Chase, Jr.†, P.J. Hansen*, and S.W. Coleman†. *University of Florida, Gainesville, FL 32611; Agricultural Research Service, USDA, †Subtropical Agricultural Research Service, Brooksville, FL 34601 Summary The effect of hair type on rectal temperature, skin temperature, respiration rate, and feed intake under confinement in ¾ Holstein: ¼ Senepol crossbred cattle was studied during the summer of 2000 at two locations in Florida. The hair type was classified subjectively as 1) “slick”, very short, sleek and shiny and, 2) normal, similar to that of purebred Holstein cattle of the same age. The visual hair differences were quantified by collecting clipped hair samples. The hair samples were weighed, and slick animals averaged 11.47 mg/cm2 as opposed to 17.82 mg/cm2 for normal haired animals. Clipped hair weight was also lower (P < 0.05) in black as compared to white areas of the same spotted animals. The rectal temperatures of animals classified as slick was 0.34° C (P < 0.05) lower than that from normal-haired animals. The skin temperatures of slick animals was 0.49° C (P < 0.05) lower than that of normal haired animals while the respiration rate of slick animals was 12.4 (P < 0.05) breaths per minute less than that of animals with normal hair. The impact of hair type on feed intake was not significant, perhaps because the animals where not fed under a high level of heat stress. -

Skin Temperature in Young Women with Low Values of Adipose Tissue
Ann Appl Sport Sci 7(4): e780, 2019. http://www.aassjournal.com; e-ISSN: 2322–4479; p-ISSN: 2476–4981. 10.29252/aassjournal.780 ORIGINAL ARTICLE Skin Temperature in Young Women with Low Values of Adipose Tissue 1Vitaliy Viktorovich Epishev, 1Anna Valerievna Nenasheva*, 2Yulia Borisovna Korableva, 1Alexander Sergeevich Belenkov, 1Alina Azatovna Episheva, 3Seyed Morteza Tayebi 1Theory and Methods of Physical Education and Sport Department, the Institute of Sports, Tourism and Service, South Ural State University (National Research University), Chelyabinsk, Russia. 2Sports Science Research Centre, the Institute of Sports, Tourism and Service, South Ural State University (National Research University), Chelyabinsk, Russia. 3Core Research of Health Physiology and Physical Activity, Department of Exercise Physiology, Faculty of Sport Science, Allameh Tabataba'i University, Tehran, Iran. Submitted 19 June 2019; Accepted in final form 23 August 2019. ABSTRACT Background. Skin temperature is an important indicator of the functional status of the body. Infrared thermal images of the body surface or its separate parts could be the indicator of body composition and, probably, the criterion of the functional activity of muscles. Objectives. This study aims to find a correlation between the average values of skin temperature in different parts of the body and the components of body composition in young women with low values of adipose tissue (FAT % = 20.73±5.50; BMI = 20.23±2.44). Methods. The study involved 69 healthy women aged 18-20 (BMI = 20.23±2.44). Participants were subjected to a 15-minute temperature adaptation in the room with a temperature of 22–24°С and humidity of 45-50%. -
The Integumentary System the Integumentary System
Essentials of Anatomy & Physiology, 4th Edition Martini / Bartholomew The Integumentary System PowerPoint® Lecture Outlines prepared by Alan Magid, Duke University Slides 1 to 51 Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Integumentary System Components • Cutaneous membrane • Epidermis • Dermis • Accessory structures • Subcutaneous layer (hypodermis) Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Main Functions of the Integument • Protection • Temperature maintenance • Synthesis and storage of nutrients • Sensory reception • Excretion and secretion Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Components of the Integumentary System Figure 5-1 Integumentary Structure/Function The Epidermis • Stratified squamous epithelium • Several distinct cell layers • Thick skin—five layers • On palms and soles • Thin skin—four layers • On rest of body Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Cell Layers of The Epidermis • Stratum germinativum • Stratum spinosum • Stratum granulosum • Stratum lucidum (in thick skin) • Stratum corneum • Dying superficial layer • Keratin accumulation Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function The Structure of the Epidermis Figure 5-2 Integumentary Structure/Function Cell Layers of The Epidermis • Stratum germinativum -

Instructions for Use: Skin Temperature Sensor
StarboardMedical.com Instructions for Use Skin Temperature Sensor Thermistor: YSI 400 Series Equivalent Cat. No.: 400-SK DESCRIPTION: CONTRAINDICATIONS: Hyperthermia and hypothermia are frequently The Starboard Medical Skin Temperature sensor is experienced clinical conditions and their undesirable contraindicated for usage over traumatized and effects in patients have been well documented in the hypo-perfused areas. literature. Body temperature is measured continuously using disposable temperature sensors ADVERSE REACTIONS: or probes to detect hyper- or hypo- thermia. These The following adverse reactions have been reported sensors are inserted in the structure designed to fit a during clinical application of the skin temperature specific anatomy of the human body where sensors: temperature is measured. The main component of Skin irritations. the temperature sensors is a chip which changes Skin burns due to aberrant electro-cautery resistance with a change in temperature. The chip radio-frequency current pathways. used in the Skin Temperature Sensor is a thermistor equivalent to a YSI 400 series. This thermistor is DIRECTIONS FOR USE: encapsulated in a plastic cap connected to a lead 1. Dry skin in the area where the sensor is to be wire. This lead wire has an insert molded connector placed. on the opposite end, to connect with the instrument 2. Remove the paper backing, and place the cable. The accuracy of the sensor is: ±0.1˚C at 37˚C sensor in the dry skin area of axila, forehead and ±0.2˚C at 5˚C and 45˚C. or any other skin surface as clinically indicated. The Starboard Medical skin temperature sensor is 3. -

2 the Function and Structure of the Skin
978140514663_4_002.qxd 12/10/07 3:14 PM Page 10 2 The function and structure of the skin The skin – the interface between humans and their the dermis is loose connective tissue, the subcutis/ environment – is the largest organ in the body. It hypodermis, which usually contains abundant fat weighs an average of 4 kg and covers an area of (Fig. 2.1). 2m2. It acts as a barrier, protecting the body from harsh external conditions and preventing the loss Epidermis of important body constituents, especially water. A death from destruction of skin, as in a burn or in The epidermis consists of many layers of closely toxic epidermal necrolysis (p. 127), and the misery packed cells, the most superficial of which are of unpleasant acne, remind us of its many important flattened and filled with keratins; it is therefore functions, which range from the vital to the cosmetic a stratified squamous epithelium. It adheres to the (Table 2.1). dermis partly by the interlocking of its downward The skin has three layers. The outer one is the projections (epidermal ridges or pegs) with upward epidermis, which is firmly attached to, and supported projections of the dermis (dermal papillae) (Fig. 2.1). by connective tissue in the underlying dermis. Beneath The epidermis contains no blood vessels. It varies in thickness from less than 0.1 mm on the eyelids to nearly 1 mm on the palms and soles. As dead sur- Table 2.1 Functions of the skin. face squames are shed (accounting for some of the Function Structure/cell involved dust in our houses), the thickness is kept constant by cells dividing in the deepest (basal or germinative) Protection against: layer.