The Medical Letter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Full Text in Pdf Format
DISEASES OF AQUATIC ORGANISMS Published July 30 Dis Aquat Org Oral pharmacological treatments for parasitic diseases of rainbow trout Oncorhynchus mykiss. 11: Gyrodactylus sp. J. L. Tojo*, M. T. Santamarina Department of Microbiology and Parasitology, Laboratory of Parasitology, Faculty of Pharmacy, Universidad de Santiago de Compostela, E-15706 Santiago de Compostela, Spain ABSTRACT: A total of 24 drugs were evaluated as regards their efficacy for oral treatment of gyro- dactylosis in rainbow trout Oncorhj~nchusmykiss. In preliminary trials, all drugs were supplied to infected fish at 40 g per kg of feed for 10 d. Twenty-two of the drugs tested (aminosidine, amprolium, benznidazole, b~thionol,chloroquine, diethylcarbamazine, flubendazole, levamisole, mebendazole, n~etronidazole,mclosamide, nitroxynil, oxibendazole, parbendazole, piperazine, praziquantel, roni- dazole, secnidazole, tetramisole, thiophanate, toltrazuril and trichlorfon) were ineffective Triclabenda- zole and nitroscanate completely eliminated the infection. Triclabendazole was effective only at the screening dosage (40 g per kg of feed for 10 d), while nitroscanate was effective at dosages as low as 0.6 g per kg of feed for 1 d. KEY WORDS: Gyrodactylosis . Rainbow trout Treatment. Drugs INTRODUCTION to the hooks of the opisthohaptor or to ulceration as a result of feeding by the parasite. The latter is the most The monogenean genus Gyrodactylus is widespread, serious. though some individual species have a restricted distri- Transmission takes place largely as a result of direct bution. Gyrodactyloses affect numerous freshwater contact between live fishes, though other pathways species including salmonids, cyprinids and ornamen- (contact between a live fish and a dead fish, or with tal fishes, as well as marine fishes including gadids, free-living parasites present in the substrate, or with pleuronectids and gobiids. -

Expert Review 2
2021 Expert Committee on Selection and Use of Essential Medicines Application review I.1 Albendazole, mebendazole and praziquantel for the indication of treatment of (item number) taeniid cestode cysts Does the application adequately ☒ Yes address the issue of the public health ☐ need for the medicine? No ☐ Not applicable Comments: The larval stages of three taeniid cestode parasites, Echinococcus granulosus, Echinococcus multilocularis and Taenia solium, produce cysts in humans that are of medical relevance. The diseases caused by these parasitic cysts are called cystic echinococcosis (CE), alveolar echinococcosis (AE), and cysticercosis (being neurocysticercosis (NCC) the most common form) respectively, and they are recognised by WHO as neglected tropical diseases. NCC is mainly a disease of poverty that predominantly affects rural populations in Africa, Asia and Latin America. Access to diagnostic and treatment, to better manage epilepsy and other NCC is a challenge for the people affected in these communities due to the availability and costs of specialised diagnostic and care. Stigma and social discrimination also mean that many people try to “hide” the disease. Briefly summarize the role of the The only real options for treatment of CE are albendazole (ALB) and Mebendazole proposed medicine(s) relative to other (MEB). ALB is the drug of choice as it has better bioavailability. ALB is also preferred to therapeutic agents currently included in MEB, because MEB requires a higher dose and a higher pill burden, for example, an the Model List, or available in the adult patient would require 8 tablets/day of MEB compared with 2 tablets/day ALB. market. ALB and praziquantel ( PZQ) are the only drugs used for the antiparasitic treatment of NCC. -

Product List March 2019 - Page 1 of 53
Wessex has been sourcing and supplying active substances to medicine manufacturers since its incorporation in 1994. We supply from known, trusted partners working to full cGMP and with full regulatory support. Please contact us for details of the following products. Product CAS No. ( R)-2-Methyl-CBS-oxazaborolidine 112022-83-0 (-) (1R) Menthyl Chloroformate 14602-86-9 (+)-Sotalol Hydrochloride 959-24-0 (2R)-2-[(4-Ethyl-2, 3-dioxopiperazinyl) carbonylamino]-2-phenylacetic 63422-71-9 acid (2R)-2-[(4-Ethyl-2-3-dioxopiperazinyl) carbonylamino]-2-(4- 62893-24-7 hydroxyphenyl) acetic acid (r)-(+)-α-Lipoic Acid 1200-22-2 (S)-1-(2-Chloroacetyl) pyrrolidine-2-carbonitrile 207557-35-5 1,1'-Carbonyl diimidazole 530-62-1 1,3-Cyclohexanedione 504-02-9 1-[2-amino-1-(4-methoxyphenyl) ethyl] cyclohexanol acetate 839705-03-2 1-[2-Amino-1-(4-methoxyphenyl) ethyl] cyclohexanol Hydrochloride 130198-05-9 1-[Cyano-(4-methoxyphenyl) methyl] cyclohexanol 93413-76-4 1-Chloroethyl-4-nitrophenyl carbonate 101623-69-2 2-(2-Aminothiazol-4-yl) acetic acid Hydrochloride 66659-20-9 2-(4-Nitrophenyl)ethanamine Hydrochloride 29968-78-3 2,4 Dichlorobenzyl Alcohol (2,4 DCBA) 1777-82-8 2,6-Dichlorophenol 87-65-0 2.6 Diamino Pyridine 136-40-3 2-Aminoheptane Sulfate 6411-75-2 2-Ethylhexanoyl Chloride 760-67-8 2-Ethylhexyl Chloroformate 24468-13-1 2-Isopropyl-4-(N-methylaminomethyl) thiazole Hydrochloride 908591-25-3 4,4,4-Trifluoro-1-(4-methylphenyl)-1,3-butane dione 720-94-5 4,5,6,7-Tetrahydrothieno[3,2,c] pyridine Hydrochloride 28783-41-7 4-Chloro-N-methyl-piperidine 5570-77-4 -

Second and Third Generation Oral Fluoroquinolones
Therapeutic Class Overview Second and Third Generation Oral Fluoroquinolones Therapeutic Class • Overview/Summary: The second and third generation quinolones are approved to treat a variety of infections, including dermatologic, gastrointestinal, genitourinary, respiratory, as well as several miscellaneous infections.1-10 They are broad-spectrum agents that directly inhibit bacterial deoxyribonucleic acid (DNA) synthesis by blocking the actions of DNA gyrase and topoisomerase IV, which leads to bacterial cell death.11,12 The quinolones are most active against gram-negative bacilli and gram-negative cocci.12 Ciprofloxacin has the most potent activity against gram-negative bacteria. Norfloxacin, ciprofloxacin and ofloxacin have limited activity against streptococci and many anaerobes while levofloxacin and moxifloxacin have greater potency against gram-positive cocci, and moxifloxacin has enhanced activity against anaerobic bacteria.11-12 Gemifloxacin, levofloxacin and moxifloxacin are considered respiratory fluoroquinolones. They possess enhanced activity against Streptococcus pneumoniae while maintaining efficacy against Haemophilus influenzae, Moraxella catarrhalis and atypical pathogens. Resistance to the quinolones is increasing and cross-resistance among the various agents has been documented. Two mechanisms of bacterial resistance have been identified. These include mutations in chromosomal genes (DNA gyrase and/or topoisomerase IV) and altered drug permeability across the bacterial cell membranes.11-12 Clinical Guidelines support -
ALBENDAZOLE (Extrapolation to All Ruminants)
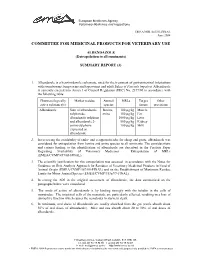
European Medicines Agency Veterinary Medicines and Inspections EMEA/MRL/865/03-FINAL June 2004 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE ALBENDAZOLE (Extrapolation to all ruminants) SUMMARY REPORT (3) 1. Albendazole is a benzimidazole carbamate, used for the treatment of gastrointestinal infestations with roundworms, lungworms and tapeworms and adult flukes of Fasciola hepatica. Albendazole is currently entered into Annex I of Council Regulation (EEC) No. 2377/90 in accordance with the following table: Pharmacologically Marker residue Animal MRLs Target Other active substance(s) species tissues provisions Albendazole Sum of albendazole Bovine, 100 µg/kg Muscle sulphoxide, ovine 100 µg/kg Fat albendazole sulphone 1000 µg/kg Liver and albendazole 2- 500 µg/kg Kidney amino sulphone 100 µg/kg Milk expressed as albendazole 2. In reviewing the availability of endo- and ectoparasiticides for sheep and goats, albendazole was considered for extrapolation from bovine and ovine species to all ruminants. The considerations and criteria leading to the identification of albendazole are described in the Position Paper Regarding Availability of Veterinary Medicines – Extrapolation of MRLs (EMEA/CVMP/457/03-FINAL). 3. The scientific justification for this extrapolation was assessed in accordance with the Notes for Guidance on Risk Analysis Approach for Residues of Veterinary Medicinal Products in Food of Animal Origin (EMEA/CVMP/187/00-FINAL) and on the Establishment of Maximum Residue Limits for Minor Animal Species (EMEA/CVMP/153a/97-FINAL). 4. In setting the ADI in the original assessment of albendazole, the data summarised on the paragraphs below were considered. 5. The mode of action of albendazole is by binding strongly with the tubulin in the cells of nematodes. -

Efficacy and Tolerability of Quinacrine Monotherapy and Albendazole Plus Chloroquine Combination Therapy in Nitroimidazole-Refractory Giardiasis: a Tropnet Study
Klinik für Infektiologie & Spitalhygiene Efficacy and tolerability of quinacrine monotherapy and albendazole plus chloroquine combination therapy in nitroimidazole-refractory giardiasis: a TropNet study Andreas Neumayr, Mirjam Schunk, Caroline Theunissen, Marjan Van Esbroeck, Matthieu Mechain, Manuel Jesús Soriano Pérez, Kristine Mørch, Peter Sothmann, Esther Künzli, Camilla Rothe, Emmanuel Bottieau Journal Club 01.03.21 Andreas Neumayr Background on giardia treatment: • 1st-line treatment: 5-nitroimidazoles: metronidazole (1957), tinidazole, ornidazole, secnidazole • cure rate of 5NIs in 1st-line treatment: ~90% • in the last decade, an increase of 5NI-refractory giardia cases has been observed in travel medicine clinics across Europe: Hospital for Tropical Diseases, London: 2008: 15% --> 2013: 40% 70% of 5NI-refractory cases imported from India • 2nd-line treatment: effectiveness of a 2nd round with a 5NI: ~17% alternative drugs: albendazole, mebendazole, nitazoxanide, quinacrine, furazolidone, chloroquine, paromomycin 2012 TropNet member survey: 53 centres use 39 different treatment regimens, consisting of 7 different drugs in mono- or combination-therapy in various dosages and durations JC 01.03.21 Nabarro LE et al. Clin Microbiol Infect. 2015;21:791-6. • by 2013, there were only 13 reports of 2nd-line therapy for giardiasis (8 case series, 5 individual case reports): n=110 Cure rates Albendazole 6/32 18.7% Paromomycin 5/17 29.4% Nitazoxanide 2/5 40.0% Albendazole + 5-NI 42/53 79.2% Quinacrine 19/21 90.5% Quinacrine + 5-NI 14/14 100% Quinacrine + Paromomycin 2/2 100% • 2013: TropNet "GiardiaREF" study kick-off: Study on efficacy and tolerability of two 2nd-line regimens in nitroimidazole-refractory giardiasis: Quinacrine JC 01.03.21 Meltzer E et al. -
Study Assessing Prices, Availability and Affordability of Children's
Study assessing prices, availability and affordability of children’s medicine in Chhattisgarh, India Part of the Better Medicine for Children project Authors Dr Antony KR Virendra Jain Puni Kokho Dr Kamlesh Jain The salient findings and views expressed in this report are solely those of the authors. Please direct correspondence to the authors: ([email protected], [email protected] [email protected], [email protected]). This publication does not necessarily represent the decisions or policies of the World Health Organization. ii Contents Acknowledgements ........................................................................................... v Abbreviations ................................................................................................... vi Executive summary ......................................................................................... vii Medicine availability .............................................................................................vii Medicine costs ................................................................................................... viii Affordability of standard treatment regimens ........................................................... ix Price components survey ...................................................................................... ix Conclusion .......................................................................................................... x 1. Introduction ................................................................................................. -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -

Valbazen ® (Albendazole)
® (albendazole oral suspension) Broad-Spectrum Dewormer Oral Suspension for Use in Cattle, Sheep, and Goats for removal and control of liver flukes, tapeworms, stomach worms (including 4th stage inhibited larvae of Ostertagia ostertagi), intestinal worms, and lungworms in cattle and sheep and for the treatment of adult liver flukes in nonlactating goats Active Ingredient Albendazole ............................. 11.36% (equivalent to 113.6 mg/mL) 1 L/33.8 fl oz (1 qt 1.8 fl oz) Approved by FDA under NADA # 110-048 40029175 ® (albendazole oral suspension) Broad-Spectrum Dewormer Oral Suspension for Use in Cattle, Sheep, and Goats for removal and control of liver Indications: flukes, tapeworms, stomach worms (including 4th stage inhibited larvae of Ostertagia Cattle and sheep: Valbazen is a broad-spectrum anthelmintic effective in the removal ostertagi), intestinal worms, and lungworms in cattle and sheep and for the treatment and control of liver flukes, tapeworms, stomach worms (including 4th stage inhibited of adult liver flukes in nonlactating goats larvae of Ostertagia ostertagi ), intestinal worms, and lungworms as indicated below. Active Ingredient: Goats: For the treatment of adult liver flukes in nonlactating goats. Albendazole .......................................................... 11.36% (Equivalent to 113.6 mg/mL) Parasite Cattle Sheep Goats Adult Liver Flukes Fasciola hepatica Fasciola hepatica, Fascioloides magna Fasciola hepatica Heads and Segments Moniezia benedeni, M. expansa Common Tapeworm (Moniezia expansa), Fringed Tapeworm of Tapeworms (Thysanosoma actinioides) Adult and 4th Stage Brown Stomach Worm, including 4th stage Brown Stomach Worm (Ostertagia circumcincta, Marshallagia Larvae of Stomach inhibited larvae (Ostertagia ostertagi), marshalli), Barber Pole Worm (Haemonchus contortus), Small Worms Barber Pole Worm (Haemonchus Stomach Worm (Trichostrongylus axei) contortus, H. -

Albendazole: a Review of Anthelmintic Efficacy and Safety in Humans
S113 Albendazole: a review of anthelmintic efficacy and safety in humans J.HORTON* Therapeutics (Tropical Medicine), SmithKline Beecham International, Brentford, Middlesex, United Kingdom TW8 9BD This comprehensive review briefly describes the history and pharmacology of albendazole as an anthelminthic drug and presents detailed summaries of the efficacy and safety of albendazole’s use as an anthelminthic in humans. Cure rates and % egg reduction rates are presented from studies published through March 1998 both for the recommended single dose of 400 mg for hookworm (separately for Necator americanus and Ancylostoma duodenale when possible), Ascaris lumbricoides, Trichuris trichiura, and Enterobius vermicularis and, in separate tables, for doses other than a single dose of 400 mg. Overall cure rates are also presented separately for studies involving only children 2–15 years. Similar tables are also provided for the recommended dose of 400 mg per day for 3 days in Strongyloides stercoralis, Taenia spp. and Hymenolepis nana infections and separately for other dose regimens. The remarkable safety record involving more than several hundred million patient exposures over a 20 year period is also documented, both with data on adverse experiences occurring in clinical trials and with those in the published literature and\or spontaneously reported to the company. The incidence of side effects reported in the published literature is very low, with only gastrointestinal side effects occurring with an overall frequency of just "1%. Albendazole’s unique broad-spectrum activity is exemplified in the overall cure rates calculated from studies employing the recommended doses for hookworm (78% in 68 studies: 92% for A. duodenale in 23 studies and 75% for N. -

Original Articles
MADIAJAGANE et al. : ANTIBIOTICS IN FEBRILE NEUTROPENIA 67 single course. However, some probable TPE cases did not REFERENCES show a fall in eosinophil counts after receiving the drug; a Udwadia FE. Tropical eosinophilia. In: Hertzog H (ed). Progress in respira- phenomenon reported by others. 18,19 These patients require tion research:Pulmonary eosinophilia. Volume 7. Basel:S. Kargar, 1975:35-155. a repeat course of diethylcarbamazine and the cause of their 2 Viswanathan R, Jaggi OP. Tropical eosinophilia. In: Ahuja MMS (ed). Progress in clinical medicine in India. First series. New Delhi:Arnold- eosinophilia is probably related to a parasite other than Heinemann Publishers, 1976:75-91. microfilaria. 3 Neva FA, Ottesen EA. Tropical (filarial) eosinophilia. N Engl J Med 1978; The prevalence of TPE in our community was high. Since 298:1129-31. 4 Spry CJF, Kumaraswami V. Tropical eosinophilia. Semin Hematol 1982; TPE is commonly caused by human lymphatic filarial infec- 19:107-15. tion, its prevalence is expected to be higher in endemic areas. 5 Ottesen EA, Neva FA, Paranjape RS, Tripathy SP, Thiruvengadam KV, However, only few susceptible individuals who had lymphatic Beaven MA. Specific allergic sensitisation to filarial antigens in tropical filarial infection had features ofTPE. The high prevalence of eosinophilia syndrome. Lancet 1979;1:1158-61. 6 World Health Organization. Fourth report of the Expert Committee on TPE that we observed was probably related to the high level Filariasis. Lymphatic filariasis. WHO Tech Rep Ser 1984;702:3--112. of filarial infection present in the community. Moreover, 7 Joshi VV, Udwadia FE, Gadgil RK. -

World Health Organization Model List of Essential Medicines, 21St List, 2019
World Health Organizatio n Model List of Essential Medicines 21st List 2019 World Health Organizatio n Model List of Essential Medicines 21st List 2019 WHO/MVP/EMP/IAU/2019.06 © World Health Organization 2019 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. World Health Organization Model List of Essential Medicines, 21st List, 2019. Geneva: World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.