Middlesex–London Paramedic Service
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Children's 76
CHILDREN'S 76 this Committee agree to make provision in revenue estimates for continuing, on a proportionate basis, the financial aid at present being afforded by Middlesex County Council to the extent shown hereunder to the Voluntary Organisations respectively named, viz.: — £ The Middlesex Association for the Blind ... ... 150 approx. The Southern Regional Association for the Blind ... 49 approx. Middlesex and Surrey League for the Hard of Hearing ... 150 approx. 27. Appointment of Deputy Welfare Officer: RESOLVED: That the Com mittee note the appointment by the Establishment Committee (Appointments Sub-Committee) on 16th November, 1964, of Mr. Henry James Vagg to this post (Scales A/B). (The meeting dosed at 9.10 p.m.) c Chairman. CHILDREN'S COMMITTEE: 30th December, 1964. Present: Councillors Mrs. Nott Cock (in the Chair), Cohen, G. Da vies, Mrs. Edwards, Mrs. Haslam, Mrs. Rees, Rouse, Tackley and B. C. A. Turner. PART I.—RECOMMENDATIONS.—NIL. PART n.—MINUTES. 10. Minutes: RESOLVED: That the minutes of the meeting of the Committee held on 30th September, 1964, having been circulated, be taken as read and signed as a correct record. 11. Appointment of Children's Officer: RESOLVED: That the Committee re ceive the report of the Town Clerk that the London Borough of Harrow Appointments Sub-Committee on 16th November, 1964, appointed Miss C. L. J. S. Boag, at present Area Children's Officer Middlesex County Coun cil, to the post of Children's Officer in the Department of the Medical Officer of Health with effect from 1st April, 1965, at a salary in accordance with lettered Grades C/D. -

London and Middlesex in the 1660S Introduction: the Early Modern
London and Middlesex in the 1660s Introduction: The early modern metropolis first comes into sharp visual focus in the middle of the seventeenth century, for a number of reasons. Most obviously this is the period when Wenceslas Hollar was depicting the capital and its inhabitants, with views of Covent Garden, the Royal Exchange, London women, his great panoramic view from Milbank to Greenwich, and his vignettes of palaces and country-houses in the environs. His oblique birds-eye map- view of Drury Lane and Covent Garden around 1660 offers an extraordinary level of detail of the streetscape and architectural texture of the area, from great mansions to modest cottages, while the map of the burnt city he issued shortly after the Fire of 1666 preserves a record of the medieval street-plan, dotted with churches and public buildings, as well as giving a glimpse of the unburned areas.1 Although the Fire destroyed most of the historic core of London, the need to rebuild the burnt city generated numerous surveys, plans, and written accounts of individual properties, and stimulated the production of a new and large-scale map of the city in 1676.2 Late-seventeenth-century maps of London included more of the spreading suburbs, east and west, while outer Middlesex was covered in rather less detail by county maps such as that of 1667, published by Richard Blome [Fig. 5]. In addition to the visual representations of mid-seventeenth-century London, a wider range of documentary sources for the city and its people becomes available to the historian. -

Middlesex. Ruislip
I DIRECTC'RY. J MIDDLESEX. RUISLIP. a43 eentral cylindrical shaft, with four smaller ones at the near the river Pin, and has a " Halt " on the Electric Motor angles, · · from a stone base : and in 1870 the chancel line from Harrow to Uxbridge. Here iS a Wesleyan chapel, 1ras under the direction of Mr. Ewan Christian, built in 1847. Eastcote House, formerly the- residence of and the rest of tho fabric by the late Sir G. G. Scott B.A.. : the Hawtreys and the property of Ralph Hawtrey Deane there are 500 sittings. The register of baptisms dates from esq. is now occupied by Charles Campbell McLeod esq. the year 1689; burials, 1695; marriage:s, 1699. The living is a vicarage, net yearly value £300, including 250 acrffi of King's End joins Ruislip. glebe, with residence, in the gift of the Dean and Canons RUISLIP COMMON is a hamlet, ll miles north--west, of Win.dsor, and held since 1900 by the Rev. William Arthur in the midst of an elevated district, with an extensive and Gordon Gray M.A. of Clare C-ollege, Cambridge, and rural beautiful prospect. Here is also a Methodist chapel. dean of Uxbridge. A new vicarage house, in the Eliza bethan style, was built in 1R81. Mrs. E. Rogers, in 1802, St. Catherine's End, or Little Manor, is 1 mile north-west ; left £380 to be invested in Consols, out of which £2 2s. was Duck's Hill, 2 miles north-west. to be paid to the vicar if he preached on Good Friday and Sexton, J oseph E. -

THE LONDON GAZETTE, 22 NOVEMBER, 1912. 8749 in Parliament.—Session 1913
THE LONDON GAZETTE, 22 NOVEMBER, 1912. 8749 In Parliament.—Session 1913. of Middlesex, commencing in the parish METROPOLITAN WATER BOARD of Laleham, in the rural district of (VARIOUS POWERS). Staines, by a junction with Conduit No. 22 authorized by the Metro- (Construction by Metropolitan Water Board politan Water Board (New Works) Act, of Waterworks, Wharf, Railways and otheV 1911, at a point on the southern side of the Works in the Counties of London, Middle- existing Staines Aqueduct of the Board, and sex, Kent and Surrey; Power to Deviate; within the fences of that aqueduct, 6£ Acquisition and Appropriation of Lands for chains or thereabouts, : measured in a Purposes of Intended Worksi and other Pur- westerly direction from the centre of the poses; Exemption from 92nd Section of River Ash where that river passes under the Lands Clauses Consolidation Act, 1845; said aqueduct near the house known as Extinction of Rights; Agreements for White House, and terminating in the parish Draining Lands and Prevention of Pollu- of Sunbury, in the urban district of Sun- tion; Diversion of Streams; Power to Retain bury-on-Thames, by a junction with an Lauds; Reservation of Rights on Sale of existing pipe of the Board at a point 1£ Lands; Provisions as to Compensation in chains or thereabouts measured in a Certain Cases; Revival of Powers for Con- southerly direction from the south-eastern structing Works and Acquisition of Lands corner of the southern valve-house at the Dis- in Middlesex authorized by New River Com- tribution Reservoir at the termination of the pany's Act, 1896; Extension of Time for said Staines Aqueduct, and | chain or there- Completion of Certain Works in Middlesex abouts measured in a north-easterly direc- and Essex, and Revival of Powers for Con- tion from the eastern bank of the brook structing other works in those Counties known as the Portlane brook. -

A«»«N, TOWN PLANNING and VALUATION
/a«»«n, TOWN PLANNING AND 18th December, 1944. VALUATION COMMITTEE Present : Councillor Priestley (in the Chair), Councillors Brown, C.C., committee. Beacham, Carter, Charles, J.P., Coles, Daniels, J.P., Ellement and Gange. PART I.—RECOMMENDATIONS. RECOMMENDATION I-Town and Country Planning Acts, 1932 : Proposed Formation of Executive Joint Town Planning Committees for Middlesex. Your Committee reported at length on this matter to the Council on 22nd July, 1944. The Council at that meeting (by Council resolution 2919) approved, in principle, the setting up of executive joint town planning committees in Middlesex in accordance with the suggestion which had been made by the Ministry of Town and Country Planning. The Ministry indicated that it would be appropriate to form three such joint committees in the County, one of these to be called the " West Middlesex Executive Joint Planning Committee" and to be appointed by the Borough Councils of Hendon, Wembley and Willesden and the Urban District Councils of Harrow, Ruislip-Northwood and Uxbridge. By the same resolution the Council authorised your Committee to appoint representatives to discuss generally, with representatives of the five other local authorities concerned, matters relating to the formation and constitution of the new West Middlesex executive joint committee, which was then being suggested by the Ministry of Town and Country Planning. The final paragraph of the recommendation adopted by the Council on 22nd July, 1944, contains an instruction to your Committee to report further, with appropriate recommendations, when a decision upon the proposals of the Ministry of Town and Country Planning had been arrived at. A conference was held in Harrow on 18th October, 1944, at which there were present representatives of the six local authorities mentioned above. -
Friern-Barnet-Library
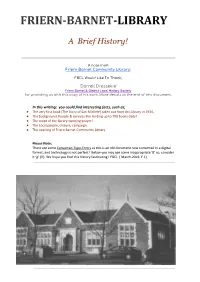
FRIERN-BARNET-LIBRARY A Brief History! A note from Friern Barnet Community Library; FBCL Would Like To Thank; ‘Dorrell Dressekie’ Friern Barnet & District Local History Society for providing us with this copy of his work. More details at the end of this document. In this writing; you could find interesting facts, such as; ● The very first book [The Story of San Michele] taken out from this library in 1934, ● The background, People & services like lending up to 700 books daily! ● The script of the library-opening-prayer! ● The Local people, closure, campaign ● The opening of Friern Barnet Community Library. Please Note; There are some Converted-Typo-Errors as this is an old document now converted in a digital format, and technology is not perfect! Below you may see some inappropriate ‘8’ so; consider it ‘g’ (!!). We hope you find this history fascinating! FBCL ( March.2019. F.I.) Frìern Barnet district Local History Society This history was compiled and written by Dorrell Dressekie in 2010 and updated in June 2012 Background Friem Barnet Library, housed in a Tudor style building in Friern Barnet Road, was opened in 1934 by the Middlesex County Council Library Service. A purpose•built a library, it was among the first to be built and filled out under the County Scheme for whole-time lending libraries. Other whole-time lending libraries of the period under the Scheme were Uxbridge (1930), Y iewsley (1931 ) and Hayts (1933). Before the opening of the label, Friem Banner Urban District Council had quite a different procedure for the lending of books. -

Gb0046 D-Ebz
GB 0046 D/EBz Hertfordshire Archives and Local Studies This catalogue was digitised by The National Archives as part of the National Register of Archives digitisation project NRA 38720 The National Archives HERTFORDSHIRE RECORD OFFICE D/EBz Deeds and other papers relating to Barnet and other parishes in Hertfordshire and Middlesex, 17th - 20th centuries, deposited between 1987 and 1992 by Messrs Boyes, Sutton and Perry. [Accessions 2292, 2414, 2693, 2711, 2733] Catalogue completed July 1993 EG HERTFORDSHIRE RECORD OFFICE D/EBz TITLE DEEDS Arkley D/EBz/T l 2 Jones Cottages 1863 1958 [Descent of title: James George Longham of Holborn, Middlesex, gent; William Temple of Sarratt, beer retailer; Henry Jones of Barnet, builder; Catherine Matilda Jones of Arkley, spinster; and Sidney John Bateman and his wife Florence [Original bundle] 14 items Barnet D/EBz/T2 Deed of Common Recovery concerning land in the 17 Dec 1825 manor of Chipping Barnet between Chadwick Marriott Walker Aytown of Edinburgh esq and his wife Eliza and Robert Longford of Gravesden, Kent, yeoman and his wife Jane D/EBz/T3 Abstract of the title of Messrs Morland and 1854 Wilkinson to freehold estates in Chipping Barnet and East Barnet D/EBz/T4 Unspecified land in High Barnet 1923 [Descent of title: William Hayes of Little Wittenham, Buckinghamshire, and Richard Raymond Weale of New Barnet] 2 items D/EBz/T5 32 Wood Street 1920 - 1966 [Descent of title: Henry Bennett of Hounslow, Middlesex, gent; Victor Alphonso Merchant of Barnet, general dealer; Annie Nellie Merchant of Barnet, wife of the above; Dorothy Bath of Barnet, married woman; Hubert Michael Cresswell Corfield of London, M.D ; and Marjorie Bateman of Barnet, widow] 11 items D/EBz/T6 5,6,7,8,9,10 Thornton Road - George Dickinson 1889 - 1918 Byfield of the City of London, gent to Samuel Dorman of North Finchley, Middlesex, estate agent; 8,9,10 Thornton Road - George Dickinson Byfield to William Marcos of Wandsworth, Surrey, gent; and 12,13,14 Thornton Road - William continued .. -

LONDON METROPOLITAN ARCHIVES SAINT MARY, SUNBURY on THAMES: CHURCH STREET, SURREY DRO/007 Page 1 Reference Description Dates
LONDON METROPOLITAN ARCHIVES Page 1 SAINT MARY, SUNBURY ON THAMES: CHURCH STREET, SURREY DRO/007 Reference Description Dates INCUMBENT Parish Registers DRO/007/A/01/001 Composite register: baptisms, marriages and 1565-1783 Not available for general access burials Please see microfilm Baptisms Dec 1565 - Dec 1783; Marriages May X001/100 1566 - Mar 1754; Burials Jan 1565/6 - Dec Please use microfilm 1654, Jul 1661 - Dec 1783 DRO/007/A/01/002 Register of births and christenings 1784-1807 Not available for general access Please see microfilm X001/100 Please use microfilm DRO/007/A/01/003 Register of births and christenings 1808-1812 Not available for general access Please see microfilm X001/100 Please use microfilm DRO/007/A/01/004 Register of baptisms 1813-1845 Not available for general access Please see microfilm X001/100 Please use microfilm DRO/007/A/01/005 Register of baptisms 1845-1880 Not available for general access Please see microfilm X001/100; X082/007 Please use microfilm DRO/007/A/01/006 Register of baptisms 1880-1893 Not available for general access Please see microfilm X082/007 Please use microfilm DRO/007/A/01/007 Register of baptisms 1893-1901 Not available for general access Please see microfilm X082/007 Please use microfilm LONDON METROPOLITAN ARCHIVES Page 2 SAINT MARY, SUNBURY ON THAMES: CHURCH STREET, SURREY DRO/007 Reference Description Dates DRO/007/A/01/008 Register of baptisms 1901-1913 Not available for general access Please see microfilm X082/007 Please use microfilm DRO/007/A/01/009 Register of baptisms 1913-1928 -

LONDON METROPOLITAN ARCHIVES STAINES RURAL and URBAN DISTRICTS ACC/1524 Page 1 Reference Description Dates Parishes ACC/1524/001
LONDON METROPOLITAN ARCHIVES Page 1 STAINES RURAL AND URBAN DISTRICTS ACC/1524 Reference Description Dates Parishes ACC/1524/001 Poor rate book. 1856-1857 ACC/1524/002/001 Tithe apportionment 1842-1843 Unfit Not available for general access ACC/1524/002/002 Tithe map. 1842-1843 Unfit Not available for general access ACC/1524/003 Enclosure award and plan. 1842 On temporary loan to depositor ACC/1524/004 Enclosure award and plan. Shepperton 1862 On temporary loan to depositor Common Lands. Title deed to Shepperton Recreation Ground and Shepperton Old Allotments ACC/1524/005 Printed copy of act for taking down and 1827 rebuilding parish church, for providing additional burial ground and for equalizing church rates With manuscript notes. ACC/1524/006 Terrier and valuation of parish of Staines, by H. 1828 Walter. Volume gives names of owner and occupier, number, description of property, old enclosure and common field acreage, annual value and total. Arranged alphabetically by name of owner. ACC/1524/007 Plan of public carriage road or highway 1843 together with public footways set out over open arable fields, meadows and pasture lands in parish of Staines. ACC/1524/008 Plan of public carriage roads or highways set 1843 out over open arable fields, meadows and pasture lands in parish of Staines. ACC/1524/009 Tithe apportionment with schedule. 1844 (No plan) LONDON METROPOLITAN ARCHIVES Page 2 STAINES RURAL AND URBAN DISTRICTS ACC/1524 Reference Description Dates ACC/1524/010 Altered apportionment of tithe rent charge with 1855 schedules and plan. Premises: land taken by Windsor, Staines and South Western Railway Company. -

RUISLIP, NORTHWOOD and EASTCOTE Local History Society Journal 2001
RUISLIP, NORTHWOOD AND EASTCOTE Local History Society Journal 2001 CONTENTS Re! Author Page Committee Members 2 Lecture Programme 2001-2002 2 Editorial 3 01/1 Catlins Lane, Eastcote (Part 2) Karen Spink 4 01/2 A Gainsborough Painting at Eastcote Lodge Eileen M Bowlt 10 01/3 The Grange at Well Green, Eastcote Eileen M Bowlt 15 01/4 A 'Pedigree' of the Arms of Hillingdon KayHolmes 19 01/5 The Arms of Middlesex KayHolmes 21 01/6 Munitions in Ruislip during the First World War Eileen M Bowlt 24 01/7 The Roads of Eastcote RonEdwards 27 Cover picture: The arms of the Ruislip-Northwood Urban District Council Designed and edited by Simon Morgan. Copyright © November 2001 individual authors and RNELHS. Membership of the Ruislip, Northwood and Eastcote Local History Society is open to all who are interested in local history. For further information please enquire at a meeting of the Society or contact the Membership Secretary. Meetings are held on the third Monday of each month from September to April and are open to visitors. (Advance booking is requiredfor the Christmas social.) An active Research Group supports those who are enquiring into or wishing to increase our understanding of the history of the ancient parish of Ruislip (the present Ruislip, Northwood and Eastcote). Its members are largely responsible for the papers in this Journal, and for other Society publications which are produced from time to time. RUISLIP, NORTHWOOD AND EASTCOTE Local History Society Registered Charity no. 288234 www.RNELHS.flyer.co.uk COMMITTEE 2001-2002 President -

Middlesex Campus Map County College
MIDDLESEX CAMPUS MAP COUNTY COLLEGE EXIT N ENTRANCE/EXIT . 667) LOT 11 MILL ROAD (RT DRIVE WH TECHNOLOGY LOT 1A LOT 10 MG COLLEG O T AC BH LOT 14 E L CB O W ED LOT 12 LOT 1 LOT 1B S WOODBRIDGE K 105 WEST I R O A D GREEN DRIV F 106 D R I V H O LOT 13 R H ES O IDEN 107 E PARKSIDE DRIVE CH F E LOT NH AL C 15 E. D R AVE. U R O A D BC MNI . 108 LOT 2 LOT 9 (RT ECOLOGICAL PARK JL EAST DRIV CHAMBERS DRIVE 109 . 514) R O U T E E EA IR LOT 8 110 CC B U S THE LOT LI EX 16 PA QUAD 111 C O GW L L ST E G E C1 EAST GREEN C2 D R RH I V E LOT 3 C3 LOT 7 COLLEGE DRIVE PE MH EAST E A S C4 TANK S1 T LH S2 ENTRANCE/EXIT BALL FIELDS BLDG 216 LOT 6 TENNI LOT 5 S CO URTS LOT 6A LOT 4 T EAS BUILDING KEY TO DRIVE AC ACADEMY FOR SCIENCE, THOMAS EDISON MATHEMATICS & PARK FM ENGINEERING TECHNOLOGIES LOT 6B BH BILLY JOHNSON HALL COLLEGE BC BLUE COLT BOOKSTORE C1 CENTER I C2 CENTER II FM FACILITIES MANAGEMENT PA PERFORMING ARTS CENTER C3 CENTER III GW GATEWAY – POLICE • INFORMATION PE PHYSICAL EDUCATION CENTER C4 CENTER IV IR INSTRUCTIONAL RESOURCE CENTER RH RARITAN HALL CH CHAMBERS HALL JL JOHNSON LEARNING CENTER S1 SOUTH I PARKING LOTS CB CRABIEL HALL LH L’HOMMEDIEU HALL S2 SOUTH II STUDENTS - 1, 1A, 2, 4, 6, 6A CC COLLEGE CENTER LI LIBRARY SR STAFF RESIDENCE (#106 - 110) FACULTY/STAFF - 1B, 5, 6B, 7, 8, 9, 10, 11, 16 EA EAST HALL MG MILL GATE ST STUDIO THEATER VISITORS - 3, 15 EX EAST HALL ANNEX MH MAIN HALL WH WEST HALL DISABLED - ALL LOTS ED EDISON HALL NH NORTH HALL 111 MCC FOUNDATION DAY CARE CENTER - 12 R9/22/11 Middlesex County College is a Smoke-Free Environment HOW TO GET TO MIDDLESEX COUNTY COLLEGE 1. -

How Middlesex County Was Settled with Farmers, Artisans, and Capitalists
Western University Scholarship@Western History eBook Collection eBook Collections 2010 How Middlesex County was Settled with Farmers, Artisans, and Capitalists: An Account of the Canada Land Company in Promoting Emigration from the British Isles in the 1830s through the 1850s Marvin L. Simner [email protected] Follow this and additional works at: https://ir.lib.uwo.ca/historybooks Part of the Canadian History Commons Recommended Citation Simner, Marvin L., "How Middlesex County was Settled with Farmers, Artisans, and Capitalists: An Account of the Canada Land Company in Promoting Emigration from the British Isles in the 1830s through the 1850s" (2010). History eBook Collection. 3. https://ir.lib.uwo.ca/historybooks/3 This Book is brought to you for free and open access by the eBook Collections at Scholarship@Western. It has been accepted for inclusion in History eBook Collection by an authorized administrator of Scholarship@Western. For more information, please contact [email protected], [email protected]. Cover: The wording on the cover, as well as the layout, is typical of that which appeared on books published in the early to mid-1800s. The purpose of the cover was to promote sales by emphasizing the most important features of the book as well as the book’s intended audience. How Middlesex County was Settled with Farmers, Artisans, and Capitalists: An Account of the Canada Land Company in Promoting Emigration from the British Isles in the 1830s through the 1850s ISBN 978-0-9812214-2-7 Copyright © Marvin L. Simner, 2010 All rights reserved. [email protected] Published by the London and Middlesex Heritage Museum 2609 Fanshawe Park Road East London, Ontario N5X 4A1 How Middlesex County was Settled with Farmers, Artisans, and Capitalists: An Account of the Canada Land Company in Promoting Emigration from the British Isles in the 1830s through the 1850s Marvin L.