Integrating Nutrition and Health in Palamu
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Accepted .Pdf
Accepted List of Accepted Application Form of Candidates for Interview for Class-IV Vacancies for Advertisement No. 01/15 dated 29.12.2015 Sl. Registration Name of Applicant Father's Name Qualificat Correspondence Address Date of Interview Time of Interview Post Sex Date of Birth Category No. No/ Roll No. applied for ion PUNAM KUMARI SHISHANKAR RAJAWAR HINU,C/5,PO-HINU,PS- 31-08-2016 08:00:00 AM DORANDA,DIST-RANCHI, 1 000002 PEON F 02/01/1990 SC MATRIC JHARKHAND,- 834002 KUNTI KUMARI KHAITA RAJAWAR HINU,C/59,PO-HINU,PS- 31-08-2016 08:00:00 AM DORANDA,DIST-RANCHI,JHARKHAND 2 000003 PEON F 02/10/1993 SC MATRIC PIN-834002 SANJAY KUMAR KINDO LATE BUDHRAM KINDO VILL-KATHAR GONDA,INDRAPURI 31-08-2016 08:00:00 AM ROAD NO-06,PO-HEHAL,DIST- 3 000004 PEON M 11/12/1976 ST BA RANCHI,JHARKHAND,PIN-834005 SANJAY KUMAR VERMA NAKUL MAHATO VILL-DHURGADGI,PO-TARA,PS- 31-08-2016 08:00:00 AM JAMUA,DIST- 4 000006 PEON M 03/01/1985 BC-2 BA GIRIDIH,JHARKHAND,PIN-815318 WAKIL FAJILAT HUSSAIN DORANDA BAILDAR 31-08-2016 08:00:00 AM MUHALLA,DORANDA,,PO- 5 000007 PEON M 05/06/1987 OBC MATRIC DORANDA,PS-DORANDA,RANCHI, JHARKHAND VIKASH KUMAR ARJUN SAW VILL-CHOTKI BARHI,PO-RASOIA 31-08-2016 08:00:00 AM DHAMNA,PS-BARHI,DIST- 6 000009 PEON M 20-10-1987 BC-1 MA HAZARIBAGH,JHARKHAND,PIN- 825405 KUMAR LAW KUSH RAMDHANI PRASAD BHATTIMUHALLA,DEVI MANDIR, 31-08-2016 08:00:00 AM DALTONGANJ,PALAMAU,JHARKHAND 7 000011 PEON M 01/06/1984 OBC MATRIC ,PIN-822101 AMRESH YADAV ALAKHDEV YADAV PO-KUNDA,PS-KUNDA,DIST- 31-08-2016 08:00:00 AM 8 000013 PEON M 09/03/1990 OBC-2 INTER CHATRA,JHARKHAND -

PMJAY Tagging List of Vles with PDS Dealer
Page 1 Ayushman Bharat (Golden Card Registration ) Dealer wise VLEs Tagging List Details Licence Sl. No. Dealer Name Mobile Address Block/Municipality GP VLE Name VLE Mobile No No. 1 1-87 JAGNARAYAN PAL 8757989781 VILL BAGHMANWA BISHRAMPUR Baghmanwa DAYA SHAMBHU RAM 8809940655 2 4-2006 KAJAL DEVI 9431147867 CHORATIA PO GARATIA BISRAMPUR BISHRAMPUR Baghmanwa DAYA SHAMBHU RAM 8809940655 3 4-93 GANGA SINGH 8002766140 VILL POST GHARTIYA BISHRAMPUR Bhagmanwa DAYA SHAMBHU RAM 8809940655 4 4-2007 JAGNARAYAN PARSAD 9939962415 VILL CHORATIA POST GHARTIYA BISHRAMPUR Bhagmanwa DAYA SHAMBHU RAM 8809940655 5 8-95 KRISHNA BAITHA 7677965242 VILL GAURA POST GHARTIYA BISHRAMPUR Bhagmanwa DAYA SHAMBHU RAM 8809940655 6 39-25 CHANDRA SHEKHAR PANDEY 8986853913 VILL POST BHANDAR PS BISHRAMPUR BISHRAMPUR Bhandar Raj Kumar 8839639358 7 5-2008 SANJAY KUMAR 9470973664 VILL TONA POST BHANDAR PS BISHRAMPUR BISHRAMPUR bhandar Raj Kumar 8839639358 8 1-1991 SHIV KUMAR PANDEY 8987470425 VILL POST BHANDAR PS BISHRAMPUR BISHRAMPUR Bhandar GUNJAN KUMAR 7544943720 9 01/17 PTG BISHRAMPUR BSO 9431578464 BISHRAMPUR BISHRAMPUR Bishrampur Anil Kumar Gupta 9572254008 10 2-2010 ASHAWAD S H G 8051102219 VILL GHASIDAG POST GHARTIYA BISHRAMPUR Ghashidag Papu kumar 7050237763 11 1-98 CHANDRADEV RAM 9608964654 VILL GHASIDAG POST GHARTIYA BISHRAMPUR Ghashidag Papu kumar 7050237763 12 6-88 DWARIKA SINGH 7631052258 VILL KOIDIYA POST GHARTIYA BISHRAMPUR Ghashidag Papu kumar 7050237763 13 01-2010 KALAP BRIKSH S H G 8969187824 VILL JAMARI POST GHARTIYA BISHRAMPUR Ghashidag Papu kumar 7050237763 -
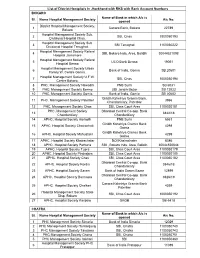
List of District Hostpitals in Jharkhand with RKS with Bank Account Numbers BOKARO Name of Bank in Which A/C Is Sl
List of District Hostpitals In Jharkhand with RKS with Bank Account Numbers BOKARO Name of Bank in which A/c is Sl. Name Hospital Management Society A/c No. opened District Hospital Management Society, 1 Canara Bank, Bokaro 22789 Bokaro Hospital Management Society Sub. 2 SBI, Chas 1000050193 Divisional Hospital Chas. Hospital Management Society Sub. 3 SBI Tenughat 1100050222 Divisional Hospital Tenughat. Hospital Management Society Referal 4 SBI, Bokaro Inds, Area, Balidih 30044521098 Hospital Jainamore Hospital Management Society Referal 5 UCO Bank Bermo 19051 Hospital Bermo Hospital Management Society Urban 6 Bank of India, Gomia SB 20601 Family W. Centre Gomia. Hospital Management Society U.F.W. 7 SBI, Chas 1000050194 Centre Bokaro. 8 PHC. Management Society Nawadih PNB Surhi SB 6531 9 PHC. Management Society Bermo UBI Jaridih Bazar SB 12022 10 PHC. Management Society Gomia Bank of India, Gomia SB 20602 Giridih Kshetriya Gramin Bank, 11 PHC. Management Society Paterber 3966 Chandankiary, Paterbar 12 PHC. Management Society Chas SBI, Chas Court Area 1100020181 PHC. Management Society Dhanbad Central Co-opp. Bank 13 3844/18 Chandankiary Chandankiary 14 APHC. Hospital Society Harladih PNB Surhi 6551 Giridih Kshetriya Gramin Bank 15 APHC. Hospital Society Chatrochati 4298 Goima Giridih Kshetriya Gramin Bank 16 APHC. Hospital Society Mahuatanr 4299 Goima 17 APHC. Hospital Society Khairachatar BOI Khairachater 8386 18 APHC. Hospital Society Pathuria SBI , Bokaro Inds. Area, Balidih 30044520844 19 APHC. Hospital Society Tupra SBI, Chas Court Area 1100050179 20 APHC. Hospital Society Pindrajora SBI, Chas Court Area 1100050180 21 APHC. Hospital Society Chas SBI, Chas Court Area 1100050182 Dhanbad Central Co-opp. -
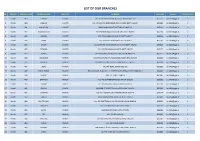
List of Our Branches
LIST OF OUR BRANCHES SR REGION BRANCH CODE BRANCH NAME DISTRICT ADDRESS PIN CODE E-MAIL CONTACT NO 1 Ranchi 419 DORMA KHUNTI VILL+PO-DORMA,VIA-KHUNTI,DISTT-KHUNTI-835 227 835227 [email protected] 0 2 Ranchi 420 JAMHAR KHUNTI VILL-JAMHAR,PO-GOBINDPUR RD,VIA-KARRA DISTT-KHUNTI. 835209 [email protected] 0 3 Ranchi 421 KHUNTI (R) KHUNTI MAIN ROAD,KHUNTI,DISTT-KHUNTI-835 210 835210 [email protected] 0 4 Ranchi 422 MARANGHADA KHUNTI VILL+PO-MARANGHADA,VIA-KHUNTI,DISTT-KHUNTI 835210 [email protected] 0 5 Ranchi 423 MURHU KHUNTI VILL+PO-MURHU,VIA-KHUNTI, DISTT-KHUNTI 835216 [email protected] 0 6 Ranchi 424 SAIKO KHUNTI VILL+PO-SAIKO,VIA-KHUNTI,DISTT-KHUNTI 835210 [email protected] 0 7 Ranchi 425 SINDRI KHUNTI VILL-SINDRI,PO-KOCHASINDRI,VIA-TAMAR,DISTT-KHUNTI 835225 [email protected] 0 8 Ranchi 426 TAPKARA KHUNTI VILL+PO-TAPKARA,VIA-KHUNTI, DISTT-KHUNTI 835227 [email protected] 0 9 Ranchi 427 TORPA KHUNTI VILL+PO-TORPA,VIA-KHUNTI, DISTT-KHUNTI-835 227 835227 [email protected] 0 10 Ranchi 444 BALALONG RANCHI VILL+PO-DAHUTOLI PO-BALALONG,VIA-DHURWA RANCHI 834004 [email protected] 0 11 Ranchi 445 BARIATU RANCHI HOUSING COLONY, BARIATU, RANCHI P.O. - R.M.C.H., 834009 [email protected] 0 12 Ranchi 446 BERO RANCHI VILL+PO-BERO, RANCHI-825 202 825202 [email protected] 0 13 Ranchi 447 BIRSA CHOWK RANCHI HAWAI NAGAR, ROAD NO. - 1, KHUNTI ROAD, BIRSA CHOWK, RANCHI - 3 834003 [email protected] 0 14 Ranchi 448 BOREYA RANCHI BOREYA, KANKE, RANCHI 834006 [email protected] 0 15 Ranchi 449 BRAMBEY RANCHI VILL+PO-BRAMBEY(MANDER),RANCHI-835205 835205 [email protected] 0 16 Ranchi 450 BUNDU -

MANISH Final
DISTRICT SUPERINTENDENT OF EDUCATION, PALAMU foHkkxh; ladYi la[;k 1145 fnukad 18-07-2019 ds vkyksd esa vizf'kf{kr f'k{kdksa dks mudh fu;qfDr frfFk ls ,oa yksd lsok vk;ksx }kjk fu;qDr f'k{kdksa dk e/s kk lwph ls xzsM&1 dh vkilh ojh;rk lwphA Social Sl# Name School Block Gender DOB DOJ in Service Grade 1 Designation Sl.No. In Merit List Address Remarks Category MOHAMMAD MADRASATUL ISLAM KUDAGA Unreserv 1 CHAINPUR (200210) Male 12/05/1962 25/09/1980 25/09/1980 INTER TRAINED PATRATU,SARJU,GARU, LATEHAR JAMALUDIN KALAN ed NEZMUDDIN AHAMAD MADRASATUL ISLAM KUDAGA Unreserv 2 CHAINPUR (200210) Male 03/02/1962 01/10/1980 01/10/1980 INTER TRAINED SHAHPUR, CHAINPUR, PALAMU ANSARI KALAN ed MADRASATUL ISLAM KUDAGA Unreserv 3 MD FASIHUDDIN CHAINPUR (200210) Male 04/04/1964 01/06/1982 01/06/1982 INTER TRAINED SHAHPUR, CHAINPUR, PALAMU KALAN ed PRAMOD KUMAR BISHRAMPUR Unreserv 4 UPG RAJKIYEKRIT MS TONA Male 01/01/1963 21/08/1982 21/08/1982 INTER TRAINED DUBEY (200209) ed Unreserv 5 AMAR NATH JHA KALI SANSKRIT MS KISHUNPUR PATAN (200212) Male 05/06/1964 29/08/1982 29/08/1982 INTER TRAINED ed DALTONGANJ Unreserv 6 AHMAD HUSSAIN MADARSA AHSANUL ULOOM Male 23/04/1964 01/04/1983 01/04/1983 INTER TRAINED kund mohallah near millat masjid (200201) ed MD REYAZUDDIN MADRASATUL ISLAM KUDAGA Unreserv 7 CHAINPUR (200210) Male 12/11/1963 02/01/1984 02/01/1984 INTER TRAINED SUNTHA, PANDEYPURA, PATAN, PALAMU ANSARI KALAN ed UPG RAJKIYEKRIT MS MANJHI Unreserv VILL- MAJHIGAWAN, P. -

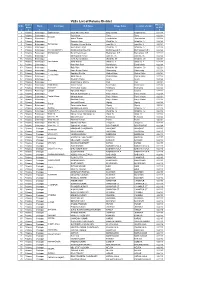
PALAMAU Name of the Lead Bank: STATE BANK of INDIA
List of villages with population below 2000 alloted to banks for FI Name of the District :: PALAMAU Name of the Lead Bank: STATE BANK OF INDIA Population of the village as Sl. Name of village with population Name of Bank , allotted per (2001 no Name of Block Name of Panchayat below 2000 the village census) 1 2 7 5 1 HARIHARGANJ KULHIYA KULHIYA VGB DHAB 920 HARIHARGANJ KULHIYA SHIKAR PUR VGB DHAB 558 HARIHARGANJ KULHIYA KARI LEBDA VGB DHAB 40 HARIHARGANJ KULHIYA LADI BADI VGB DHAB 592 HARIHARGANJ KULHIYA KOTHILA VGB DHAB 735 HARIHARGANJ KULHIYA NAUDIHA KALA VGB DHAB 126 HARIHARGANJ KULHIYA JAGDISHPUR VGB DHAB 635 HARIHARGANJ KULHIYA DIGLA VGB DHAB 9 HARIHARGANJ KULHIYA KOLHUWADA VGB DHAB 585 HARIHARGANJ KULHIYA JAHANA VGB DHAB 354 HARIHARGANJ KULHIYA NATHA VGB DHAB 50 HARIHARGANJ KULHIYA HARNIYA KHURD VGB DHAB 4 HARIHARGANJ SEMERWAR SEMERWAR VGB DHAB 1515 HARIHARGANJ SEMERWAR BHANDAR VGB DHAB 21 HARIHARGANJ SEMERWAR BIJWAR VGB DHAB 314 HARIHARGANJ SEMERWAR RAJWAR VGB DHAB 153 HARIHARGANJ SEMERWAR THARGHAT VGB DHAB 9 HARIHARGANJ SEMERWAR DHABKALA VGB DHAB 1398 HARIHARGANJ SEMERWAR DHABA KHURD VGB DHAB 168 HARIHARGANJ SEMERWAR MAMERKHA VGB DHAB 195 HARIHARGANJ SEMERWAR KAUWAKHOH VGB DHAB 478 HARIHARGANJ SEMERWAR PIRAUJEE VGB DHAB 448 HARIHARGANJ SEMERWAR TARACHAK VGB DHAB 110 HARIHARGANJ SEMERWAR CHANDA VGB DHAB 151 HARIHARGANJ SEMERWAR BIJNIWAR URF LAKHNI VGB DHAB 526 HARIHARGANJ KATAIYA KUSHDIH VGB DHAB 546 HARIHARGANJ KATAIYA TENUWA KALA VGB HARIHARGANJ 819 HARIHARGANJ KATAIYA JAGDISHPUR/ RAMPUR VGB HARIHARGANJ 389 HARIHARGANJ KATAIYA -

Schools for Class-VIII in All Districts of Jharkhand State School CODE UDISE NAME of SCHOOL
Schools for Class-VIII in All Districts of Jharkhand State School CODE UDISE NAME OF SCHOOL District: RANCHI 80100510 20140117617 A G CHURCH HIGH SCHOOL RANCHI 80100376 20140105605 A G CHURCH MIDDLE SCHOOL KANKE HUSIR 80100383 20140106203 A G CHURCH SCHOOL FURHURA TOLI 80100806 20140903803 A G CHURCH SCHOOL 80100917 20140207821 A P E G RESIDENTIAL SCHOOL RATU 80100808 20140904002 A Q ANSARI URDU MIDDLE SCHOOL IRBA 80100523 20140119912 A S PUBLIC SCHOOL 80100524 20140120009 A S T V S ZILA SCHOOL 80100411 20140109003 A V K S H S 80100299 20140306614 AADARSH GRAMIN PUBLIC SCHOOL TANGAR 80100824 20140906303 ADARSH BHARTI PUBLIC HIGH SCHOOL MANDRO 80100578 20142401811 ADARSH H S MCCLUSKIEGANJ 80100570 20142400503 ADARSH HIGH SCHOOL SANTI NAGAR KHALARI 80100682 20142203709 ADARSH HIGH SCHOOL KOLAMBI TUSMU 80100956 20141108209 ADARSH UCHCHA VIDYALAYA MURI 80100504 20140116916 ADARSHA VIDYA MANDIR 80100846 20140913601 ADARSHHIGH SCHOOL PANCHA 80100214 20140603012 ADIVASI BAL VIKAS VIDYALAYA JINJO THAKUR GAON 80100911 20140207814 ADIVASI BAL VIKAS VIDYALAYA RATU 80100894 20140202702 ADIVASI BAL VIKAS VIDYALAYA TIGRA GURU RATU 80100119 20140704204 ADIVASI BAL VIKAS VIDYALAYA TUTLO NARKOPI 80100647 20140404507 ADIWASI VIKAS HIGH SCHOOL BAJRA 80101106 20140113028 AFAQUE ACADEMY 80100352 20140100813 AHMAD ALI MORDEN HIGH SCHOOL 80100558 20140123620 AL-HERA PUBLIC SCHOOL 80100685 20142203716 AL-KAMAL PLAY HIGH SCHOOL 80100332 20142303514 ALKAUSAR GIRLS HIGH SCHOOL ITKI RANCHI 80100741 20140803807 AMAR JYOTI MIDDLE CUM HIGH SCHOOL HARDAG 80100651 20140404516 -
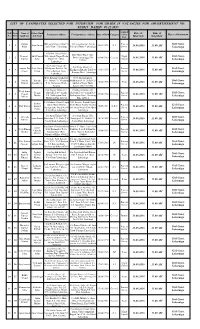
List of Candidates Selected for Interview .Pdf
LIST OF CANDIDATES SELECTED FOR INTERVIEW FOR GRADE IV VACANCIES FOR ADVERTISEMENT NO. 01/2015 DATED 05.11.2015 Applied Roll Form Name of Father/Husb Date of Time of Permanent Address Correspondence Address Date of Birth Category for the No. Sl.No Applicant and Name Place of Interview Post Interview Interview Indrani D/O jatru Oraon vill& P.S Vill juria Kathar Toli & Process Civil Court, 1 1 Jatru Oraon 30/03/1976 S.T 16.08.2016 11.00 AM Kujur juria Distt.- Lohardaga P.S juria Distt.- Lohardaga Server Lohardaga S/O Shiv Prasad Sahu Shiv Hotel Block More Pramod Shiv Prasad Vill- Shanti Nagar Kisko Night Civil Court, 2 2 Distt- Lohardaga PIN 05/06/1985 General 16.08.2016 11.00 AM Kumar Sahu More P.O + Distt- Guard 835302 Lohardaga Lohardaga S/o Nania Oraon vill- S/o Nania Oraon vill- Laxman Deo Late Nania Khakpatra Kumba Toli Process Civil Court, 3 3 Khakpatra Kumba Toli P.O 12/01/1976 S.T 16.08.2016 11.00 AM Oraon Oraon P.O – Rampur Distt- Server – Rampur Distt- Lohardaga Lohardaga Lohardaga D/O- Balram Upadhayay New Shashtri nagar Antima Balram Vill- Odnar P.S- Chainpur Madhukam,P.O- Hehal P.S- Civil Court, 4 4 12/06/1988 General Peon 16.08.2016 11.00 AM Tiwary Upadhayay P.O- Harinamar Distt- Sukhdeo Nagar Distt- Lohardaga Palamu Ranchi PIN – 834005 S/O Degan Mahto vill- S/O Degan Mahto vill- Bhadeshwar Degan Shivadih P.O – Sandh Shivadih P.O – Sandh P.S- Process Civil Court, 5 5 Prasad 09/06/1990 General Mahto P.S- Badkagaon Distt- Badkagaon Distt- Hazarbag Server 16.08.2016 11.00 AM Mehta Lohardaga Hazarbag Pin- 825311 Pin- 825311 S/O -
S.No. District Code Name of the Establishment Address Major
Jharkhand S.No. District Name of the Address Major Activity Broad NIC Owners Employ Code Establishment Description Activity hip ment Code Code Class Interval 1 01 Madhya vidhalya sisari 822114 Education 20 851 1 15-19 BOKARO STEEL 2 BHAVNATHPUR Mining 05 051 4 25-29 MINES TOWNSHEEP BHAVNATHPUR TOWNSHEEP 822112 201 VATIKA HOTEL 9 GURUDAWARA Resturant 14 561 2 15-19 GALI GURUDAWARA GALI 815301 304 SAWAN BEAR BAR 19 GANDHI CHOWK Resturant 14 563 2 10-14 GANDHI CHOWK 404 815301 MAHATO HOTEL 103 AURA AURA Hotel 14 562 2 10-14 504 825322 6 04 HOTEL KALPANA 19 ISRI ISRI 825107 Resturant 14 561 2 15-19 7 04 HOTEL KAVERI 64 ISRI ISRI 825107 Resturant 14 561 2 10-14 HARIDEVI REFRAL 89 THAKURGANGTI Health 21 861 1 10-14 806HOSPITAL 813208 RAJMAHAL 105 814154 Health 21 861 4 30-99 PARIYOJNA 906HOSPITAL SAMUDAYIK HEALTH PATHERGAMA 814147 Health 21 861 1 30-99 10 06 CENTER SAMUDYIK HEALTH 129 SUNDERPAHARI Health 21 861 1 15-19 CENTER 814133 11 06 rajkiya madh vidyalaya 835302 Education 20 851 1 15-19 12 11 jeema ICICI BANK 160 RAMGARH Banking 16 641 2 10-14 13 16 829118 PRATHMIK BLOCK MOD Health 21 861 1 15-19 SWASTHYA KENDRA PATRATU 829118 14 16 CCL HOSPITAL 82 RAMGARH 829106 Health 21 871 1 30-99 15 16 BHURKUNDA JINDAL STEEL AND 4(1) PATRATU Manufature 06 243 4 >=500 16 16 POWER BALKUDRA 829118 KEDLA WASHRI BASANT PUR Mining 05 051 2 >=500 17 16 WASHRI 829101 PRERNA MAHILA 126(2) SANGH Retail 12 472 5 10-14 VIKASH MANDAL RAMNAGAR BARKA CHUMBA 18 16 RAMNAGAR 829101 BIRU TASHA PARTY 89(2) BARKA Exitment 19 772 2 15-19 CHUMBA BRAHMAN 19 16 MUHALLA 829101 -

Annual Report
ANNUAL REPORT 2014 - 15 Jharkhand Jan Kalyan Vikas Sansthan Muslim Nagar, Daltonganj , Palamu (jharkhand) Web-www.jjkvs.org E-mail – [email protected] JJKVS ANNUAL REPORT 2014-15 From the Secretary Desk Socio economic grassroots changes and sustainable transformation need strategic planning, continuous efforts and intervention. Every year is a challenging year with new learning and experiences, but also offers new growth and impacts for the people involved with our projects and programs. The report presents the details of our strategy, intervention, activities, and impact at grass root level. We have continued our activities in this financial year with key issues of wasteland development, livelihood enhancement through agriculture promotion, environmental awareness, health and hygiene, AIDS awareness campaign, promotion of SRI,/SWI . The agriculture related activities has addressed waste land utilization, developing land resources, water resources for livelihood enhancement the activities have put thrust on preparation of agriculture calendar at every project village. The SRI and SWI promotion have been instrumental in mobilizing widespread community action in agriculture production at low cost and water use efficiency. Our efforts for integrated development of , marginalized farmers and women continued this year also through various activities like awareness generation on new technology in agriculture practice, SRI/SWI kitchen gardening, horticulture development, capacity building of farmers on water use efficiency, leadership -

ANSWERED ON:22.12.2004 POST OFFICES in JHARKHAND Manoj Kumar Shri
GOVERNMENT OF INDIA COMMUNICATIONS AND INFORMATION TECHNOLOGY LOK SABHA UNSTARRED QUESTION NO:3500 ANSWERED ON:22.12.2004 POST OFFICES IN JHARKHAND Manoj Kumar Shri Will the Minister of COMMUNICATIONS AND INFORMATION TECHNOLOGY be pleased to state: (a) the total number and names of places in various districts of Jharkhand where post offices are in operation; (b) the names of places in all the districts of Jharkhand particularly Palamu, Gadhva and Latehar districts where post offices are likely to be opened; and (c) the time by when Government proposes to open post offices at the proposed places? Answer THE MINISTER OF STATE IN THE MINISTRY OF COMMUNICATIONS AND INFORMATION TECHNOLOGY (DR. SHAKEEL AHMAD ) (a) District-wise details of post offices functioning in Jharkhand are given at Annexure. (b) At present no justified proposal is pending based on the distance, population and income norms for opening post offices in any district including Palamu, Gadhva and Latehar districts. (c) Does not arise in view of (b) above. Detail of Jharkhand Circle Postal Network HAZIRABAGH DISTRICT Sl. Name Name of Name of village in which No. of Tehsil/Taluka/ located where applicable Post Block in Office which located. 1. Bara Bazar Sadar H. Bagh Bara Bazar 2. Hazaribagh Sadar H. Bagh Hazaribagh 3. Boddom Bazar Sadar H. Bagh Boddom Bazar 4. B.S.F. Meru Sadar H. Bagh Meru 5. Jagarnath Dham Sadar H. Bagh Jagarnath Dham 6. College More Sadar H. Bagh College More 7 Babhanbey Sadar H. Bagh Babhandey 8. Lila Nagar Sadar H. Bagh Lila Nagar 9. Morangi Sadar H. -
Master Report 30 Column District Palamu (Total 657)
VLEs List of Palamu District District PIN Code Sl No. Block Panchayat VLE Name Village Name Location of CSCs Name of CSC 1 2 3 4 5 6 7 8 1 Palamu Bishrampur Baghmanwan Daya Shambhu Ram Baghmanwa Baghmanwa 822124 2 Palamu Bishrampur Raj Kumar Tona Tona 822124 Bhandar 3 Palamu Bishrampur Ashok Thakur Jharhakalan Jharhakalan 822124 4 Palamu Bishrampur Hasnain Alam Ward No. 17 Ward No. 17 822124 5 Palamu BishrampurBishrampur Chandan Kumar Mehta ward No. 8 ward No. 8 822124 6 Palamu Bishrampur Amiteshwar Dayal Ward No. 17 Ward No. 17 822124 7 Palamu Bishrampur Bishrampur(N.P.) Harshvardhan Bux Rai Bishrampur(N.P.) Bishrampur(N.P.) 822124 8 Palamu Bishrampur Bishsrampur Nurul Hoda Ansari Bishrampur N.P. Bishrampur N.P. 822124 9 Palamu Bishrampur Md Rajiullah Ansari ward no. 05 ward no. 05 822124 10 Palamu Bishrampur Vivek Kumar Shukla Ward No. 09 Ward No. 09 822124 11 Palamu BishrampurDandilakala Afzal Ahmad Ward no. 8 Ward no. 8 822124 12 Palamu Bishrampur Ram Nath Ram Dandilakala Dandilakala 822124 13 Palamu Bishrampur Raju Ram Ward No. 09 Ward No. 09 822124 14 Palamu Bishrampur Ghansidag Papu Kumar Yadav Ghansidag Ghansidag 822124 15 Palamu Bishrampur Kapildeo Shukla Gurha Kalan Gurha Kalan 822124 Gurha Kalan 16 Palamu Bishrampur Sunil Kumar Gurha Kalan Gurha Kalan 822124 17 Palamu Bishrampur Ravindra Yadav Seora Seora 822124 Guri 18 Palamu Bishrampur Akash Kumar Mishra Guri Guri 822124 19 Palamu Bishrampur Ketat Kalan Vishal Kumar Ketat Kalan Ketat Kalan 822124 20 Palamu Bishrampur Koshiyara Anil Kumar Gupta Koshiyara Koshiyara 822124 21 Palamu Bishrampur Lalgarh Md Jainul Abedin Lalgara Lalgara 822124 22 Palamu Bishrampur Rakesh Kumar Dubey Panjri Kalan Panjri Kalan 822124 23 Palamu BishrampurPanjari Kalan Momtaj Ansari Panjri Kalan Panjri Kalan 822124 24 Palamu Bishrampur Rambrat Dubey Panjri Kalan Panjri Kalan 822124 25 Palamu Bishrampur Santosh Prasad Sigsigi Sigsigi 822124 Sigsigi 26 Palamu Bishrampur Salamuddin Ansari Sigsigi Sigsigi 822124 27 Palamu Bishrampur Sordiha Md Mahboob Akhtar Ward No.