Mature Cystic Teratoma Mimicking Ectopic:Layout 1.Qxd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diagnostic Approach to Congenital Cystic Masses of the Neck from a Clinical and Pathological Perspective
Review Diagnostic Approach to Congenital Cystic Masses of the Neck from a Clinical and Pathological Perspective Amanda Fanous 1,†, Guillaume Morcrette 2,†, Monique Fabre 3, Vincent Couloigner 1,4 and Louise Galmiche-Rolland 5,* 1 Pediatric Otolaryngology-Head and Neck Surgery, AP-HP, Hôpital Universitaire Necker Enfants Malades, 75015 Paris, France; [email protected] (A.F.); [email protected] (V.C.) 2 Department of Pediatric Pathology, AP-HP, Hôpital Robert Debré, 75019 Paris, France; [email protected] 3 Department of Pathology, AP-HP, Hôpital Universitaire Necker Enfants Malades, Université Paris Descartes, 75015 Paris, France; [email protected] 4 Faculté de Médecine, Université de Paris, 75015 Paris, France 5 Department of Pathology, University Hospital of Nantes, 44000 Nantes, France * Correspondence: [email protected] † These authors contributed equally to this work. Abstract: Background: neck cysts are frequently encountered in pediatric medicine and can present a diagnostic dilemma for clinicians and pathologists. Several clinical items enable to subclassify neck cyst as age at presentation, anatomical location, including compartments and fascia of the neck, and radiological presentation. Summary: this review will briefly describe the clinical, imaging, pathologi- cal and management features of (I) congenital and developmental pathologies, including thyroglossal duct cyst, branchial cleft cysts, dermoid cyst, thymic cyst, and ectopic thymus; (II) vascular malforma- Citation: Fanous, A.; Morcrette, G.; Fabre, M.; Couloigner, V.; tions, including lymphangioma. Key Messages: pathologists should be familiar with the diagnostic Galmiche-Rolland, L. Diagnostic features and clinicopathologic entities of these neck lesions in order to correctly diagnose them and Approach to Congenital Cystic to provide proper clinical management. -

A Novel SRY Missense Mutation Affecting Nuclear Import in a 46,XY Female Patient with Bilateral Gonadoblastoma
European Journal of Human Genetics (2009) 17, 1642 – 1649 & 2009 Macmillan Publishers Limited All rights reserved 1018-4813/09 $32.00 www.nature.com/ejhg ARTICLE A novel SRY missense mutation affecting nuclear import in a 46,XY female patient with bilateral gonadoblastoma Remko Hersmus1, Bertie HCGM de Leeuw1, Hans Stoop1, Pascal Bernard2, Helena C van Doorn3, Hennie T Bru¨ggenwirth4, Stenvert LS Drop5, J Wolter Oosterhuis1, Vincent R Harley2 and Leendert HJ Looijenga*1 1Department of Pathology, Erasmus MC-University Medical Center Rotterdam, Josephine Nefkens Institute, Daniel den Hoed Cancer Center, Rotterdam, The Netherlands; 2Human Molecular Genetics Laboratory, Prince Henry’s Institute of Medical Research, Clayton, Victoria, Australia; 3Department of Gynaecologic Oncology, Erasmus MC-University Medical Center Rotterdam, Rotterdam, The Netherlands; 4Department of Clinical Genetics, Erasmus MC-University Medical Center Rotterdam, Rotterdam, The Netherlands and 5Department of Pediatric Endocrinology, Erasmus MC-University Medical Center Rotterdam, Sophia, Rotterdam, The Netherlands Patients with disorders of sex development (DSD), especially those with gonadal dysgenesis and hypovirilization, are at risk of developing the so-called type II germ cell tumors (GCTs). Both carcinoma in situ and gonadoblastoma (GB) can be the precursor lesion, resulting in a seminomatous or non- seminomatous invasive cancer. SRY mutations residing in the HMG domain are found in 10–15% of 46,XY gonadal dysgenesis cases. This domain contains two nuclear localization signals (NLSs). In this study, we report a unique case of a phenotypical normal woman, diagnosed as a patient with 46,XY gonadal dysgenesis, with an NLS missense mutation, on the basis of the histological diagnosis of a unilateral GB. -

Ovarian Cysts Before the Menopause
Information for you Published in June 2013 Ovarian cysts before the menopause About this information This information is for you if you are premenopausal (have not gone through the menopause) and your doctor thinks you might have a cyst on one or both of your ovaries. It tells you about cysts on the ovary and the tests and treatment you may be offered. This information aims to help you and your healthcare team make the best decisions about your care. It is not meant to replace advice from a doctor about your situation. What are ovaries? Ovaries are a woman’s reproductive organs that make female hormones and release an egg from a follicle (a small fluid-filled sac) each month. The follicle is usually about 2–3 cm when measured across (diameter) but sometimes can be larger. What is an ovarian cyst? An ovarian cyst is a larger fluid-filled sac (more than 3 cm in diameter) that develops on or in an ovary. A cyst can vary in size from a few centimetres to the size of a large melon. Ovarian cysts may be thin-walled and only contain fluid (known as a simple cyst) or they may be more complex, containing thick fluid, blood or solid areas. There are many different types of ovarian cyst that occur before the menopause, examples of which include: • a simple cyst, which is usually a large follicle that has continued to grow after an egg has been released; simple cysts are the most common cysts to occur before the menopause and most disappear within a few months • an endometrioma – endometriosis, where cells of the lining of the womb are found outside the womb, sometimes causes ovarian cysts and these are called endometriomas (for further information see the RCOG patient information leaflet Endometriosis: What You Need to 1 Know, available at: www.rcog.org.uk/womens-health/clinical-guidance/endometriosis-what-you- need-know) • a dermoid cyst, which develops from the cells that make eggs in the ovary, often contains substances such as hair and fat. -

Ultrasound of Female Pelvic Organ
울산의대 서울아산병원 영상의학과 김미현 Introduction Benign disease of uterus Malignant disease of uterus Non-tumorous condition of ovary Tumorous condition of ovary Transvaginal – 소변(-) Transabdominal – 소변(+) Tranrectal or transperineal - virgin Sonohysterography Thick or irregular endometrium on transvaginal US Endometrium Basal layer – echogenic Functional layer – hypoechoic Endometrial stripe Endometrium 가임기 증식기 4-12 mm 분비기 8-15 mm 폐경기 5 mm 미만 Myometrium Innermost layer junctional zone Ovary Oval shape Central medulla – hyperecho Peripheral cortex (follicle) - hypoecho Benign disease of uterus Ectopic endometrial glands and stroma in the myometrium m/c cause of vaginal bleeding Due to unopposed estrogen Overgrowth of EM glands and stroma US Focally increased EM thickening DDx (HSG-US helpful) Hyperplasia Submucosal myoma < EM cancer m/c pelvic tumor Submucosal, intramural, subserosal US Well-defined hypoechoic solid mass Variable echogenicity due to degeneration Interface vessels btw tumor and uterus bridging vascular sign(+) Subserosal myoma > ovary tumor M U Cause Dilatation and currettage Gestational trophoblastic disease Complication of malignancy Previous surgery Uterine myoma Endometriosis Antagonist of the estrogen receptor in breast tissue Agonist in the endometrium EM hyperplasia Antagonist of the estrogen receptor in breast tissue Agonist in the endometrium EM hyperplasia Malignant disease of uterus Cervical cancer Endometrial cancer Gestational trophoblastic disease US- poor sensitivity for diagnosis • 45F, premenopause • EM -
Torsion of a Large Ovarian Dermoid Cyst in the Second Trimester of Pregnancy and Its Management: a Case Report
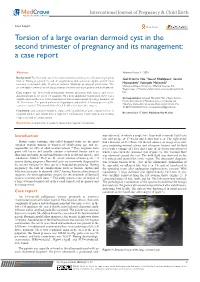
International Journal of Pregnancy & Child Birth Case Report Open Access Torsion of a large ovarian dermoid cyst in the second trimester of pregnancy and its management: a case report Abstract Volume 6 Issue 3 - 2020 Background:The Dermoid cyst is the most common ovarian germ cell tumor in pregnant Goli Kazemi Nia,1 Yousef Khalifpour,1 Saadat women. During pregnancy, the risk of complications such as torsion, rupture,and infection 1 2 increases in dermoid cysts. Treatment includes follow-up or surgical intervention. The Hajatzadeh, Somayeh Makvandi 1Ahvaz Jundishapur University of Medical Sciences, Iran present study reports a case of a large ovarian dermoid cyst in pregnancy and its treatment. 2Department of Midwifery, Islamic Azad university Ahvaz branch, Case report: An 18-year-old primiparous woman presented with nausea and severe Iran abdominal pain in the lower left quadrant. On a deep abdominal examination, there was a palpable mass in the area. Ultrasound showed left ovarian torsion of a large dermoid cyst Correspondence: Somayeh Makvandi, PhD of Reproductive Health, Department of Midwifery, School of Nursing and 10×11cm in size. The patient underwent a laparotomy and with the left ovary preserved, the Midwifery, Islamic Azad university Ahvaz branch, Ahvaz, Iran, cyst was removed. Ultrasound showed fetal health a few days after surgery. Tel 00989166042247, Email Conclusion: gynecologists should be aware of the possibility of acute ovarian torsion in April 17, 2020 | May 08, 2020 pregnant women and should have a high level of suspicion. Early surgical intervention Received: Published: reduces the risk of complications. Keywords: dermoid cyst, pregnancy, laparotomy, vaginal examination Introduction was observed, in which a single live fetus with a normal fetal heart rate and an age of 17 weeks and 4 days was seen. -

Coexisting Pathology of Ectopic Pregnancy and Dermoid Cyst: an Uncommon Occurrence
Case Report Coexisting pathology of ectopic pregnancy and dermoid cyst: An uncommon occurrence Sushma Ramraje1, Sulagna Giri2, Grace D’Costa3, Abhishek Sengupta4 From 1Associate Professor, 2Assistant Professor, 3Professor and Head, 4Resident Pathologist, Department of Pathology, Grant Government Medical College, Mumbai, Maharashtra, India Correspondence to: Dr. Sushma Ramraje, 2/15, Dhanwantari, Sir J J Hospital Campus, Byculla, Mumbai - 400 008, India. E-mail: [email protected] Received – 04 March 2018 Initial Review – 03 April 2018 Published Online – 21 June 2018 ABSTRACT Mature cystic teratomas (dermoid cysts) are common benign ovarian neoplasms. About 10% of dermoid cysts are detected during pregnancy. Multiple gynecologic pathologies occurring together are uncommon, and both an ectopic pregnancy and dermoid cyst are seen concurrently being unknown and poorly documented. Here, we report a case of ectopic pregnancy and dermoid cyst occurring simultaneously in a 30-year-old woman. Key words: Gynecologic, Multiple, Pathologies ature cystic teratomas (dermoid cysts) contribute to done. On per speculum examination, cervix was not visualized about 33% of all benign ovarian neoplasms occurring and was pushed up. On per vaginal examination, the cervix was Mbetween 10 and 30 years of age [1,2]. Majority of felt pushed up. Free fluid was present bilaterally and a mass the dermoid cysts are asymptomatic at diagnosis with 10–15% measuring 12–14 weeks with restricted mobility was felt in the being bilateral. About 10% of dermoid cysts are detected during posterior pouch. pregnancy [3]. She was hemodynamically stable and her hemoglobin and About 1–2% of all reported pregnancies in the developed hematocrit were 10.6 g/dL and 29%, respectively. -
An Unusual Presentation of Ovarian Dermoid Cyst
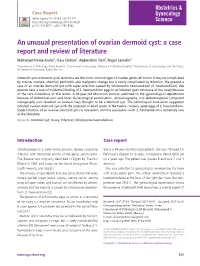
Case Report Obstet Gynecol Sci 2018;61(4):529-532 https://doi.org/10.5468/ogs.2018.61.4.529 pISSN 2287-8572 · eISSN 2287-8580 An unusual presentation of ovarian dermoid cyst: a case report and review of literature Mohamed Amine Azami1, Iliass Elalami2, Abderrahim Siati3, Najjat Lamalmi1 1Department of Pathology, Child Hospital, 2Department of Oncology, Mohamed V Military Hospital, 3Department of Gynecology and Obstetrics, Mohammed V University, Rabat, Morocco Dermoid cysts or mature cystic teratoma are the most common type of ovarian germ cell tumor. It may be complicated by torsion, rupture, chemical peritonitis and malignant change but is rarely complicated by infection. We present a case of an ovarian dermoid cyst with super-infection caused by Schistosoma haematobium (S. haematobium). We present here a case of incidental finding of S. haematobium eggs in an infected cystic teratoma of the ovary because of the rare occurrence of this lesion. A 45-year-old Moroccan woman admitted to the gynecological department because of abdominal pain and fever. Gynecological examination, ultrasonography, and abdominopelvic computed tomography scan revealed an ovarian mass thought to be a dermoid cyst. The pathological evaluation suggested infected ovarian dermoid cyst with the presence of adult worm in the tumor, contains same eggs of S. haematobium. Super-infection of an ovarian dermoid cyst is a rare event, and the association with S. haematobium is extremely rare in the literature. Keywords: Dermoid cyst; Ovary; Infection; Schistosoma haematobium Introduction Case report Schistosomiasis is a water-borne parasitic disease caused by She is a 45-year-old Moroccan patient. She was followed for infection with trematode worms of the genus Schistosoma. -

Epithelioid Trophoblastic Tumor: Clinicopathological Features with an Emphasis on Uterine Cervical Involvement
Modern Pathology (2006) 19, 75–82 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Epithelioid trophoblastic tumor: clinicopathological features with an emphasis on uterine cervical involvement Oluwole Fadare1, Vinita Parkash2, Maria-Luisa Carcangiu3 and Pei Hui1 1Department of Pathology, Yale University School of Medicine, New Haven, CT, USA; 2Department of Pathology, Hospital of Saint Raphael, New Haven, CT, USA and 3Department of Pathology, Istituto Nazionale Tumori, Milan, Italy We report on the clinical and histological features of five cases of epithelioid trophoblastic tumor, with an emphasis on its involvement of the uterine cervix. All five patients were of reproductive age (median age 38.4 years) and all, except one, presented with vaginal bleeding 3 to 18 years after the most recent pregnancy. One patient presented with amenorrhea. Elevation of serum human chorionic gonadotropin (hCG) was seen in four cases. Pathologically, the tumor involved endocervix in three cases and involved uterine corpus in another two. All five tumors were invasive, nodular lesions consisting of epithelioid intermediate trophoblastic cells that were mononuclear with abundant eosinophilic cytoplasm, along with zones of hyaline material and necrotic debris. In three cases of cervical involvement, the neoplastic cells focally replaced endocervical surface and glandular epithelium, simulating high-grade squamous intraepithelial lesions. Immunohistochemically, all five tumors displayed focal positivity for human placental lactogen and hCG. Positive nuclear staining of p63 was seen in all five cases. All patients received total hysterectomy and various regimes of adjuvant chemotherapy. Three patients survived the tumor with no recurrences or metastases with follow-up periods of 3, 7 and 16 years. -

Dermoid Cyst of Testis in a 72-Year-Old Man: a Rare Entity
Case Report Dermoid cyst of testis in a 72-year-old man: A rare entity Vijay Sreedhar Babu Kinnera, Kumaraswamy Reddy Mandyam, Mutheeswaraiah Yootla1, Venkatarami Reddy Vutukuru1 Departments of Pathology and 1General Surgery, Sri Venkateswara Institute of Medical Sciences, Tirupati - 517 507, India Abstract Dermoid cyst is a mature-type teratoma containing sebaceous material and predominantly tufts of hair or teeth along with skin appendages. It is most commonly observed in the ovary but is rare in the testis, and only a few cases have been reported so far. In most of the reports, the cyst tended to be diagnosed in a younger age group. Here, we report a dermoid cyst of the testis in a 72-year-old man. Key Words: Dermoid cyst, mature teratoma, testis Address for correspondence: Dr. Vijay Sreedhar Babu Kinnera, Department of Pathology, Sri Venkateswara Institute of Medical Sciences, Tirupati - 517 507, India. E-mail: [email protected] Received: 17.12.2008, Accepted: 26.02.2009, DOI: 10.4103/0974-7796.56045 INTRODUCTION hernia having bowel contents. Preoperative tumor markers, serum α-fetoprotein (<10 IU/lit.) and human chorionic Dermoid cyst is the most common teratoma of the ovary, gonadotrophin (4.0 IU/lit.), were unremarkable. Subsequently, but is extremely rare in the testis. The incidence of dermoid the patient underwent right high inguinal orchidectomy and cyst is unknown, and its rarity may be due to lack of clinical bilateral inguinal hernia repair by mesh. Postoperative recovery criteria to establish a preoperative diagnosis and the fact that was uneventful. Macroscopically the testis was measuring some cases are grouped under mature teratomas.[1] We report 5.0 × 4.5 × 3.0 cm. -

Germ Cell Tumours of Testis
Classification of GCT Germ Cell Tumours . British Testicular Tumour Panel (BTTP) of Testis •Seminoma; spermatocytic seminoma •Yolk sac tumour (only infantile) Murali Varma Cardiff, UK •Malignant teratoma differentiated (MTD) [email protected] •Malignant teratoma undifferentiated (MTU) •Malignant teratoma intermediate (MTI) •Malignant teratoma trophoblastic (MTT) Sarajevo Nov 2013 Classification of GCT BTTP vs. WHO . WHO . Proportion of components in mixed tumours • WHO: recommends determination of •Seminoma, spermatocytic seminoma proportions •Teratoma: . eg. 75% EC, 10% YST, 10% seminoma, 5% teratoma • Mature/immature/overtly malignant • BTTP: purely descriptive •Embryonal carcinoma . MTI may be 95% MTD or 95% MTU . MTT may be <5% choriocarcinoma •Yolk sac tumour . Focal choriocarcinoma in EC has good prognosis •Choriocarcinoma . Meaning of the term Teratoma •Malignant mixed germ cell tumour • Different in BTTP and WHO Testicular Teratoma Teratoma (WHO) . WHO: . In contrast to ovarian teratomas • Only tumours analogous to ovarian • Most are solid (cf benign cystic teratoma teratoma of ovary) . BTTP • All testicular teratomas in post-pubertal males potentially malignant • All non-seminomatous germ cell tumours • Pure mature teratoma in post-pubertal • Embryonal carcinoma = malignant males has metastatic potential teratoma undifferentiated • Pure mature teratoma in pre-pubertal males is benign 1 Testicular Teratoma Epidermoid cyst . Presence and extent of immaturity . Unilocular, squamous epithelium lined cyst generally not important • Keratinous contents • Do not report “immature teratoma” . No other components . PNET: area greater than 1 low-power . Testis away from cyst normal field of pure immature neuroepithelium • No atrophy • Presence in testis does not alter prognosis • No ITGCN • Presence in metastasis very poor outcome . Adjacent testis may show pressure effects • Chemoresistant • Atrophy, fibrosis Dermoid cyst Dermoid cyst vs. -

Dermoid Cysts and Mucinous Cystadenoma in the Same Ovary and a Review of the Literature
Bostanci et al. Obstet Gynecol cases Rev 2015, 2:2 ISSN: 2377-9004 Obstetrics and Gynaecology Cases - Reviews Case Report: Open Access Collision Tumor: Dermoid Cysts and Mucinous Cystadenoma in the Same Ovary and a Review of the Literature Mehmet Sühha Bostanci1, Ozge Kizilkale Yildirim2, Gazi Yildirim2, Murat Bakacak3, Isin Dogan Ekinci4, Sevgi Bilgen5 and Rukset Attar2* 1Sakarya University Medical School, Obstetrics and Gynecology, Turkey 2Yeditepe University Hospital, Obstetrics and Gynecology, Turkey 3Kahramanmaras Sütçü Imam University Medical School, Obstetrics and Gynecology, Turkey 4Yeditepe University Hospital, Pathology, Turkey 5Yeditepe University Hospital, Anethesiology and Reanimation, Turkey *Corresponding author: Rukset Attar, Yeditepe University Hospital, Obstetrics and Gynecology, Istanbul, Turkey, Tel: 0902165784832/905378401900, E-mail: [email protected] carcinoma and granulosa cell tumor [4], teratoma with granulosa Abstract cell tumor [5], and serous adenocarcinoma and steroid cell tumor Collision tumor is defined as the coexistence of two adjacent, [6]. The juxtaposition with dermoid cysts has been reported as but histologically distinct tumors without histological admixture in the same tissue or organ. Collision tumors involving ovaries are comprising approximately 5% of benign mucinous ovarian tumors extremely rare. The coexistence of a mucinous cystadenoma and rare examples of proliferating mucinous tumors [7]. with a dermoid cyst is infrequently reported. However, the most common histological combination of collision tumor in the ovary is The case is here reported of a rare collision tumor in the ovary the coexistence of teratoma with mucinous tumors. If a dermoid consisting of mucinous cystadenoma and two distinct dermoid cyst accompanies a multiseptated cyst and if the multiseptalcyst tumors. contains fatty foci, these two components may be associated. -

Management of Ovarian Cyst
Management of Ovarian cyst What is an ovarian cyst? An ovarian cyst is a space-occupying lesion that develops within an ovary. How common are ovarian cysts and generally what happens to them? Ovarian cysts are common. Most are benign (non- cancerous), cause no problems and do not require surgical removal. However, 1 in 10 women may require removal of ovarian cyst or the ovary containing the cyst due to complications such as bleeding, rupture, torsion, secondary effect on fertility or concern with malignancy. What is the difference between simple and complex ovarian cyst? Commonly discovered by ultrasound, ovarian cyst is often described by its appearance as simple (thin walled, only containing fluid) or complex (containing a mixture of fluid, blood and solid areas). What are the different types of ovarian cysts? Ovarian cysts are broadly classified as benign, malignant or borderline. Benign ovarian cysts include: • Functional cysts – during a normal ovulatory cycle, a follicle (small cyst) grows, matures and releases an egg. After ovulation, the follicle turns into a corpus luteum. o A follicular cyst occurs when the follicle does not rupture or release its egg. o When the corpus luteum fails to involute and continues to grow, a corpus luteal cyst is formed. • Haemorrhagic cysts form from random bleeding into the inside of a functional cyst. This kind of cyst may cause some discomfort or pain but often resolves spontaneously within 6–8 weeks. • Endometriotic cyst forms as a result of endometriosis developing within the ovary. • Cystadenoma form from different types of cells which secrete clear watery fluid (serous cystadenoma) or thick, sticky fluid (mucinous cystadenoma).