Pathological Grading for Predicting Metastasis in Phaeochromocytoma and Paraganglioma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Grading Evolution and Contemporary Prognostic Biomarkers of Clinically Significant Prostate Cancer
cancers Review Grading Evolution and Contemporary Prognostic Biomarkers of Clinically Significant Prostate Cancer Konrad Sopyllo 1, Andrew M. Erickson 2 and Tuomas Mirtti 1,3,* 1 Research Program in Systems Oncology, Faculty of Medicine, University of Helsinki, 00014 Helsinki, Finland; konrad.sopyllo@helsinki.fi 2 Nuffield Department of Surgical Sciences, University of Oxford, Oxford OX3 9DU, UK; [email protected] 3 Department of Pathology, HUS Diagnostic Centre, Helsinki University Hospital, 00029 Helsinki, Finland * Correspondence: tuomas.mirtti@helsinki.fi Simple Summary: Prostate cancer treatment decisions are based on clinical stage and histological diagnosis, including Gleason grading assessed by a pathologist, in biopsies. Prior to staging and grading, serum or blood prostate-specific antigen (PSA) levels are measured and often trigger diagnostic examinations. However, PSA is best suited as a marker of cancer relapse after initial treatment. In this review, we first narratively describe the evolution of histological grading, the current status of Gleason pattern-based diagnostics and glance into future methodology of risk assessment by histological examination. In the second part, we systematically review the biomarkers that have been shown, independent from clinical characteristics, to correlate with clinically relevant end-points, i.e., occurrence of metastases, disease-specific mortality and overall survival after initial treatment of localized prostate cancer. Abstract: Gleason grading remains the strongest prognostic parameter in localized prostate ade- nocarcinoma. We have here outlined the evolution and contemporary practices in pathological evaluation of prostate tissue samples for Gleason score and Grade group. The state of more observer- Citation: Sopyllo, K.; Erickson, A.M.; Mirtti, T. Grading Evolution and independent grading methods with the aid of artificial intelligence is also reviewed. -

Metastatic Potential Prediction by a Visual Grading System of Cell Motility: Prospective Validation in the Dunning R-3327 Prostatic Adenocarcinoma Model1
(CANCER RESEARCH 48. 4312-4317, August 1, 1988] Metastatic Potential Prediction by a Visual Grading System of Cell Motility: Prospective Validation in the Dunning R-3327 Prostatic Adenocarcinoma Model1 James L. Mohler,2 Alan W. Partin,3 John T. Isaacs, and Donald S. Coffey Department of Urology, The Johns Hopkins University School of Medicine and The Johns Hopkins Oncology Center, Baltimore, Maryland 21205 ABSTRACT At present many grading systems are used to assess the metastatic potential of prostatic carcinoma. Whether these A method for accurate prediction of prognosis in individual patients grading systems describe architectural (3), cytological (4), or with prostatic carcinoma does not exist. The limitations of pathological some combination of both features (5-8), they share the short grading systems may result from the failure of standard pathological examination of fixed dead tissue to accurately assess the biological and coming of relying upon the examination of dead tissue to predict metastatic behavior of live tumor cells. Many of the sublines of the the biological behavior of a living dynamic tumor system. At Dunning R-3327 rat prostatic adenocarcinoma are histologically similar present no grading system has utilized living cancer cells that yet differ in metastatic potential. Cells from the Dunning model were may possess biological properties that are related to the aggres grown in culture and filmed by time-lapse videomicroscopy. These cells siveness of neoplasms. Cancer cell motility is an obvious ex exhibited characteristic membrane ruffling, pseudopodal extension, and ample of a property that would be lost with fixation but may cellular translation that could be graded with 80% reproducibility. -

Breast Cancer Grading Poster
Breast Cancer Grading Nottingham Criteria Accurate grading of invasive breast cancer requires good fixation, processing, section cutting, staining and careful application of grading criteria. In the UK, about 20% of symptomatic breast cancers are grade 1, 30% grade 2, and 50% grade 3. These proportions may be different in asymptomatic cancers detected by mammographic screening. Special type cancers (lobular, etc) should also be graded. Three separate scores are given: ThisGland (acinus) formation Score 1: more than 75% of the whole carcinoma forms acini Only score clearly formed glandular lumens surrounded Score 2: 10–75% of the whole carcinoma forms acini by polarised cancer cells Score 3: less than 10% of the whole carcinoma forms acini Nuclearpublication atypia/pleomorphism Only about 5% of symptomatic cancers score 1 for nuclear atypia; about 50% score 3. Score 1: nuclei only slightly larger than benign breast epithelium (< 1.5 × normal area); minor variation in size, shape and chromatin pattern Score 2: nuclei distinctly enlarged (1.5–2 × normal area), often vesicular, nucleoli visible; may be distinctly variable in size and shape but not always Score 3: markedly enlarged vesicular nuclei (> 2 × normal area), nucleoli often prominent; generally marked variation in size and shape but atypia not necessarily extreme was archived Nuclei of 20 consecutive breast cancers by increasing mean nuclear area (left to right, top to bottom). Paired non-neoplastic breast epithelium is shown above each case for comparison. Only one cancer (top left) has nuclei which score 1. The others in the top row score 2. All 10 in the bottom row score 3. -
Lung Cancer: Clinical Presentation, Epidemiology, 1 Tumor Staging, Classification, Histologic Grading, and Spread Through Air Spaces
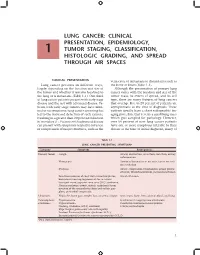
LUNG CANCER: CLINICAL PRESENTATION, EPIDEMIOLOGY, 1 TUMOR STAGING, CLASSIFICATION, HISTOLOGIC GRADING, AND SPREAD THROUGH AIR SPACES CLINICAL PRESENTATION vena cava, or metastasis to distant sites such as Lung cancer presents in different ways, the bone or brain (Table 1-1). largely depending on the location and size of Although the presentation of primary lung the tumor and whether it remains localized to cancer varies with the location and size of the the lung or is metastatic (Table 1-1). One third tumor mass, its extent of spread, and its cell of lung cancer patients present with early stage type, there are many features of lung cancers disease and the rest with advanced disease. Pa- that overlap. Five to 20 percent of patients are tients with early stage tumors may have mini- asymptomatic at the time of diagnosis. These mal or no symptoms; lung cancer screening has patients usually have a chest radiographic im- led to the increased detection of such cancers, aging procedure that reveals a small lung mass resulting in a greater than 20 percent reduction which gets sampled for pathology. However, in mortality (1). Patients with advanced disease over 80 percent of new lung cancer patients can present with symptoms related to invasion have one or more symptoms referable to their or compression of major structures, such as the disease at the time of initial diagnosis, many of Table 1-1 LUNG CANCER PRESENTING SYMPTOMSa Category Symptom Pathogenesis Primary tumor Cough Airway obstruction, atelectasis, infection, airway infammation Hemoptysis -

Coding Guidelines PROSTATE GLAND C619 Grade Note
SEER Program Coding and Staging Manual 2012 Coding Guidelines PROSTATE GLAND C619 Grade Note: These guidelines pertain to the data item Grade. Refer to the Collaborative Stage Data Collection Manual for instructions on coding site-specific factors for prostate cases. Priority Rules for Grading Prostate Cancer Code the tumor grade using the following priority order 1. Gleason score (Use the table to convert Gleason score to the appropriate code) 2. Terminology Differentiation (well differentiated, moderately differentiated, etc) 3. Histologic grade Grade i, grade ii, grade iii, grade iv 4. Nuclear grade only Gleason Pattern Prostate cancers are commonly graded using Gleason score or pattern. Gleason grading is based on a 5- component system, based on 5 histologic patterns. The pathologist will evaluate the primary pattern (most predominant) and secondary patterns (second most predominant) for the tumor. Example: A Gleason pattern of 2 + 4 means that the primary pattern is 2 and the secondary pattern is 4. Gleason Score The primary and secondary patterns are added together to create a score. Primary pattern is doubled when there is no secondary pattern. Tertiary pattern is not used to determine Gleason score. Example: If the patterns are 2 + 4, the score is 6. If the pathology report contains only one number, and that number is less than or equal to 5, it is a pattern. If the pathology report contains only one number, and that number is greater than 5, it is a score. If the pathology report specifies a specific number out of a total of 10, the first number given is the score. -
Grading of Prostatic Adenocarcinoma: Current State and Prognostic Implications Jennifer Gordetsky1,2 and Jonathan Epstein3,4*
Gordetsky and Epstein Diagnostic Pathology (2016) 11:25 DOI 10.1186/s13000-016-0478-2 REVIEW Open Access Grading of prostatic adenocarcinoma: current state and prognostic implications Jennifer Gordetsky1,2 and Jonathan Epstein3,4* Abstract Background: Despite significant changes in the clinical and histologic diagnosis of prostate cancer, the Gleason grading system remains one of the most powerful prognostic predictors in prostate cancer. The correct diagnosis and grading of prostate cancer is crucial for a patient’s prognosis and therapeutic options. However, this system has undergone significant revisions and continues to have deficiencies that can potentially impact patient care. Main Body: We describe the current state of grading prostate cancer, focusing on the current guidelines for the Gleason grading system and recent changes from the 2014 International Society of Urological Pathology Consensus Conference on Gleason Grading of Prostatic Carcinoma. We also explore the limitations of the current Gleason grading system and present a validated alternative to the Gleason score. The new grading system initially described in 2013 in a study from Johns Hopkins Hospital and then validated in a multi-institutional study, includes five distinct Grade Groups based on the modified Gleason score groups. Grade Group 1 = Gleason score ≤6, Grade Group 2 = Gleason score 3 + 4 = 7, Grade Group 3 = Gleason score 4 + 3 = 7, Grade Group 4 = Gleason score 8, Grade Group 5 = Gleason scores 9 and 10. Conclusion: As this new grading system is simpler and more accurately reflects prostate cancer biology, it is recommended by the World Health Organization (WHO) to be used in conjunction with Gleason grading. -

(NCCN) Breast Cancer Clinical Practice Guidelines
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Breast Cancer Version 5.2020 — July 15, 2020 NCCN.org NCCN Guidelines for Patients® available at www.nccn.org/patients Continue Version 5.2020, 07/15/20 © 2020 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN. NCCN Guidelines Index NCCN Guidelines Version 5.2020 Table of Contents Breast Cancer Discussion *William J. Gradishar, MD/Chair ‡ † Sharon H. Giordano, MD, MPH † Sameer A. Patel, MD Ÿ Robert H. Lurie Comprehensive Cancer The University of Texas Fox Chase Cancer Center Center of Northwestern University MD Anderson Cancer Center Lori J. Pierce, MD § *Benjamin O. Anderson, MD/Vice-Chair ¶ Matthew P. Goetz, MD ‡ † University of Michigan Fred Hutchinson Cancer Research Mayo Clinic Cancer Center Rogel Cancer Center Center/Seattle Cancer Care Alliance Lori J. Goldstein, MD † Hope S. Rugo, MD † Jame Abraham, MD ‡ † Fox Chase Cancer Center UCSF Helen Diller Family Case Comprehensive Cancer Center/ Comprehensive Cancer Center Steven J. Isakoff, MD, PhD † University Hospitals Seidman Cancer Center Massachusetts General Hospital Amy Sitapati, MD Þ and Cleveland Clinic Taussig Cancer Institute Cancer Center UC San Diego Moores Cancer Center Rebecca Aft, MD, PhD ¶ Jairam Krishnamurthy, MD † Karen Lisa Smith, MD, MPH † Siteman Cancer Center at Barnes- Fred & Pamela Buffet Cancer Center The Sidney Kimmel Comprehensive Jewish Hospital and Washington Cancer Center at Johns Hopkins University School of Medicine Janice Lyons, MD § Case Comprehensive Cancer Center/ Mary Lou Smith, JD, MBA ¥ Doreen Agnese, MD ¶ University Hospitals Seidman Cancer Center Research Advocacy Network The Ohio State University Comprehensive and Cleveland Clinic Taussig Cancer Institute Cancer Center - James Cancer Hospital Hatem Soliman, MD † and Solove Research Institute P. -

An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Reet Pai, MD
An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Reet Pai, MD University of Pittsburgh Medical Center Pittsburgh, PA Session Outline Topic 1: Classification and Staging of Low- Grade Appendiceal Mucinous Neoplasm • Peritoneal Surface Oncology Group International (PSOGI) classification proposal • AJCC 8th Edition staging update Topic 2: Classification and Grading of Mucinous Adenocarcinoma • PSOGI and AJCC 8th Edition Terminology and Grading Schemes • “Grey zone areas” in classifying peritoneal disease The Problem of Terminology • Peritoneal Surface Oncology Group International (PSOGI) recognized persistent lack of uniform diagnostic terminology in appendiceal mucinous neoplasia • A working group of 71 participants (surgical pathology, surgical oncology, medical oncology) from 13 countries on appendiceal mucinous neoplasia led by Dr. Norman Carr of Basingstoke Hospital in the United Kingdom • Adopted a consensus on diagnostic terminology published in the American Journal of Surgical Pathology in 2016 The Problem of Terminology Classification schemes used by participants prior to PSOGI consensus proposal. No. of Confined to Dissecting Pushing invasion Infiltrative Signet Ring Cells Responses mucosa Mucin Invasive 11 ? Low-grade mucinous Mucinous adenocarcinoma neoplasm (LAMN) 5 Adenoma Low-grade mucinous Mucinous adenocarcinoma neoplasm (LAMN) 8 ? ? Low-grade High-grade High-grade mucinous mucinous mucinous adenocarcinoma adenocarcinoma adenocarcinoma with signet ring cells 6 ? ? Low-grade High-grade mucinous -

Independent Predictors of Breast Malignancy in Screen-Detected Microcalcifications: Biopsy Results in 2545 Cases
British Journal of Cancer (2011) 105, 1669 – 1675 & 2011 Cancer Research UK All rights reserved 0007 – 0920/11 www.bjcancer.com Independent predictors of breast malignancy in screen-detected microcalcifications: biopsy results in 2545 cases ,1 2 1 1 1 G Farshid* , T Sullivan , P Downey , PG Gill and S Pieterse 1 2 BreastScreen SA and SA Pathology, 1 Goodwood Road, Wayville, South Australia 5034, Australia; Data Management and Analysis Centre, Discipline of Public Health, University of Adelaide, Adelaide, Australia BACKGROUND: Mammographic microcalcifications are associated with many benign lesions, ductal carcinoma in situ (DCIS) and invasive cancer. Careful assessment criteria are required to minimise benign biopsies while optimising cancer diagnosis. We wished to evaluate Clinical Studies the assessment outcomes of microcalcifications biopsied in the setting of population-based breast cancer screening. METHODS: Between January 1992 and December 2007, cases biopsied in which microcalcifications were the only imaging abnormality were included. Patient demographics, imaging features and final histology were subjected to statistical analysis to determine independent predictors of malignancy. RESULTS: In all, 2545 lesions, with a mean diameter of 21.8 mm (s.d. 23.8 mm) and observed in patients with a mean age of 57.7 years (s.d. 8.4 years), were included. Using the grading system adopted by the RANZCR, the grade was 3 in 47.7%; 4 in 28.3% and 5 in 24.0%. After assessment, 1220 lesions (47.9%) were malignant (809 DCIS only, 411 DCIS with invasive cancer) and 1325 (52.1%) were non-malignant, including 122 (4.8%) premalignant lesions (lobular carcinoma in situ, atypical lobular hyperplasia and atypical ductal hyperplasia). -

Advances and Controversies in Grading and Staging of Renal Cell Carcinoma
Modern Pathology (2009) 22, S24–S36 & 2009 USCAP, Inc All rights reserved 0893-3952/09 $32.00 www.modernpathology.org Advances and controversies in grading and staging of renal cell carcinoma Brett Delahunt Department of Pathology and Molecular Medicine, Wellington School of Medicine and Health Sciences, University of Otago—Wellington, Wellington, New Zealand Despite the considerable progress made in our understanding of the pathogenesis, genetics, and pathology of renal cell carcinoma (RCC), difficulties remain relating to the prediction of clinical outcome for individual cases. Although there is evidence to show that high-grade tumors have a poorer prognosis when compared to those of low grade, debate remains regarding the predictive value of grading, especially for those tumors classified into the intermediate grades. Numerous composite morphologic and nuclear grading systems have been proposed for RCC and although that of the Fuhrman classification have achieved widespread usage, the validity of the grading criteria of this classification has been questioned. In addition, there are few studies that have attempted to validate the Fuhrman system for RCCs beyond that of the clear cell subtype. Recent studies have indicated that grading of papillary RCC should be based on nucleolar prominence alone and that the components of the Fuhrman grading classification do not provide prognostic information for chromophobe RCC. Independent of tumor grade, the prognostic importance of tumor stage for RCC is well recognized. The Union Internationale Contre le Cancer/American Joint Committee for Cancer Staging and End Results Reporting TNM staging system is now in its sixth edition (2002) and recent refinements have focused on defining size cut points that will identify apparently localized tumors that will develop recurrence and/or metastases despite attempted curative surgery. -

Solid Tumour Section Mini Review
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Solid Tumour Section Mini Review Bone: Giant cell tumour Ramses G Forsyth, Pancras CW Hogendoorn N. Goormaghtigh Institute of Pathology, University Hospital Ghent, B-9000 Gent, Belgium (RGF); Department of Pathology, Leiden University Medical Center, Leiden, the Netherlands (PCWH) Published in Atlas Database: June 2003 Online updated version: http://AtlasGeneticsOncology.org/Tumors/BoneGiantCellTumID5150.html DOI: 10.4267/2042/37996 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 2.0 France Licence. © 2003 Atlas of Genetics and Cytogenetics in Oncology and Haematology Identity A characteristic well-defined eccentric, lytic subchondral lesion involving the epiphysis and metaphysis. The borders are well defined and usually not sclerotic. Pathologic fracture is present in 5-10% of giant cell tumours. Dynamic MRI shows a fast uptake and a slow wash out of contrast. Atlas Genet Cytogenet Oncol Haematol. 2003; 7(3) 194 Bone: Giant cell tumour Forsyth RG, Hogendoorn PCW Alias Pathology Osteoclastoma; Giant cell tumour of bone A mixture of four components can be distinguished: - spindled-shaped and rounded mononuclear cells, Clinics and pathology - osteoclastic-type giant cells and small blood vessels. Disease The spindle-shaped mononuclear cells are regarded as neoplastic on results from electron microscopy and cell Locally destructive, benign and mono-ostotic tumoral cultures. The origin of this cell type is still unknown, lesion, typically presenting in the meta-epiphysis of but it is thought to arise from the primitive long tubular bones with predilection for the knee region mesenchymal stromal cell. -

Testing Different Brain Metastasis Grading Systems in Stereotactic Radiosurgery: Radiation Therapy Oncology Group's RPA, SIR
J Neurosurg (Suppl) 117:31–37, 2012 Testing different brain metastasis grading systems in stereotactic radiosurgery: Radiation Therapy Oncology Group’s RPA, SIR, BSBM, GPA, and modified RPA Clinical article TORU SERIZAWA, M.D.,1 YOSHINORI HIGUCHI, M.D.,2 OSAMU NAGANO, M.D.,3 TAtsUO HIRAI, M.D.,4 JUNICHI ONO, M.D.,3 NAOKAtsU SAEKI, M.D.,2 AND AKIFUMI MIYAKAWA, M.D.4,5 1Tokyo Gamma Unit Center, Tsukiji Neurologic Clinic, Tokyo; 2Department of Neurological Surgery, Chiba University Graduate School of Medicine, Chiba; 3Gamma Knife House, Chiba Cardiovascular Center, Ichihara; 4Stereotaxis and Gamma Unit Center, Fujieda Heisei Memorial Hospital, Fujieda; and 5Department of Radiology, Graduate School of Medical Science and Medical School, Nagoya City University, Nagoya, Japan Object. The authors conducted validity testing of the 5 major reported indices for radiosurgically treated brain metastases— the original Radiation Therapy Oncology Group’s Recursive Partitioning Analysis (RPA), the Score Index for Radiosurgery in Brain Metastases (SIR), the Basic Score for Brain Metastases (BSBM), the Graded Prognostic Assessment (GPA), and the subclassification of RPA Class II proposed by Yamamoto—in nearly 2500 cases treated with Gamma Knife surgery (GKS), focusing on the preservation of neurological function as well as the traditional endpoint of overall survival. Methods. The authors analyzed data from 2445 cases treated with GKS by the first author (T.S.), the primary surgeon. The patient group consisted of 1716 patients treated between January 1998 and March 2008 (the Chiba series) and 729 pa- tients treated between April 2008 and December 2011 (the Tokyo series). The interval from the date of GKS until the date of the patient’s death (overall survival) and impaired activities of daily living (qualitative survival) were calculated using the Kaplan-Meier method, while the absolute risk for two adjacent classes of each grading system and both hazard ratios and 95% confidence intervals were estimated using the Cox proportional hazards model.