Angul, Odisha DISTRICT DEMOGRAPHIC PROFILE Insert Map Here
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
ANGUL Adarsha ITC, At/PO-Rantalei,Dist- 338 101400 Angul 2 ANGUL Akhandalmani ITC , At/Po
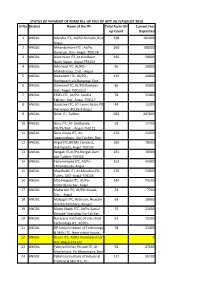
STATUS OF PAYMENT OF FORM FILL-UP FEES OF AITT JULY/AUGUST 2018 Sl No District Name of the ITI Total Form fill- Current fees up Count Deposited 1 ANGUL Adarsha ITC, At/PO-Rantalei,Dist- 338 101400 Angul 2 ANGUL Akhandalmani ITC , At/Po. 360 108000 Banarpal, Dist- Angul- 759128 3 ANGUL Aluminium ITC,At-Kandasar, 196 58800 Nalco Nagar, Angul-759122 4 ANGUL Ashirwad ITC, At/PO - 96 28800 Mahidharpur, Dist.- Angul 5 ANGUL Biswanath ITC, At/PO - 136 40800 Budhapank,via-Banarpal, Dist.- 6 ANGUL Diamond ITC, At/PO-Rantalei, 86 25800 Dist- Angul-759122,0 7 ANGUL ESSEL ITC, At/PO- Kaniha 78 23400 Talcher, Dist.-Angul-759117 8 ANGUL Gayatree ITC, AT-Laxmi Bazar,PO- 44 13200 Vikrampur,FCI,Dist-Angul 9 ANGUL Govt. ITI, Talcher 692 207600 10 ANGUL Guru ITC, At- Similipada, 59 17700 PO/PS/Dist. - Angul-759122 11 ANGUL Guru Krupa ITC, At- 170 51000 Jagannathpur, Via-Talcher, Dist- 12 ANGUL Angul ITC,(RCMS Campus), 260 78000 Hakimpada, Angul-759143 13 ANGUL Rengali ITI,At/Po-Rengali Dam 261 78300 site,Talcher-759105 14 ANGUL Kaminimayee ITC, At/Po- 153 45900 Chhendipada, Angul 15 ANGUL Maa Budhi ITI, At-Maratira,PO- 176 52800 Tubey, DIST-Angul-759145 16 ANGUL Maa Hingula ITC, At/Po- 244 73200 talabrda,talcher, Angul 17 ANGUL Maharishi ITC, At/PO-Kosala, 24 7200 Dist. - Angul 18 ANGUL Malyagiri ITC, Batisuan, Nuasahi 63 18900 Dimiria Pallahara, Anugul 19 ANGUL Matru Shakti ITC, At/Po-Samal 72 21600 Barrage Township,Via-Talcher, 20 ANGUL Narayana Institute of Industrial 51 15300 Technology ITC, At/PO- 21 ANGUL OP Jindal Institute of Technology 78 23400 & Skills ITC, Near cricuit house, 22 ANGUL Orissa ITC, At/Po-Panchamahala 0 Dist-Angul-759122 23 ANGUL Pabitra Mohan Private ITI, At- 92 27600 Manikmara, Po-Dharampur, Dist- 24 ANGUL Pallahara Institute of Industrial 117 35100 Training & Skill ITC, At - 25 ANGUL Pathanisamanta ITC,S-2/5 191 57300 Industrial Estate, Hakimpada, 26 ANGUL Satyanarayan ITC, At-Boinda, PO- 0 Kishoreganj, Dist-Angul – 27 ANGUL Shreedhriti ITC, Jagannath 114 34200 Nagar, Po-Banarpal, Dist-Angul- 28 ANGUL Shivashakti ITC, At -Bikashnagar, 0 Tarang, Dist. -

Tehsil Name DDO Code Office Name Amount Agalpur RDD010 RURAL
Tehsil Name DDO Code Office Name Amount Agalpur RDD010 RURAL WORKS DIVISION, BOLANGIR 11497 Agalpur WAT001 MINOR IRRIGATION DIVISION, BOLANGIR 33091 Ambabhona RDD004 RURAL WORKS DIVISION, BARGARH 7319 Ambabhona WAT007 MINOR IRRIGATION DIVISION, PADAMPUR 40612 Anandapur WOR072 ROADS & BUILDINGS DIVISION, GHATAGAON 23576 Anandapur IRR060 BAITARANI DIVISION, SALAPADA 4920556 Anandapur IRR144 F.A & C.A.O, Anandapur Barrage Project, Salapada 124670 Anandapur WAT017 MINOR IRRIGATION DIVISION, ANANDAPUR 42499 Angul WOR001 ROADS & BUILDINGS DIVISION, ANGUL 446399 Angul WAT028 MINOR IRRIGATION DIVISION, ANGUL 82962 Angul HUD021 PUBLIC HEALTH DIVISION, ANGUL 2940 Aska RDD001 RURAL WORKS DIVISION, GANJAM-I 9241 Aska IRR042 Bhanjanagar Irrigation Division, Bhanjanagar 2917943 Aska IRR127 Drainage Division, Berhampur 7656 Astaranga RWS022 RWSS DIVISION, PURI 4674 Astaranga IRR081 Nimpara Irrigation Division 907773 Athagarh WOR021 ROADS & BUILDINGS DIVISION, CHARBATIA 36967 Athagarh IRR115 F.A & C.A.O, R.R.C.S, Mahishapat, Dhenkanal 401076 Athagarh IRR034 Mahanadi South Division No-I,Jobra, Cuttack 980598 Athagarh WAT003 MINOR IRRIGATION DIVISION, CUTTACK 65298 Athamallik WOR001 ROADS & BUILDINGS DIVISION, ANGUL 920905 Athamallik IRR002 Manjore Irrigation Division,Athmallik 1305746 Athamallik WAT028 MINOR IRRIGATION DIVISION, ANGUL 46274 Attabira RDD004 RURAL WORKS DIVISION, BARGARH 9025 Attabira WOR058 ROADS & BUILDINGS DIVISION, BARAGARH 1701787 Attabira WAT007 MINOR IRRIGATION DIVISION, PADAMPUR 32367 Attabira IRR085 Sambalpur Irrigation Division -

Tahasildar, Talcher
IN RESPECT OF BANABASPUR SAND BED FOR WINING OF RIVER SAND OVER AN AREA OF 17.18 ACRES OR 6.872 HECTARES IN VILLAGE- BANABASPUR, TAHASIL-TALCHER OF ANGUL DISTRICT, ODISHA PREPARED FOR & ON BEHALF OF TAHASILDAR, TALCHER DISTRICT-ANGUL, ODISHA APPENDIX 1 FORM – I (I) Basic Information SL.NO. ITEM DETAILS 1 Name of the Project/s Banabaspur sand Quarry (Singharha jor River) 2 SL. No. in the Schedule Project Activity 1(a) (i) Mining of Minerals. Propose Capacity/ area/ length/ Proposed Production Capacity – tonnage to be handled/command About 12500 Cum of Sand will be 3 area/ lease area/number or wells produced during the Plan Period to be drilled Total Lease Area- 17.18 Acres or 6.872 Ha 4 New/Expansion/Modernization New 5 Existing Capacity/Area etc. Not Applicable, since it is a new project. Category of Project i.e. 'A' or 'B' It is a category ‘B’ project. (<25 Ha all the minor mineral mining lease areas are considered as B2, as per 6 MoEF, GoI, Office Memorandum No. J-13012/12/2013-IA-II ( I), d a t e d : 24-12-2013). non coal mine lease) Does it attract the general 7 No Condition? If yes, please specify. 8 Does it attract the specific Condition? If yes, please specify No The applied area over 6.872 hectares is located in village- Banabaspur and is bounded by 20°59I15.3II N to Location 20°59I40.7II N and 85°02I22.0II E to 85°02I49.8II E. 9 Plot No.- 61, Khata No.- 106 Plot/Survey/Khasra No. -

Physico-Chemical Analysis of Ground Water in Angul-Talcher Region of Orissa, India
Marsland Press Journal of American Science 2009;5(5):53-58 Physico-Chemical Analysis of Ground Water in Angul-Talcher Region of Orissa, India Rizwan Reza1 and Gurdeep Singh2 1JRF, Dept. of Environmental Science & Engineering, ISM University, Dhanbad, Jharkhand, India 2Professor and Head, Dept. of Environmental Science & Engineering, ISM University, Dhanbad, Jharkhand, India Email: [email protected] ABSTRACT: The study was carried out to assess the impacts of industrial and mining activities on the ground water quality in Angul-Talcher region of Orissa. The quality was assessed in terms of physio-chemical parameters. Ground water samples were collected from thirteen (13) open well at various locations in study area during pre and post monsoon season. The physico-chemical parameters such as pH, Electrical conductivity, TDS, Total hardness, Ca hardness, Mg hardness, Ca ion, Mg ion, Chloride, and COD were analyzed (APHA, 1998) to know the present status of the groundwater quality. Drinking water quality (IS: 10500) of pre-monsoon season was better than post monsoon season. Few water samples were slightly alkaline along with high dissolved solids. [The Journal of American Science. 2009;5(5):53-58]. (ISSN 1545-1003). Key words: Ground water, physico-chemical parameters, water quality, drinking water standard INTRODUCTION: contamination of ground water (Jinwal and Dixit, 2008). The incidence of ground water pollution is highest in The safe portable water is absolutely essential for urban areas where large volumes of waste are healthy living. Ground water is ultimate and most concentrated and discharge into relatively small areas suitable fresh water resource for human consumption in (Rao and Mamatha, 2004). -

List of PHC {N) SI. No District C.H.C Si. No .P.H.C {NJ Angul BANAMIRA > Angul 2 PURUNAGARH :.- Angul Banta La PURUNA !(OTE
- List of PHC {N) - 0 SI. No District C.H.C s- I. No .P.H.C {NJ Angul 1 BANAMIRA > -- Angul 2 PURUNAGARH :.-_ -- Angul Banta la 3 PURUNA_!(OTE Angul 4 - JAGANNATHPUR ,- Angul 5 TAINSI MHU -- Angul 6- PAIKSAHI / Madhapu Angul 7 {THAKURGARH le r Angul 8 PATAKA. C Angul I® - - 9 BADAKE RAJANGA A»g , Angul 10 . BALARAMPRASAD Banarpal_ Angul 11 MARATIRAHAT / - Angul 12 , TALAMUL - - Angul 13 BAGEDIA Angul 14 Kosala JARAPADA Angul 15 BALIPATA 1 ·- Angul 16 Patrapada - Angul 17 BAJRAKOTE. Angul 18 BIROO -· Kaniha a Angul .. 19 PABITRANAGAR Angul 20 Kuluma (Angul 21 CHASA GURUJANGA Angul 22 JAMARDIHI 7 Angul Khamar 23 JHARBEDA / Angul 24 RAJADANGA Angul 25 SAHAR GURUJUNGA ,,,,--_ Angul 26 Raj ANGAPADA Angul 27 HANDAPA K.Nagar Angul 28 BOINDA. - Angul 29 Godiban KALLAM CHHULN · » Angul 30 GOPAL PRASAD - dha Angul 31 KANKILL - Balasore 32 Ghantua Balasore 33 LANGALES WAR Balasore Baliapal 34 SRIRAMPUR -- Balasore 35 JAMAKUNDA A Balasore 36 Bolanga g Balasore 37 AMARDA ROAD Balasore 38 IRDA.· so , Balasore Basta 39 PAUNSAKALI Balasore 40 SANTOSH UR Balasore 41 SINGLA Balasore 42 BHOGORAI Balasore 43 CHANDANESWAR Balasore 44 DAHAMUNDA · Joo Balasore g Iola¢urn 45 DEULA 0 JQI>VVa Balasore 46 Pur JALASUHARIA , Balasore 47 KAKHADA Balasore 48 NIMATPUR Balasore 49 Jayarampur Balasore .. so 1SRADHAP UR , Balasore 51 GARASANGA - Balasore 52 ANTARA· - J Balasore 53 / Khaira DUNGURA Balasore / I 54 GANDIBED Balasore 55 K UPARI - Balasore 56 TUDIGADIA Balasore 57 KESHARIPUR Balasore 58 BAGUDI - a, - Bala sore Soro 59 DANDAPALASA - Balasore , 60 MANIPUR ,, - Balasore 61 - PAKHAR - Balasore All 62 BAHANAGA· a Balasore Gopal 63 BISHNUPUR Jo Balasore Pur 64 KHARASAHAPUR ®e Balasore 65 SAUD Balasore 66 BASANTI SINDHIA 2 Balasore 67 PALASAPUR . -

Proceedidng of the Permit Grant Committee Meeting
PROCEEDIDNG OF THE PERMIT GRANT COMMITTEE MEETING OF STA, ODISHA, CUTTACK HELD IN THE 7th FLOOR CONFERENCE HALL OF TRANSPSORT COMMISSIONER-CUM-CHAIRMAN,STA, ODISHA ON 23RD SEPTEMBER, 2019. 1. ROUTE- ANGUL TO ROURKELA, VIA-KHAMAR, BALIPASI AND BACK. VEHICLE NO. Vehicle No.OR19K-6937, CMD, OSRTC, BHUBANESWAR The applicant is represented by Sri Bibhuti Samal Sri Ashok Ku. Pattanayak and Pradipta Kumar Nayak the employees of OSRTC. There are two objections 1. Sri Bijay Kumar Sahoo, owner of vehicle No.OD19F-0096 ob:ected that the applied vehicle will start from Angul 05 minutes ahead or his vez-licie 2. Sri Dileswar Samal, owner of vehicle No.OD05H-421.6 has tiled objection stating that OSRTC has applied 10 minutes ahead of his timing There is clash of timing from Khamar to Rourkela. This may be verified. 2 ROUTE- BAHARANA TO SATAPADA, VIA-UTTARA CHHAK. PiPID .L\NDBACK VEHICLE NO OR19H-0747, CMD, OSRTC, BHUBANESWAR The applicant is represented by Sri Bibhuti Samal Sri Ashok Ku Pattanayak and Pradipta Kumar Nayak, the employee of OSRTC There is no objection. T.P. may be considered after checking of clash free timing. 3. ROUTE- JHARSUGUDA TO MALKANGIRI, VIA-NABARANGPUR, VEHICLE .OD17L- 0728, CMD, OSRTC, BHUBANESWAR The applicant is represented by Sri Bibhuti Sa, al Si Ashok Ku. Pattanayak and Pradipta Kumar Nayak, the employee of OSRTC. 1'nere is no objection. This is alter service of OD17L-0725. T.P. may be cori:deed as per the timing of the alter service. 4. ROUTE- PADAMPUR TO SONEPUR, VIA-DUDUKA, SALEBHATA AND BACK VEHICLE NO.ODO2BC-6649, CMD, OSRTC, BHUBANESWAR The applicant is represented by Sri Bibhuti Samal, S:i ;\shok Ku. -
![(AI) Details [District Wise]](https://docslib.b-cdn.net/cover/3941/ai-details-district-wise-1193941.webp)
(AI) Details [District Wise]
National Institute of Open Schooling Regional Centre, Bhubaneswar Study Centre (AI) Details [District Wise] Sl No. AI/ Study Centre Code Name & Address of Study Centre (AI) District 1 150147/410104 Govt. High School,Phulamba, Po-Kalyanpur,Via-Rajkishore Nagar Dist-Angul, Angul Orissa, PIN-759126 Mob:9438511716. 2 150146/410103 Govt. Girls High School, At/Po-Jamardini, Via-Pallahara, Dist-Angul, Orissa, Angul Mb-9338842157,9583491446 3 150037 Jawahar Navodaya Vidyalaya, At-F.C.I, Po-Vikrampur, Via-Talcher, Dist-Angul, Angul Orissa-759106, Ph: 06760-262626, Mb: 9437665821. 4 150028 Kendriya Vidyalaya, NTPC, Koniha, P.O. - Deepshikha, Distt.-Angul. Orrisa - Angul 759147. Ph.No. 06760-243658, Fax : 243658,MOB:9937616275 5 150140/410097 Govt.(SSD) Higher Sec. School, At/Po-Malpada, Via-H.S.Road, Dist-Balangir, Balangir Orissa, Mob:9437917452. 6 150059/410021 Govt. High School(SSD), At-Rampur, Block-Agalpur, Tehsil-Loisingha, Dist- Balangir Balangir, Orissa-767021, Mob:9937485942,9439225778,9438283911 7 150058/410020 Govt. High School(SSD), At-Desil, Block/Tehsil-Titlagarh, Dist-Balangir, Orissa- Balangir 767033, Mob:9658253599,9437429416 8 150139/410096 Govt.(SSD) Girls High School, At/Po-Saintala, Dist-Balangir, Orissa, Mob: Balangir 9437429188. 9 150026 Shree Dadiji Mandir Trust, Prabhavati Public School, At Pipalpadar, Dist. Balangir Balangir, Orissa - 767033 Phone No 06655 220272 10 150032 Oriental Public School, At/PO Malamunda, Distt. Bolangir - 767002, Ph. No. Balangir 06652-230025, 09437223303 11 150096/410052 Govt.(SSD) Girls Higj School, At/Po-Tenda, Via-Sajangarh, Dist-Balasore, Balasore Orissa, Mob::9668222895, 9937302394. 12 150097/410053 Govt. High School, At/Po-Kabatghati, Via-Hatigarh, Dist-Balasore-756033, Balasore Orissa. -
Angul Range for Tax Audit During 2011-12
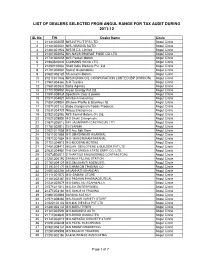
LIST OF DEALERS SELECTED FROM ANGUL RANGE FOR TAX AUDIT DURING 2011-12 SL No. TIN Dealer Name Circle 1 21131302055 M/S.NTPC/TTPS LTD Angul Circle 2 21141302001 M/S.JAMUNA AUTO Angul Circle 3 21461301922 M/S M.C.L Limited Angul Circle 4 21401302052 M/s.NAVA BHARAT FUSE CO LTD. Angul Circle 5 21741302059 M/S Parbati Motors Angul Circle 6 21983500044 CUMMINS INDIA LTD Angul Circle 7 21292100083 Shell India Markets Pvt. Ltd Angul Circle 8 21701302081 Samal Automobiles Angul Circle 9 21621302125 Shuvlaxmi Motors Angul Circle 10 21211311032 M/S.INDIAN OIL CORPORATION LIMITED(IBP DIVISION) Angul Circle 11 21961304363 S.R Traders Angul Circle 12 21581302632 Saha Agency Angul Circle 13 21721305950 Aryan Energy Pvt Ltd. Angul Circle 14 21891308039 Spectrum Coal & power Angul Circle 15 21571304820 Amritesh industries Angul Circle 16 21851309807 Bhuvee Profile & Stainless ltd Angul Circle 17 21871302133 Baba Gangaram Foods Products. Angul Circle 18 21031304729 Nilaya Enterprises Angul Circle 19 21521302083 M/S Samal Motors (P) Ltd. Angul Circle 20 21021305850 M/S Shakti Enterprisetrs Angul Circle 21 21871306013 JAY JAGANNATH CASTING (P) LTD Angul Circle 22 21781302813 S.N SARMA Angul Circle 23 21021311088 M/S Anu Rbk Store Angul Circle 24 21611301888 M/S UMASANKAR AGARWAL Angul Circle 25 21971301884 M/S- MANGTURAM RATANAL Angul Circle 26 21751304915 M/S-MODERN MOTERS Angul Circle 27 21481308410 MILLAN DEVLOPERS & BUILDER PVT LTD Angul Circle 28 21631304981 THE DM ORISSA STATE SUPP. CO. LTD. Angul Circle 29 21073500011 S.THARTIUS ENGINEERING CONTRACTORS Angul Circle 30 21281306192 SARALIA FILLING STATION. -

Grid Substations
EHV SUBSTATIONS WITH MVA CAPACITIES Year of Sl. No. Name of Substation District Installed Capacity (MVA) Commissioning 400/220kV 2x315 MVA, 400/220 kV 2005 (400 kV) 1 Meramundali Angul 3x100 MVA, 220/132 kV 2002 (220 kV) 1x12.5 MVA, 132/33 kV 2x315 MVA, 400/220 kV 2010 (400 kV) 2 Mendhasal Khurda 1x20, 220/33kV 2008 (220 kV) 3 New Duburi Jajpur 2x315 MVA, 400/220kV 2005 220/132/33kV 2x160 MVA, 220/132 kV 1996 (220 kV) 1 Balasore Balasore 2x63+1x40 MVA, 132/33 kV 1981 (132 kV) 3x100 MVA, 220/132 kV 2008 (220kV) 2 Bhadrak Bhadrak 2x63+1x40 MVA, 132/33 kV 1983 (132kV) 2x160 MVA, 220/132 kV 3 Bhanjanagar Ganjam 1984 1x40+1x16 MVA, 132/33 kV 1x160+2x100 MVA, 220/132 kV 2004 (220 kV) 4 Bidanasi Cuttack 2x63+1x40 MVA, 132/33 kV 1993 (132 kV) 2x160 MVA, 220/132 kV 5 Budhipadar Jharsuguda 1995 1x20+1x12.5 MVA, 132/33 kV 2x160+2x100 MVA, 220/132 kV 6 Chandaka Khurda 1989 2x63+1x40 MVA, 132/33 kV 3x100 MVA, 220/132 kV 7 Duburi Jajpur 2x40 MVA, 220/33 kV 1989 1x5 MVA, 132/33 kV 2x160 MVA, 220/132 kV 8 Jayanagar Koraput 1980 2x20+1x12.5 MVA, 132/33 kV 3x100 MVA, 220/132 kV 9 Joda Keonjhar 1959 1x40+3x20 MVA,132/33 kV 2x100 MVA, 220/132 kV 2007 (220 kV) 10 Katapali Sambalpur 1x40+2x20 MVA, 132/33 kV 2004 (132 kV) 11 Lapanga Sambalpur 2x160 MVA, 220/132 kV 2014 2x160 +1x100MVA, 220/132 kV 12 Narendrapur Ganjam 1999 2x40+1x20 MVA, 132/33 kV 2x160 MVA, 220/132 Kv 13 New Bolangir Bolangir 2010 1x12.5 MVA, 132/33 kV 1x160+1x100+1x50 MVA, 220/132 kV 2009 (220 kV) 14 Paradeep Jagatsinghpur 2x20+1x12.5 MVA, 132/33 kV 1981 (132 kV) 15 Tarkera Sundargarh 4x100 -

Lws. BHARAT KUMAR SAHOO €> (Consultant Electricat Engineer & Contractor) *
Mob. i 787309079S / 06760 ,277799 lWs. BHARAT KUMAR SAHOO €> _ (Consultant Electricat Engineer & Contractor) *. lP\ (An tSO 9oo1 : 2008 Cerrified) g _ AUPo.A/ia. : Rengali Dam Site, Dist. :Angul (Odisha) - 759105- - - E-mail : [email protected] - 25t9gt2015 na: rv".9113113-i9? Date To The Managing Oirector, Odisha Knowledge Co.poralion Ltd_, Bhubaneswar. Subject: Verification report of ICT lab Dear Sir, We are a registered conlladot Mls-Bharat Kumar Sahoo, an approved Electrical contractor of Governmenl of Odisha, bearing Lic€nce No. 21S8(HTXCopy of tidnse is enctosed) for your kind perusal. After verification of the following items of the ICT lab KUNLaM HtcH scHooL KUNAM, UDISE Code- 211507_14501 Elock-Pallahara, District-Angul, as per the minimum specification mentioned below, the report for the same is treing attached. S.. M i nihu m Specificati o ns Quantity Copp€. phte eanhing sbtions making eadhing phte Eam,ng (as per lS copp€, eadi 1 6@ r "rih mh 600 mm r 3 m lnid i.dud'ng tunmt, cha@Ucoke, sa[. 1 s A- 240 V swnches (tnduding Switch Soad) 15+9=24 5 in I 5\ and 1tq Socl€b 19+1:20 15 A 240 V sodet with - shdtd 1 Switches and 2 l.1di€ti€ alan6: - Arc,lor / tiavetb / sockels (lsl Ma*) cr:blrc /Wpro /PhittE / Logrand (pt6 ticU Swicies and soateb b lo be provdcd bt all ebcton'c6lT .qu'p.Ent lnctuding po.ter a.d pqecton system to be pleed al hb t6.inEian t bb Pvc conduis iocruding nasrGlboiEJliiiiEl!66iEbeGerea= 3nd propedy dahped. Widng'nsulaled porer 3 Wirins (lsl Mark) lor 5 and 15A ouueG wnh 4 squ.re mn pVC insutated srran<re<, @oer @ndudd s,E Eanhing of 3{ pin with PvC insulated qEen colo, 2 5 square mm clpper wire Name & Sig pAN : AeEpS9899p, TtN :2't241307669, Civit (L) - .t6808 EPF : 16036, S.Tax - AeEpSggggpSOOO2, ESI - 440001'16440001099, Etect. -

Dist- Rayagada
Dist- Rayagada The Data Base for the Post of Health Worker (F) HSC (20%) ( +2) ( 30%) ANM Course 50% 20 30 % 50 ANM< Catag Age AS ON Percentag Marks Marks Total SL No Name of the candidate Fathers/ gurdian Name Address SEX Date of Birth Full Marks Percenta Full Percentage Full Percentag Percentage Registratio Remarks ories 30.06.2020 e out of Secur Percentage Secure Mark Email ID Phone Number Marks Secured ge Marks out of Marks e out of n Number Percentag ed d Percentage Percentage e NO ONC archanapanda333 REGISTRATION 1 ARCHANA PANDA BHASKAR PANDA GOUDA SAHI,DURGI,RAYAGADA F UR 1/7/1992 6/30/2020 28 Y 5 M 750 409 54.533 10.907 600 340 56.667 17.000 1400 1110 79.286 39.643 Registratio 67.55 9439141872 NO. NOT n @gmail.com SUBMITTED MARKSHEET DUMBAGUDA chandinisabar990@ 2 CHANDINI SABAR JAGABANDHU SABAR F ST 6/20/1994 6/30/2020 26 Y 0 M 600 0 0.000 0.000 600 0.000 0.000 1400 0.000 0.000 22707 0.00 6371168364 NOT COLONY,ASADA,GUDARI,RAYAGADA gmail.com SUBMITTED sujatamishal@gmai 3 SUJATA KUMARI MISAL KAMAL MISAL KHILLAPADAR,PADMAPUR,RAYAGADA F UR 2/15/1988 6/30/2020 32 Y 4 M 750 300 40.000 8.000 900 334 37.111 11.133 1400 1023 73.071 36.536 32129 55.67 7205771118 l.com KUNJABIHARI 4 SURABHI KANSABEHERA BABULI NAGAR,GUNUPUR,RAYAGADA F SEBC 5/3/1998 6/30/2020 22 Y 1 M 600 296 49.333 9.867 600 234 39.000 11.700 1400 1059 75.643 37.821 28552 59.39 8117892424 KANSABEHERA LIMAPADAR,UKKAMBA,GUNUPUR,RAYA arjun.panda2@gma 5 JHARANA PANDA SUNANDA PANDA F UR 6/16/1988 6/30/2020 32 Y 0 M 750 323 43.067 8.613 900 342 38.000 11.400 1400 1070 76.429 38.214 -

Office of the Commissioner of Commercial Taxes: Orissa: Cuttack
OFFICE OF THE COMMISSIONER OF COMMERCIAL TAXES: ORISSA: CUTTACK. No._______________/CT., Date._________________ III (III) 32/2007 NOTIFICATION In exercise of the powers conferred by sub-rule (7) of Rule 4 of the Orissa Value Added Tax Rules, 2005, I Sri Aditya Prasad Padhi, I.A.S, Commissioner of Sales Tax, Orissa, Cuttack do hereby assign the records of the dealers under the jurisdiction of Cuttack II Range, Cuttack to the Large Taxpayers’ Units (LTUs) constituted in the said Range vide Finance Department Notification No.54102/F dt. 02.12.2005 as per the list below. This Notification is effective from 02.12.2005 i.e. the date of constitution of the said unit or the registration of such dealer under the Orissa Value Added Tax Act, 2004 whichever is later. Large Taxpayers’ Unit (LTU) –I Sl No. Name and Address of the dealers Tax Payers’ Identification Number (TIN) 1. M/s. Agarwalla Spices & Food, Jagatpur, Industrial 21571301328 Estate, Jagatpur. 2. M/s. Asian Paints India Ltd. Co. Telengapentha, Cuttack. 21741300022 3. M/s. Bajrangbali Alloys, Choudwar, Manguli, Cuttack. 21471300704 4. M/s. Balmer Lawrie & Co. Limited, Plot 168, Industrial 21931300742 Estate, Jagatpur. 5. M/s. Dhruba Industries, Bhairpur, Jagatpur, Cuttack. 21561300897 6. M/s. Eastern Foods, N.I.E., Jagatpur, Cuttack. 21741300798 7. M/s. Eastern Foods Pvt. Ltd. N.I.E, Jagatpur, Cuttack. 21651300799 8. M/s. Eastern Roller Flour Mill (P) Ltd., N.I.E, Jagatpur, 21561300800 Cuttack. 9. M/s. Emcure Pharmaceuticals, C/o- Santuka Associates, 21681301704 Pratapnagari, Cuttack. 10. M/s. Eveready Industries India Ltd., Bhanpur, Gopalpur, 21141100726 Cuttack.