Klippel-Feil Anomaly with Associated Rudimentary Cervical Ribs in a Human Skeleton: Case Report and Review of the Literature
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Klippel-Feil Syndrome and Thoracic Outlet Syndrome
Neurological Disorders & Epilepsy Journal Open Access Clinical Image Klippel-Feil Syndrome and Thoracic Outlet Syndrome Ali Rıza Sonkaya1*, Erkan Kaya2, Serdar Firtina3 and Mehmet AK4 1Department of Neurology, Okmeydam Training and Research Hospital, Turkey 2Department of Physical Medicine and Rehabilitation, Rehabilitation Hospital, Turkey 3Department of Cardiology, Cyprus Military Hospital, Turkey 4Department of Radiology, Ilker Celikcan Physical Medicine and Rehabilitation Hospital, Turkey A R T I C L E I N F O CLINICAL IMAGE Article history: Received: 08 September 2017 Klippel–Feil Syndrome (KFS) is a rare disease that was firstly described in Accepted: 12 October 2017 Published: 18 October 2017 1912 by Maurice Klippel and Andre Feil. It is a bone disorder recognized by the abnormal fusion of two or more spinal bones, it seem in the cervical Copyright: © 2017 Sonkaya AR et al., vertebrae. It has three major features which are short neck, limited age of Neurol Disord Epilepsy J This is an open access article distributed motion in the cervical spine and low hairline at the beck [1]. under the Creative Commons Attribution License, which permits unrestricted use, We report the case of a 26-year-old male patient was admitted to distribution, and reproduction in any medium, provided the original work is cardiology clinic with complaint of left arm and chest pain. Mitral valve properly cited. prolapse detected by transthoracic echocardiography. Patient was referred to Citing this article: Sonkaya AR, Kaya E, Firtina S, Mehmet AK. Klippel-Feil physical therapy and rehabilitation clinic due to cervical scoliosis and the short Syndrome and Thoracic Outlet Syndrome. Neurol Disord Epilepsy J. -

Download PDF File
Folia Morphol. Vol. 77, No. 2, pp. 386–392 DOI: 10.5603/FM.a2017.0080 O R I G I N A L A R T I C L E Copyright © 2018 Via Medica ISSN 0015–5659 www.fm.viamedica.pl Incidental imaging findings of congenital rib abnormalities: a case series and review of developmental concepts A.M. Aignătoaei1, C.E. Moldoveanu2, I.-D. Căruntu3, S.E. Giuşcă3, S. Partene Vicoleanu3, A.H. Nedelcu3 1Department of Pathology, “Sf. Spiridon” Clinic Hospital, 1, Independenţei Square, Iaşi, Romania 2Department of Radiology, Pneumology Clinic Hospital, 30, dr. Iosif Cihac Street, Iaşi, Romania 3Department of Morphofunctional Sciences, “Grigore T. Popa” University, 16, University Street, Iaşi, Romania [Received: 12 June 2017; Accepted: 24 July 2017] Background: Congenital rib abnormalities are found in approximately 2% of the general population. Usually, they occur in isolation and are rarely symptomatic, but they can also be associated with other malformations. Materials and methods: We reviewed imaging examinations performed over a period of 2 years (2014–2015), enabling us to identify isolated rib abnormalities in 6 adult patients. Results: The case series consisted in 3 cases with bilateral cervical ribs and 1 case each with bifid rib, costal fusion and rib pseudarthrosis. In all patients, the costal anomalies were discovered incidentally. All rib malformations were detected at thoracic radiography, except for the rib pseudarthrosis, which was identified at computed tomography (CT) scan. Differential diagnosis was made between cer- vical ribs and abnormalities of the C7 transverse process and of the first rib, while the other costal malformations were distinguished from tumoural, traumatic or inflammatory lesions of the chest wall, lung and pleura. -

A Narrative Review of Poland's Syndrome
Review Article A narrative review of Poland’s syndrome: theories of its genesis, evolution and its diagnosis and treatment Eman Awadh Abduladheem Hashim1,2^, Bin Huey Quek1,3,4^, Suresh Chandran1,3,4,5^ 1Department of Neonatology, KK Women’s and Children’s Hospital, Singapore, Singapore; 2Department of Neonatology, Salmanya Medical Complex, Manama, Kingdom of Bahrain; 3Department of Neonatology, Duke-NUS Medical School, Singapore, Singapore; 4Department of Neonatology, NUS Yong Loo Lin School of Medicine, Singapore, Singapore; 5Department of Neonatology, NTU Lee Kong Chian School of Medicine, Singapore, Singapore Contributions: (I) Conception and design: EAA Hashim, S Chandran; (II) Administrative support: S Chandran, BH Quek; (III) Provision of study materials: EAA Hashim, S Chandran; (IV) Collection and assembly: All authors; (V) Data analysis and interpretation: BH Quek, S Chandran; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: A/Prof. Suresh Chandran. Senior Consultant, Department of Neonatology, KK Women’s and Children’s Hospital, Singapore 229899, Singapore. Email: [email protected]. Abstract: Poland’s syndrome (PS) is a rare musculoskeletal congenital anomaly with a wide spectrum of presentations. It is typically characterized by hypoplasia or aplasia of pectoral muscles, mammary hypoplasia and variably associated ipsilateral limb anomalies. Limb defects can vary in severity, ranging from syndactyly to phocomelia. Most cases are sporadic but familial cases with intrafamilial variability have been reported. Several theories have been proposed regarding the genesis of PS. Vascular disruption theory, “the subclavian artery supply disruption sequence” (SASDS) remains the most accepted pathogenic mechanism. Clinical presentations can vary in severity from syndactyly to phocomelia in the limbs and in the thorax, rib defects to severe chest wall anomalies with impaired lung function. -

Some Sequels of Abnormality at the Thoracic Outlet* by J
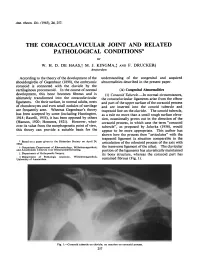
Thorax: first published as 10.1136/thx.2.1.1 on 1 March 1947. Downloaded from Thorax (1947), 2, 1. SOME SEQUELS OF ABNORMALITY AT THE THORACIC OUTLET* BY J. R. LEARMONTH Edinburgh This paper-on obstruction at the thoracic outlet-deals with the results of anomalies of bone and muscle; first rib, cervical rib, and scaleni. Though thoracic surgeons approach these structures from a different exposure, and with a different end in view, they may be interested in the related types of vascular and nervous disturbance, and may like to compare them with any anomalies thev have encountered in their own operative procedures and which were possibly not associated with clinical symptoms. MORPHOLOGY N~~~~~~~~~~~~~~~~~~~~~~~~1 http://thorax.bmj.com/ The- arrangement of the bones which form the thoracic outlet derives from the typical thoracic segment (Fig. 1). This con- sists of a central piece or centrum (the body of the vertebra) carrying a dorsal and a ventral hoop of bone. The dorsal hoop (neural arch) provides the laminae and spinous process. The central piece or centrum may be defective as on October 3, 2021 by guest. Protected copyright. to one half (hemivertebra), producing both scoliosis and absence of one rib, which inevit- ably alter the architecture of the thoracic out- let on both sides; or it may be fused with adjoining central pieces. The ventral hoop, or haemal arch, is much expanded in the thor- acic region. The haemal arch has a double origin, from a dorsal segment of bone, the pleurapophysis, and a ventral segment, the FIG. 1.-Typical thoracic segment *An address to the Society of Thoracic Surgeons (Owen). -

Ultrasonographic Screening for Fetal Rib Number Anomalies
Original Article Hong Kong J Gynaecol Obstet Midwifery 2020;20(2):81-7 | https://doi.org/10.12809/hkjgom.20.2.08 Ultrasonographic screening for fetal rib number anomalies Florrie NY YU, MBChB, MRCOG, FHKAM (Obstetrics and Gynaecology) Teresa WL MA, MBBS, FRCOG, FHKAM (Obstetrics and Gynaecology) Department of Obstetrics and Gynaecology, Queen Elizabeth Hospital, Hong Kong Objective: To determine associations between fetal rib number anomalies detected on ultrasonography and chromosomal anomalies and other structural anomalies, and the outcome of affected pregnancies. Methods: All cases of fetal rib number anomalies referred to the Prenatal Diagnosis Clinic of Queen Elizabeth Hospital between 1 January 2016 and 31 December 2019 were reviewed. Fetal ribs were examined by static three- dimensional multiplanar or volume contrast ultrasonography. Genetic counselling was offered. The prenatal and postnatal records were reviewed. Results: 21 fetuses with rib number anomalies were identified over 4 years. The most common presentation was unilateral or bilateral absence of the 12th thoracic rib (n=12, 57.1%), followed by the presence of lumbar rib (n=6, 28.6%) and the presence of cervical rib (n=3, 14.3%). Three (14.3%) fetuses were identified to have anomalies in other systems: unilateral absence of nasal bone (n=1) and minor vascular anomalies (n=2). One patient with multiple anomalies of the fetus underwent amniocentesis, and the chromosomal microarray analysis was normal. Postnatally, 13 babies had chest radiographs taken. Two were confirmed to have normal number of ribs. Prenatal and postnatal findings were consistent in 6 (46.2%) babies. Conclusion: Fetal rib number anomalies were an isolated finding in most cases. -

Missed Cervical Ribs Alter Pain Management in Thoracic Outlet Syndrome
® Radiology Rounds Missed Cervical Ribs Alter Pain Management in Thoracic Outlet Syndrome By James D. Collins, MD his 47-year-old, right-handed female physical therapist was Radiographic Findings referred by a neurologist for bilateral magnetic resonance T imaging (MRI) of her brachial plexus. The referring neu- rologist indicated the patient developed tingling, numbness, and pain in her right arm with right occipital headache following a whiplash injury she sustained on a roller coaster. Thereafter, she reportedly underwent transaxillary resection of her right first rib for right thoracic outlet syndrome (TOS). After the surgery, the patient suffered persistent pain in her right shoulder and hand, and then 4 months later, she underwent right supraclavicular anterior scalene and middle scalenectomy. Although she received multiple treatments — including Botox in- jections, physical therapy, and myofascial release of the intercostal muscles — she continued to experience pain and numbness in her right arm that interfered with her work. One-and-a-half years later, the patient underwent right pectoralis minor tenotomy and neurolysis of the right brachial plexus, but again without relief. Subsequently, the following chest radiograph and bilateral MRI, magnetic resonance angiography (MRA), and magnetic resonance veinography (MRV) of the brachial plexus were obtained. Figure 1 This posterior-anterior (PA) chest radiograph displays sharp margination of the right sternocleidomastoid muscle (STM) atrophy of the right trapezius muscle (TRP) as compared -

A Study of Sacralisation of Fifth Lumbar Vertebrae in Saurashtra Region
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article A Study of Sacralisation of Fifth Lumbar Vertebrae in Saurashtra Region Zaveri KK1*, Talsaniya D1*, Singel TC2**, Patel MM2* 1Tutor, 2Professor and Head, *M.P.Shah Government Medical College, Jamnagar, Gujarat. **B.J. Medical College, Ahmedabad, Gujarat. Corresponding Author: Dhaval Talsaniya Received: 25/06/2015 Revised: 15/07/2015 Accepted: 17/07/2015 ABSTRACT The present study was done to study the Incidence of sacralisation of fifth lumbar vertebrae in Saurashtra region. In modern life backache is common complaint. One of the causes is Sacralisation of lumbar vertebra. Sacralisation means addition of sacral elements by the incorporation of fifth lumbar vertebra. In Sacralisation of fifth lumbar vertebra, the transverse process of fifth lumbar vertebra (L5) becomes larger than normal on one or both sides, and fuses to the sacrum, or ilium and or both. In the present study 96 dry human sacra of Saurashtra region, 68 male & 28 female were studied. It was found that typical sacrum consisting of five segments in 85 (88.5%) specimens, while sacralisation of fifth lumbar vertebrae was seen in 11 (11.5%) sacra. Out of 11 cases 8(11.7%) were of male and 3 (10.7%) were of female sacra. Sacralisation of fifth lumbar vertebrae is well-known anomaly of Lumbosacral spine and is associated with low backache, disc herniation and with cervical rib. So, Knowledge of Sacralisation is not only useful for the orthopaedic surgeons, but also vital for the clinical anatomist, radiologists, forensic experts and morphologists. -

'Cervical Rib' and Its Association with Gender, Body Side, Handedness and Other Thoracic Bony Anomalies in a Population of Central India
Indian Journal of Basic and Applied Medical Research; March 2014: Vol.-3, Issue- 2, P.593-597 Original article: Prevalence of 'Cervical Rib' and its association with gender, body side, handedness and other thoracic bony anomalies in a population of Central India DK Sharma, Vishnudutt, Vandana Sharma, Mrithunjay Rathore Name of the Institute/college: Department of Anatomy , All India Institute of Medical Sciences (AIIMS), Raipur, Chhattisgarh, India Corresponding author: Dr. DK Sharma ; Email id: [email protected] Abstract Objectives of this study were to see the prevalence of cervical rib in people of Central India and its association with gender, body sides, handedness and other thoracic bony anomalies; and correlate with the studies already reported. Total 5000 consecutive plain radiograms of chest of patients (2500 males and 2500 females directed by various departments) were examined in the Department of Radiology, Pt. J. N. M. Medical College, Raipur during January to September 2013. Skiagrams of persons below 15 years of age, belonging outside the Central India and with obvious pathology obstructing the bony shadows to be examined, were excluded from the study. We found 61(1.22%) persons with cervical rib among 5000, out of which 22 (0.44%) bilateral and 39 (0.78%) unilateral, so statistically there was a little unilateral predominance. Overall and unilateral incidences were little more common in males (M-0.68% : F-0.54% and M-0.48% : F-0.3%) whereas bilateral incidence was little more common in females (M-0.2 : F-0.24), however these associations were statistically insignificant. Unilateral cases showed little predominance towards males and left side but statistically it was not evident. -

Differential Diagnosis of Complex Conditions in Paleopathology: a Mutational Spectrum Approach by Elizabeth Lukashal a Thesis
Differential Diagnosis of Complex Conditions in Paleopathology: A Mutational Spectrum Approach by Elizabeth Lukashal A thesis presented to the University of Waterloo in fulfillment of the thesis requirement for the degree of Master of Arts in Public Issues Anthropology Waterloo, Ontario, Canada, 2021 © Elizabeth Lukashal 2021 Author’s Declaration I hereby declare that I am the sole author of this thesis. This is a true copy of the thesis, including any required final revisions, as accepted by my examiners. I understand that my thesis may be made electronically available to the public. ii Abstract The expression of mutations causing complex conditions varies considerably on a scale of mild to severe referred to as a mutational spectrum. Capturing a complete picture of this scale in the archaeological record through the study of human remains is limited due to a number of factors complicating the diagnosis of complex conditions. An array of potential etiologies for particular conditions, and crossover of various symptoms add an extra layer of complexity preventing paleopathologists from confidently attempting a differential diagnosis. This study attempts to address these challenges in a number of ways: 1) by providing an overview of congenital and developmental anomalies important in the identification of mild expressions related to mutations causing complex conditions; 2) by outlining diagnostic features of select anomalies used as screening tools for complex conditions in the medical field ; 3) by assessing how mild/carrier expressions of mutations and conditions with minimal skeletal impact are accounted for and used within paleopathology; and 4) by considering the potential of these mild expressions in illuminating additional diagnostic and environmental information regarding past populations. -

Part I, Cervical Spine
Open Access Review Article DOI: 10.7759/cureus.8667 Anatomical Variations That Can Lead to Spine Surgery at the Wrong Level: Part I, Cervical Spine Manan Shah 1 , Dia R. Halalmeh 2 , Aubin Sandio 1 , R. Shane Tubbs 3, 4, 5 , Marc D. Moisi 2 1. Neurosurgery, Wayne State University, Detroit Medical Center, Detroit, USA 2. Neurosurgery, Detroit Medical Center, Detroit, USA 3. Neurosurgery and Structural & Cellular Biology, Tulane University School of Medicine, New Orleans, USA 4. Anatomical Sciences, St. George's University, St. George's, GRD 5. Neurosurgery and Ochsner Neuroscience Institute, Ochsner Health System, New Orleans, USA Corresponding author: Dia R. Halalmeh, [email protected] Abstract Spine surgery at the wrong level is an adversity that many spine surgeons will encounter in their career, and it falls under the wrong-site surgery sentinel events reporting system. The cervical spine is the second most common location in the spine at which surgery is performed at the wrong level. Anatomical variations of the cervical spine are one of the most important incriminating risk factors. These anomalies include craniocervical junction abnormalities, cervical ribs, hemivertebrae, and block/fused vertebrae. In addition, patient characteristics, such as tumors, infection, previous cervical spine surgery, obesity, and osteoporosis, play an important role in the development of cervical surgery at the wrong level. These were described, and several effective techniques to prevent this error were provided. A thorough review of the English-language literature was performed in the database PubMed between 1981 and 2019 to review and summarize these risk factors. Compulsive attention to these factors is essential to ensure patient safety. -
The Coracoclavicular Jointand Related
Ann. rheum. Dis. (1965), 24, 257. THE CORACOCLAVICULAR JOINT AND RELATED PATHOLOGICAL CONDITIONS* BY W. H. D. DE HAAS,t M. J. KINGMA,+ AND F. DRUCKER§ Amsterdam According to the theory of the development of the understanding of the congenital and acquired shouldergirdle of Gegenbaur (1898), the embryonic abnormalities described in the present paper. coracoid is connected with the clavicle by the cartilaginous procoracoid. In the course of normal (A) Congenital Abnormalities development, this bone becomes fibrous and is (1) Coracoid Tubercle.-In normal circumstances, ultimately transformed into the coracoclavicular the coracoclavicular ligaments arise from the elbow ligaments. On their surface, in normal adults, nests and part of the upper surface of the coracoid process of chondrocytes and even small nodules of cartilage and are inserted into the conoid tubercle and are frequently seen. Whereas Gegenbaur's theory trapezoid line on the clavicle. The conoid tubercle, has been accepted by some (including Huntington, as a rule no more than a small rough surface eleva- 1918; Ravelli, 1955), it has been opposed by others tion, occasionally grows out in the direction of the (Hanson, 1920; Hommes, 1921). However, what- coracoid process, in which case the term "coracoid ever its value from the morphogenetic point of view, tubercle", as proposed by Jaluvka (1956), would this theory can provide a suitable basis for the appear to be more appropriate. This author has shown how the process then "articulates" with the trapezoid ligament (a situation comparable to the * Based on a paper given to the Heberden Society on April 24, 1964. articulation of the odontoid process of the axis with t Outpatients Department of Rheumatology, Wilhelminagasthuis, the transverse ligament of the atlas). -

Function of the Retinoic Acid Receptors (Rars) During Development (I) Craniofacial and Skeletal Abnormalities in RAR Double Mutants
Development 120, 2723-2748 (1994) 2723 Printed in Great Britain © The Company of Biologists Limited 1994 Function of the retinoic acid receptors (RARs) during development (I) Craniofacial and skeletal abnormalities in RAR double mutants David Lohnes*,†, Manuel Mark*, Cathy Mendelsohn*,‡, Pascal Dollé, Andrée Dierich, Philippe Gorry, Anne Gansmuller and Pierre Chambon§ Laboratoire de Génétique Moléculaire des Eucaryotes du CNRS, Unité 184 de Biologie Moléculaire et de Génie Génétique de l’INSERM, Institut de Chimie Biologique, Faculté de Médecine, 11 rue Humann, 67085 Strasbourg Cedex, France *Should be considered as equal first authors †Present address: Institut de recherches cliniques de Montréal, Laboratoire de Biologie Cellulaire et Moléculaire, 110 Avenue des Pins-Ouest, Montréal, Québec H2W 1R7, Canada ‡Present address: Columbia University, Department of Physiology and Biophysics, 630 W 168th Street, New York, NY 10032, USA §Author for correspondence SUMMARY Numerous congenital malformations have been observed in abnormalities, which are reported in this and in the accom- fetuses of vitamin A-deficient (VAD) dams [Wilson, J. G., panying study. We describe here multiple eye abnormali- Roth, C. B., Warkany, J., (1953), Am. J. Anat. 92, 189-217]. ties which are found in various RAR double mutant fetuses Previous studies of retinoic acid receptor (RAR) mutant and are similar to those previously seen in VAD fetuses. mice have not revealed any of these malformations [Li, E., Interestingly, we found further abnormalities not previ- Sucov, H. M., Lee, K.-F., Evans, R. M., Jaenisch, R. (1993) ously reported in VAD fetuses. These abnormalities affect Proc. Natl. Acad. Sci. USA 90, 1590-1594; Lohnes, D., ocular glands, salivary glands and their associated ducts, Kastner, P., Dierich, A., Mark, M., LeMeur, M., Chambon, the axial and limb skeleton, and all skeletal elements P.